
Abstract
Background:
Among total cancer deaths, esophageal cancer ranks sixth in mortality. Radiotherapy and chemotherapy remain the main treatments for unresectable, locally advanced esophageal cancer, but a relapse and drug resistance are still common. The optimized choice for therapeutic schemes with low toxicity and a high quality of life is unclear when local progression occurs after radiotherapy and chemotherapy. Fluoroscopy-guided photodynamic therapy (PDT) on patients with recurrent esophageal cancer in whom the endoscope cannot pass may be used as a salvage treatment, and nanoparticle albumin-bound paclitaxel (Nab-P) has been shown to be effective for advanced esophageal cancer. The combination of PDT and Nab-P might be an effective and tolerable option for advanced esophageal cancer.
Case summary:
The authors present a 65-year-old male patient diagnosed with esophageal squamous cell carcinoma (ESCC) confirmed to have developed local progression after receiving radiotherapy and chemotherapy. Severe esophageal stenosis, mild malnutrition and anemia, and radiation pneumonia were found when he was admitted to the authors' hospital. For rapid reduction of tumor burden and to restore normal diet, he received PDT by the X-ray fluoroscopy positioning method and Nab-P chemotherapy. The patient obtained clinical benefit from these treatments, and improved his quality of life.
Conclusions:
This case demonstrates potential advantages of fluoroscopy-guided PDT combined with Nab-P in reducing the tumor load, preserving organ function, and improving the quality of life, as well as the beneficial effect on locally advanced esophageal cancer after radiotherapy and chemotherapy. This combination therapy provides an alternative for the clinical treatment of locally advanced esophageal cancer and it has broad prospects in treatment of the disease.
Core tip:
Herein, the authors report a case of a patient with ESCC who suffered locally progressive disease after chemotherapy and radiotherapy as well as malnutrition and mild anemia because of feeding difficulties. The patient was treated with PDT, which was assisted by a new positioning technique of X-ray fluoroscopy and Nab-P chemotherapy, and finally achieved clinical benefits. In addition, a modified transnasal feeding tube was also applied in the process of fluoroscopy-guided PDT in this article.
Introduction
Esophageal cancer, a common malignant tumor of the digestive tract, ranks sixth in mortality among the total cancer deaths worldwide 1 and seriously threatens human health. The incidence of esophageal cancer is related to smoking, drinking, gastroesophageal reflux, diet, obesity, body composition, and genetic factors. 2 In the locally advanced stage, the feeding ability is limited by an esophageal obstruction, which aggravates the risk and severity of malnutrition on the basis of a high tumor burden, and it significantly reduces the patient's quality of life and survival.
The early symptoms of esophageal cancer are not obvious, so most patients lose the opportunity for surgery when they initially come to the hospital. For an unresectable lesion, radiotherapy and chemotherapy are commonly used, while recurrence and local progression of esophageal cancer occur frequently due to insensitivity and resistance to treatments. Relieving the esophageal obstruction and improving nutrition and quality of life of patients are the focus of clinical work presently after chemotherapy and radiotherapy failure. Photodynamic therapy (PDT), as a minimally invasive technique of cancer therapy, is an appropriate treatment for advanced esophageal cancer. 3
PDT, with the benefits of precise targeting and low toxicity, combines a photosensitizer, oxygen, and laser light. In brief, the main mechanisms of PDT are as follows: the photosensitizers gathers in the tumor after injection, then molecular oxygen converts into reactive oxygen species (ROS) under the irradiation of laser. Ultimately, the tumor cells develop apoptosis and necrosis induced by ROS. 4 Nanoparticle albumin-bound paclitaxel (Nab-P) is known as a new taxane drug that has less of an adverse reaction and higher efficacy compared with traditional paclitaxel. 5 Recently, the chemotherapy regimen of Nab-P combined with cisplatin became the first-line therapy for esophageal cancer in China. 6
Herein, the authors report the first case of PDT in combination with Nab-P as an optional therapy for locally advanced esophageal squamous cell carcinoma (ESCC) after chemoradiotherapy. Additionally, this article aims to share a novel site-locating technique for laser radiation during PDT, especially for patients with esophageal cancer who are not suitable for endoscopic PDT.
