
Abstract
Purpose:
Adrenocorticotropic hormone (ACTH)-dependent Cushing's disease accounts for 75% cases of the endogenous Cushing's syndrome. The size of lesion is usually very small, which results in false-negative magnetic resonance imaging (MRI) even after biochemical confirmation of the disease. Corticotrophin-releasing hormone (CRH) the key controller of hypothalamus–pituitary–-adrenal axis binds to CRH receptor R1 and R2. CRH R1 is overexpressed in pituitary adenomas. The present study aims to target these overexpressed receptors with 68Ga-DOTA-CRH for noninvasive imaging of ACTH-dependent pituitary adenomas.
Materials and Methods:
Custom-synthesized 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid (DOTA)-CRH peptide was purified by high performance liquid chromatography (HPLC) and characterized by mass spectra. Postradiolabeling optimization with 68Ga, quality control tests were carried out to ensure the suitability of 68Ga DOTA-CRH for intravenous administration. A pilot study consisting of 15 patients including 6 known cases of macroadenoma underwent 68Ga-DOTA-CRH regional brain positron emission tomography/computed tomography (PET/CT). The optimal imaging time and biodistribution studies were performed in five patients' whole-body and serial brain PET/CT imaging. Lesion activity was determined as SUVmax and correlated with CE-MRI and histopathology of excised tissue.
Results:
A retention time of 11.3 min and mass of 5145 Da was observed on HPLC and mass spectra. Radiolabeling yield of >98% was achieved under optimized conditions using 25–100 μg of conjugated peptide for 10–22 mCi of 68Ga. The quality control results were in agreement with acceptable criteria. 68Ga-DOTA-CRH was able to delineate ACTH secreting corticotropinoma in all 15 patients. Physiological uptake of radiotracer was observed in liver and spleen with diffused marrow activity. Excretion was noted by renal route. Imaging results were in correlation with CE-MRI and histopathology of excised tissue.
Conclusion:
68Ga-DOTA-CRH PET/CT is a promising molecular imaging modality for detection of ACTH-dependent microadenoma.
Introduction
Cushing's syndrome refers to a variety of clinical symptoms either owing to endogenous production of excessive adrenocorticotropic hormone (ACTH) or independent secretion of cortisol from adrenals. ACTH-dependent Cushing's syndrome accounts for 80%–85% cases of which 75% cases are the result of Cushing's disease (ACTH secreting pituitary adenoma), 15%–20% from ACTH secreting ectopic tumors, and <1% by corticotrophin-releasing hormone (CRH)-producing tumors. 1 –4 ACTH-independent Cushing's syndrome accounts for 15%–20% cases in adults of which 90% cases are caused by adrenal tumors. Although the incidence rate is only 0.2–5.0 per million people per year, the morbidity and mortality associated with this disease is very high because of the associated consequences of cardiovascular disease and infection. 5 –7
Diagnosis of Cushing's syndrome involves multiple biochemical tests like 24 h urinary free cortisol (UFC), late-night salivary cortisol, low-dose dexamethasone suppression test (DST), and CRH stimulation test. The sensitivity and specificity of these tests are variable. 8,9 The most commonly used magnetic resonance imaging (MRI) technique also has limitation in the identification of pituitary adenomas below 6 mm of size. Inferior petrosal sinus sampling (IPSS) is considered the gold standard procedure that distinguishes ACTH secreting pituitary adenoma from ectopic ACTH syndrome (EAS). 10 –13 However, the method is invasive in nature and requires dedicated facilities and a high degree of perfection in addition to the involved cost. In addition, its role is still controversial for determining the precise location of the tumor. There is ample scope for the development of new functional imaging probes/techniques that can determine the location of pituitary tumors noninvasively.
Positron emission tomography/computed tomography (PET/CT) is a powerful diagnostic modality providing anatomical and molecular whole-body details in a single study. Fluorine-18-labeled deoxyglucose (18F FDG) is the most widely used PET tracer for diagnosis, staging, restaging, reoccurrence, and response evaluation in cancer patients. 14 –17 Because of the high physiological uptake of 18F FDG in the brain, its diagnostic utility in Cushing's syndrome is limited only to the localization of site in the EAS. 18,19 Gallium-68 (68Ga)-labeled 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid (DOTA)-TATE/TOC are peptide-based other PET radiopharmaceuticals that have also been explored to detect EAS, targeting the overexpressed somatostatin receptors (SSTR). 20 –22
CRH, the fundamental controller of the hypothalamus–pituitary–adrenal (HPA) axis is a 41 amino acid peptide derivative that binds to two receptor subtypes namely CRH-R1 and CRH-R2. Overexpression of CRH-R1 is reported in pituitary adenomas compared with normal pituitary. 23,24 Synthetic CRH peptide, when radiolabeled with suitable radioisotope (68Ga/18F), can be used to image the overexpression of CRH receptors in Cushing's disease. The authors herein share the initial radiolabeling and PET/CT imaging experience of novel 68Ga-labeled synthetic CRH for differential diagnosis of ACTH-dependent Cushing's syndrome.