Case Presentation
Chief complaints
A 65-year-old man was admitted to the authors' hospital in June 2019 with a chief complaint of progressive dysphagia after chemotherapy and radiotherapy for ESCC.
History of present illness
The patient was admitted to a local hospital in April 2018 due to dysphagia. An esophagogastroduodenoscopy (EGD) revealed an irregular neoplasm located 21–24 cm from the incisors and it was confirmed as ESCC by a pathological examination. A computed tomography (CT) scan showed multiple metastatic lymph nodes in the left peribronchial sulcus and around the abdominal aorta. The patient was clinically diagnosed with T3 N3 M0 stage III cancer (according to the American Joint Clinical Committee on Cancer (AJCC) staging system). 7 He received chemotherapy using docetaxel in combination with lobaplatin in April 2018. The treatment scheme was replaced with tetrafluoride, calcium leucovate and lobaplatin after the patient experienced severe adverse reactions to previous chemotherapy. Afterward, the patient received three-dimensional conformal radiotherapy of 60 Gy, which was delivered in 30 fractions, and he was evaluated as being in partial remission after radiotherapy. He then received chemotherapy using fluorouracil plus cisplatin for six cycles, and his condition turned into a stable disease. Thereafter, the patient's therapy was replaced with oral teggio, and it was maintained until he came to the authors' hospital. The patient developed progressive dysphagia in the last month of the period of receiving chemotherapy with teggio.
Physical examination and laboratory testing
There was no positive signs in his physical examination except for thin appearance. According to the laboratory testing, his hemoglobin (93 g/L) and albumin (35.6 g/L) levels were lower than the normal range. The test results of the tumor markers showed that gastrin-releasing peptide had increased (77.02 pg/mL), while AFP, CEA, and CA199 showed no significant abnormalities.
Imaging examination
The CT showed the thickness of the esophagus wall at the T4–7 vertebral level (Fig. 1A, B) and radiation pneumonia. The EGD showed that the tumor was 22 cm from the incisors, and the head of the endoscope could not pass through due to narrowing of the lesion (Fig. 2A). A metal tissue clip was marked above the upper margin of the tumor in the lining of the esophagus (Fig. 2B). To obtain a more detailed assessment of the severity of the obstruction, iodine (iohexol) contrast radiography was performed, which revealed the obstruction of the iohexol passage with a stenosis length of about 6 cm (Fig. 3A).
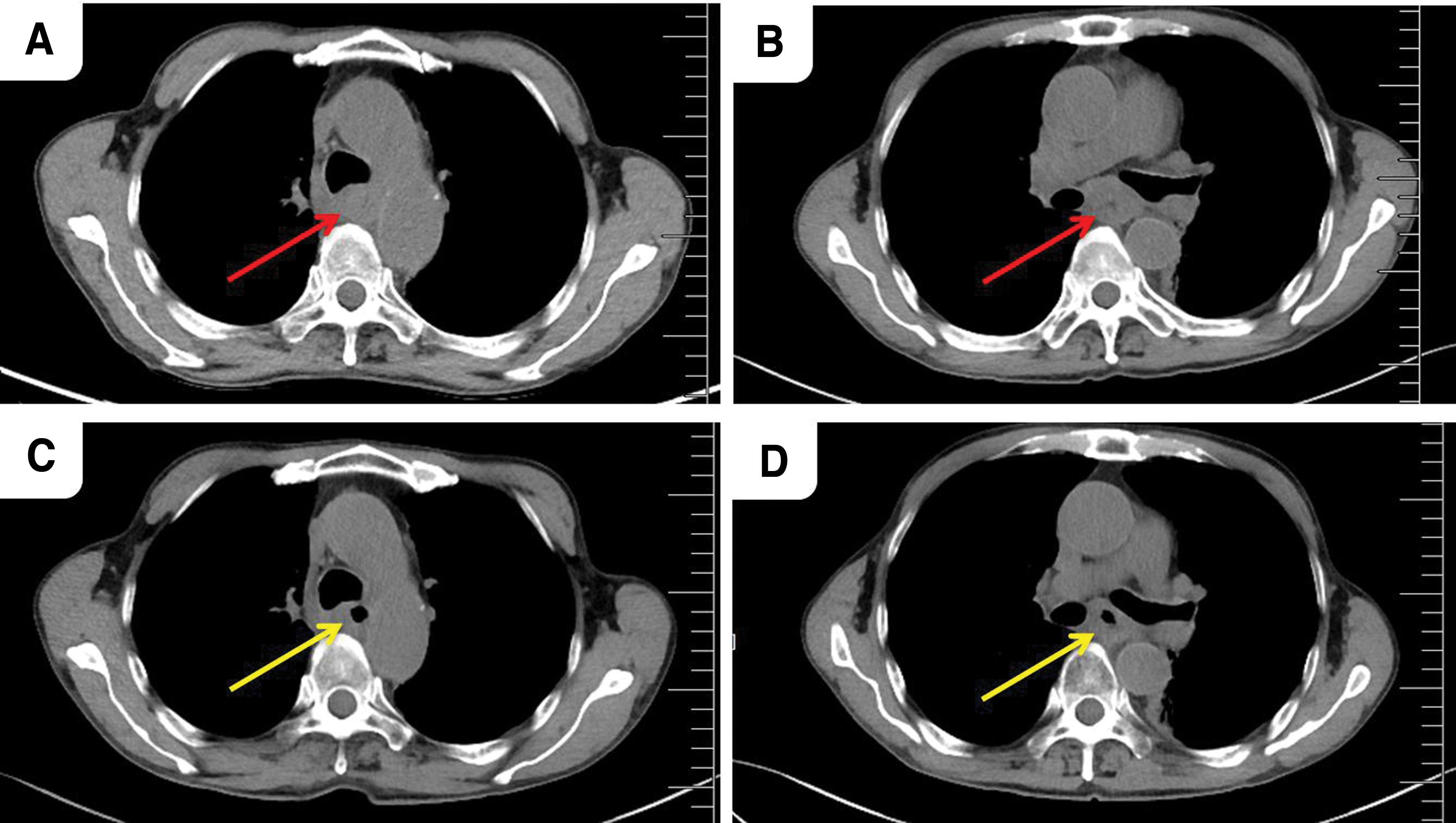
Computed tomography images.
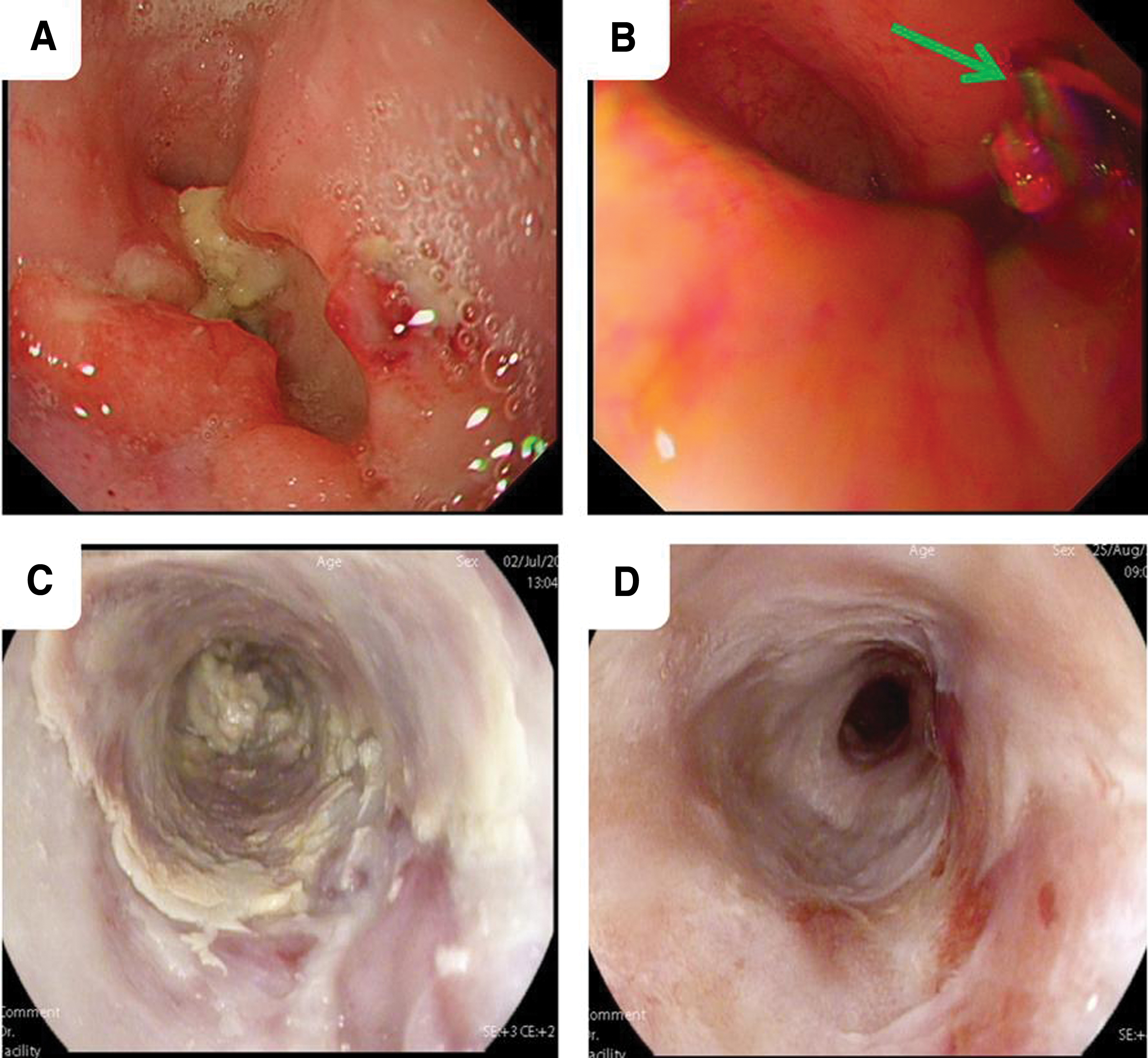
EGD images.

Contrast radiography.
Further diagnostic work-up
The tumor was confirmed to be poorly differentiated ESCC by histological examination. Immunohistochemical staining showed that the Ki67 index was >90%, with positive staining for P16, CK5/6, P63, and P40 and negative staining for CK7, CK20, and villin (Fig. 4).
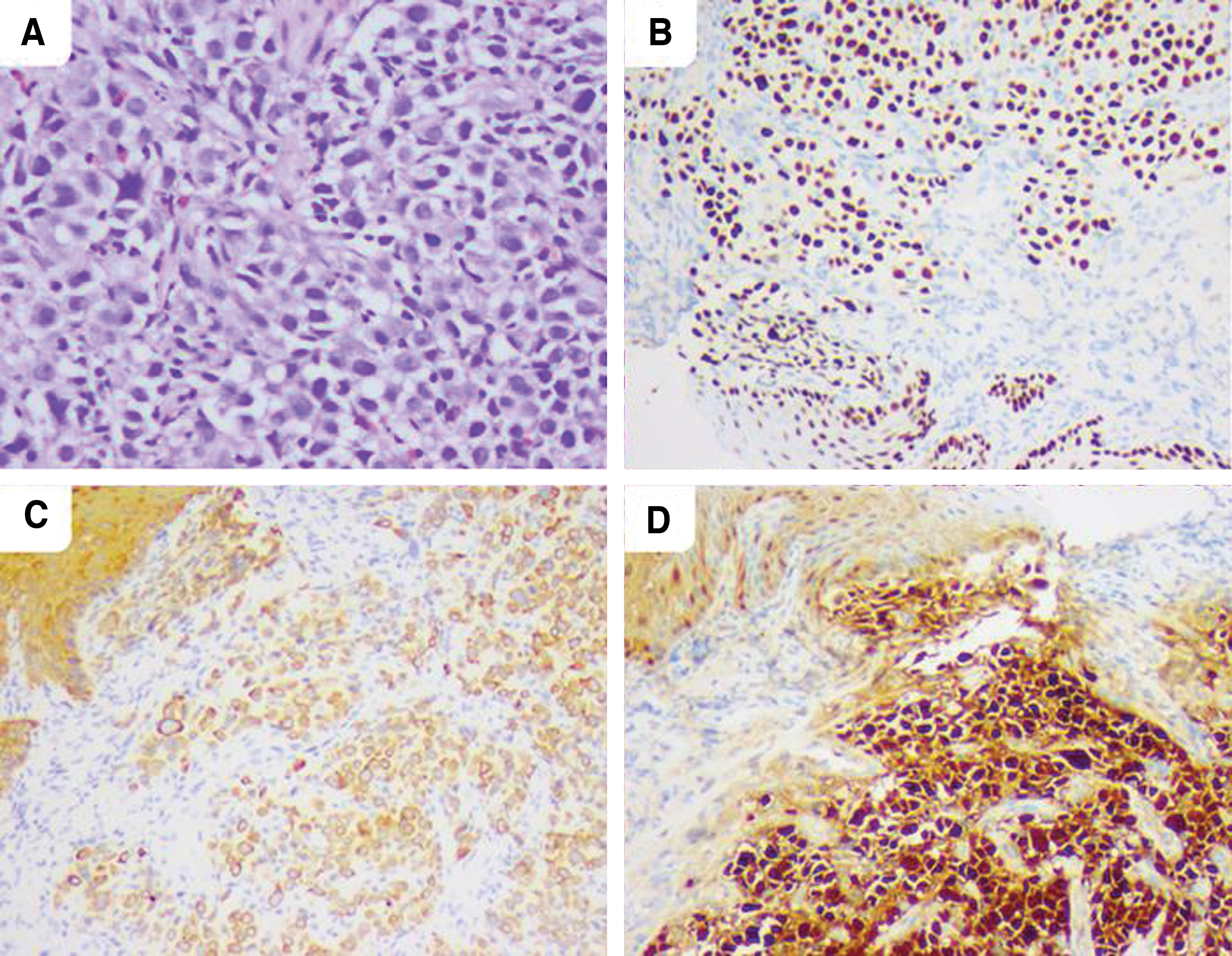
Tumor histology.
Final Diagnosis
The patient was diagnosed as having ESCC, mild anemia and hypoalbuminemia, and radiation pneumonia.
Treatment
On March 3, 2019, for the purpose of relieving the obstruction and reducing tumor load, the authors performed PDT on the patient. Twenty-four hours before laser irradiation, a photosensitizer (hematoporphyrin derivatives, HpD and Hiporfin®) was administered by intravenous infusion at a dose of 5 mg/kg. A local anesthetic on the esophageal mucosa was administered preoperatively to relieve any pain during the laser treatment. Because visualization of the positioning was not available from the EGD on account of severe esophageal stenosis, X-ray fluoroscopy was employed to locate the treatment site before the light irradiation. A laser fiber connected to PDT apparatus was used to perform irradiation (630 nm, 700 mW, for 13 min). On the tip of the fiber, the luminary had two tiny metal markers for positioning. The fiber was inserted into the irradiation areas via a modified transnasal feeding tube (MTFT). During the period of irradiation, the luminary was first placed at the lower field and then withdrawn from the upper field precisely, which aimed to treat the lesions (8 cm), including the visible tumor, for about 6 cm and 1 cm outside the tumor margin on the vertical axis. The patient had no obvious discomfort, except for mild burning pain in the esophagus during the laser irradiation. After PDT, X-ray fluoroscopy was performed to recheck the relative position of the luminary and tumor. The patient then spent 1 month avoiding sun exposure. Two weeks after the laser irradiation, the patient received Nab-P chemotherapy (240 mg/m2 on day 1 Q3W) for three cycles, with no allergic reaction and severe adverse reactions to the chemotherapy.
Outcome and Follow-Up
Two weeks after PDT, EGD was performed for observation of efficacy and debridement, in which the endoscope equipment could safely pass through the obstructed region, and it showed a large amount of necrosis tissue in the laser irradiation area of the esophagus (Fig. 3B). The chest CT showed that lesions of the tumor decreased in the area of light irradiation (Fig. 1C, D). The diluted barium esophagography showed that the stream of contrast in the esophageal lumen was more expedited than before (Fig. 3B). The laboratory examination showed that the concentration of hemoglobin (108 g/L) and albumin (39.3 vg/L) had increased after the treatment and the tumor marker, gastrin-releasing peptide precursor, was reduced to 52.05 pg/mL. EGD was used to monitor changes in the treatment site during the follow-up period, in which the necrotic tissue gradually decreased and was replaced by scar tissue (Fig. 2D). The patient returned to a normal diet within 1 month and is still alive with a high quality of life.
Discussion
Globally, morbidity and mortality rates of esophageal cancer are the highest in China, 1 which closely relate to diet, genes, and region conditions. The symptoms of early esophageal cancer are not obvious, and most patients have already developed progressive esophageal cancer by the time they visit the doctor, with severe difficulty in swallowing, so some of them lose their chance of undergoing surgery. As for unresectable esophageal cancer, targeted and immune therapy has achieved great success in recent years. 8 –10 However, radiotherapy and chemotherapy are still the main treatment methods. Reradiotherapy can significantly benefit patients who develop recurrence or local progression after chemotherapy and radiotherapy, but they have to accept the risks of increasing side-effects and radiation exposure. 11
More critically, the relapse of esophageal stenosis by radiotherapy is a slow process. At this point, choosing superior treatment strategies with better safety and efficacy is an important issue for clinicians. Clinical studies indicated that PDT was a salvage treatment for use after chemotherapy and radiotherapy failure for esophageal cancer. 12,13 PDT, a minimally invasive treatment with low toxicity and precise targeting, is often used in the treatment of gastrointestinal tumors using an endoscopic technique. 14,15
In this case, the patient underwent local progression after receiving chemotherapy and radical radiotherapy for esophageal cancer. He was limited to fluid food and suffered anemia and malnutrition caused by severe esophageal stenosis. Considering the presence of radiation pneumonia, reradiotherapy might not reach a radical cure dose or resolve the obstruction in the short term. In the meantime, the risk of adverse effects might increase. In addition, the patient refused surgery and endoscopic resection. In which case, to recover his ability to eat and improve the status of nutrition as soon as possible, the PDT was applied to this patient. Meanwhile, taking the patient's adverse reaction to previous chemotherapy into account, chemotherapy with Nab-P was used to treat his cancer.
However, there are no direct clinical data to guide the precise timing for systemic chemotherapy with Nab-paclitaxel after PDT. To prevent recurrence after PDT and considering the patient's tolerance to combination therapy, Nab-paclitaxel was applied 2 weeks after PDT. CT (Fig. 1C, D) and continuous EGD (Fig. 2C, D) revealed the recanalization of the esophageal lumen and a decrease in tumor volume during the follow-up. One week after PDT, the patient began to have semiliquid food, and then solid food was introduced in his diet 2 weeks later. Finally, the patient resumed a normal diet, and his anemia and nutritional status improved within a month. With his improved nutrition level, he was able to perform general physical activity 2 months later.
No allergic reaction or cutaneous photosensitivity was found after PDT, and there was no abnormality in his liver or kidney functions throughout the course of the treatment. The clinical results shown above demonstrate that the combination of PDT and Nab-P chemotherapy might be an optional treatment method for advanced ESCC, with favorable safety and significant efficacy.
For a long time, PDT in the treatment of esophageal cancer commonly draws support from the endoscope technique, mainly a painless endoscopic procedure. 16 –19 Precise positioning, real-time visualization, and facilitation of laser irradiation are integrated into the advantages of endoscope-mediated PDT, owing to the fiber being carried to the tumor through the accessory channel of the endoscopic device. Moreover, avoiding pain during laser irradiation is one of the advantages of a general anesthetic. 20 More importantly, the application of a general anesthetic for patients with esophageal cancer can obviously alleviate vomiting and a stress reaction; therefore, maintenance of the precise positioning could be easily implemented by a doctor during the treatment.
However, a painless endoscopic procedure is not appropriate for some elderly patients with severe underlying diseases. Moreover, for patients with severe esophageal stenosis, an endoscopic procedure may fail to provide a clear view of the far end of the narrow section, thus precise positioning may be affected. In this case, the EGD examination before PDT showed that the endoscopic equipment could not successfully pass through the stenosis of the esophagus. X-ray fluoroscopy was then used for positioning instead of endoscopy. Simultaneously, an MTFT was applied to assist the fiber that entered into the stenosis area. After the nonendoscope-assisted approach was chosen, the patient was treated in a supine position on the examination couch of the X-ray fluoroscopy equipment.
To reduce the risk of aspiration due to vomiting during the PDT when the patient was in the supine position, the general anesthetic was replaced with a surface anesthetic with oxybuprocaine hydrochloride gel before irradiation. According to the response of the patient during the PDT, he experienced only a slight burning sensation and had no other discomfort. This might be because the gelatinous anesthetic can better adhere to the esophageal surface and release the anesthetic slowly, which provided a satisfactory anesthetic effect throughout the treatment. In the X-ray fluoroscopy positioning, the relative distance between the metal tissue clip (Fig. 2B) and the metal markers on the luminary of the fiber was measured on a digital imaging system, and the location of the luminary was adjusted to the predesigned treatment site.
After the positioning, to minimize the impact on positioning from the patient's speaking, the patient was instructed to stay quiet. During irradiation, the patient's response was monitored in real time and he responded to the questions that were asked with a prerehearsed gesture. After irradiation, the relative position of the luminary and tumor was rechecked by X-ray fluoroscopy, which showed no obvious signs of the luminary shifting. The accuracy of positioning with this locating approach was clearly demonstrated by results of both the rechecked X-ray fluoroscopy on the digital imaging system and the range of inflammatory changes on EGD examination after PDT (Fig. 2C, D).
Studies have shown that the rate of tumor necrosis after PDT treatment is higher than that after radiotherapy. 21,22 However, PDT has a high recurrence rate. The combination therapies of PDT and other noninvasive therapies, such as radiotherapy, chemotherapy, and immunotherapy, have been widely used as effective nonsurgical strategies for advanced esophageal cancer. 22 –24 Compared with PDT alone in the field of esophageal cancer treatment, some combination therapies can significantly reduce the postoperative recurrence rate of PDT. Therefore, for patients with advanced, inoperable esophageal cancer, combination therapies based on PDT are an alternative option to reduce the postoperative recurrence rate and improve their quality of life.
To the best of the authors' knowledge, this article reported a case of PDT combined with the sequential treatment with Nab-P chemotherapy for the first time. PDT combined with taxanes may have a magnificent clinical prospect in the treatment of esophageal cancer. Experimental studies have shown that PDT combined with paclitaxel has a synergistic inhibitory effect on proliferation of the human esophageal cancer cell line, Eca-109, and it induces apoptosis. 25 As a novel taxane drug, Nab-P can be engulfed by tumor cells by facilitation of an albumin molecule, which binds to SPARC, 26 and paclitaxel molecules loaded on albumin will be released against the tumor when Nab-P enters into the tumor cells. 27
As far as the authors know, no studies have directly confirmed whether there is a synergistic effect of Nab-P combined with PDT, so further studies are needed. Furthermore, some studies have pointed out that HpD will be carried by albumin when it enters the blood, 28,29 so whether HpD can be loaded onto the albumin structure of Nab-P to increase the concentration of HpD in tumor cells for efficacy enhancement needs to be verified with further experiments.
Conclusions
PDT has become an alternative therapy for advanced esophageal cancer, which cannot be resected or recur after chemotherapy and radiotherapy, due to its lower toxicity and prominent efficacy. Meanwhile, the strategy of using combination therapies based on PDT is a reliable option for palliative treatment. This article demonstrates the safety and efficacy of the combination therapy of PDT and Nab-P chemotherapy. Additionally, it provides a new option for patients who are not suitable for endoscopic localization and patients can be free from the pain of endoscopic operation.
However, the clinical application of PDT still has some main limitations. For instance, the laser penetrates the tissue to a shallow depth, which leads to a high recurrence rate. Furthermore, it is necessary to avoid light exposure for a long time to prevent the occurrence of photoallergy after the treatment. With the compatibility of combination therapy, diversification of the treatment, and improvement of the photosensitizer, PDT will have magnificent prospects in clinical application.
Footnotes
Authors' Contributions
W.Z., J.Z., and M.Z. collected the patient's clinical data, reviewed the literature, and drafted the manuscript; L.K. performed the pathological examination and collected digital images and drafted the manuscript; C.L., Z.X., and J.L. collected the patient's clinical data and contributed to manuscript drafting; and all authors issued a final approval for the version to be submitted.
Informed Consent Statement
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors thank the government-funded training of outstanding clinical medical talent and basic research projects in 2017.
The authors thank the patient and are grateful for the project funds provided by Key Research and Development in Hebei Province, China (20377777D).