Materials and Methods
Commercially available Germanium-68 (68Ge)/Gallium-68 (68Ga) generator (ITG, Germany) was utilized to obtain 68Ga for radiolabeling. The other reagents and chemicals used during radiolabeling were of high performance liquid chromatography (HPLC) grade.
Synthesis of DOTA-CRH
DOTA-coupled synthetic CRH (DOTA-CRH) was custom synthesized. The conjugated peptide was lyophilized and characterized by HPLC and mass spectra. For HPLC a gradient of acetonitrile and water (30%–100%) with 0.1% trifluoroacetic acid was used as mobile phase. The HPLC sequence was run for 40 min. The absorbance was measured at 220 nm. The lyophilized peptide was reconstituted in water (1 mg/mL) and aliquots (25 μL) were stored at −20°C until further used for radiolabeling.
Radiolabeling of DOTA-CRH peptide with 68Ga
The radiolabeling was performed in a semi-automated fluidic module (ITG). 68Ga was freshly eluted in the form of gallium chloride (GaCl3) from the 68Ge/68Ga generator with 0.05 M hydrochloric acid (HCl). A varied amount of peptide (25–100 μg) was used for radiolabeling. The radiolabeling reaction was carried out at 95°C. The pH of the reaction mixture was maintained with 0.25 M sodium acetate (NaOAc) buffer solution. Purification of 68Ga-DOTA-CRH was performed by preconditioned light C-18 cartridge. The final product was eluted with 50% ethanol followed by dilution with saline (8 mL). The pH of 68Ga-DOTA-CRH was maintained in the physiological range with 0.25 M NaOAc buffer solution. To maintain the sterility of the preparation 68Ga-DOTA-CRH was passed through 0.22 μm GV filters (Millipore, Ireland).
Quality control of 68Ga-DOTA-CRH
After purification the final product was subjected to various physicochemical and biological quality control tests including radionuclide purity, radiochemical purity, chemical purity, sterility, and pyrogenicity according to procedures reported earlier. 25 In brief, the radionuclide purity was tested by a multichannel analyzer at the open window at 0 and 24 h postelution. Radiochemical purity was tested every 15 min for up to 2 h by instant thin layer chromatography (ITLC). Sodium citrate (0.5 M) buffer solution was used as the mobile phase and silica gel-coated ITLC strips were used as the stationary phase. The strips were read in the ITLC scanner (TLC-204; Comecer). Residual solvent (ethanol) was tested by gas chromatography (Varian). Pyrogenicity was tested using the PTS system (Charles River). Sterility was checked by incubating the samples in fluid thioglycollate medium and tryptic soy broth medium. In vitro stability of 68Ga-DOTA-CRH was tested in phosphate-buffered saline (PBS) for up to 2 h.
Inclusion and exclusion criteria for patients
The study was duly approved from the institutional ethics committee (NK/37771/Study/5440). Patients with clinical suspicion of Cushing's syndrome, who were 18 years or older, and ready to give written informed consent were included in the study. Pregnant and lactating women, claustrophobic, unstable, and noncooperative patients were excluded from the study. All patients underwent CE-MRI. Patients presenting with a lesion in pituitary on either modality underwent surgical resection. The findings of the fused PET scan were also used to lateralize the tumor for intraoperative navigation and also for histopathological comparison of the excised tissue.
PET/CT imaging
In this pilot study, 15 patients including 6 known case of macroadenoma were recruited. PET/CT scan was performed in all the patients 35–40 min after intravenous administration of 3–5 mCi of 68Ga-DOTA-CRH. To determine the maximum uptake of 68Ga-DOTA-CRH in the pituitary, initial five patients were subjected to serial brain PET image acquisition. The imaging was initiated immediately after the injection of radiotracer on bed followed by nine consecutive images (300 s/image) for up to 45 min. Whole-body noncontrast PET/CT imaging from the base of the skull to mid-thigh was also acquired in these five patients, to see the biodistribution of 68Ga-DOTA-CRH. For the whole-body acquisition, time of each PET bed position was 90 s. In the remaining 10 patients, only regional brain PET/CT imaging was performed with an acquisition time of 10 min. For all the patients, CT data were acquired first followed by PET acquisition. Regional brain CT acquisition was performed with tube voltage of 140 kVp, tube current 280 mA, 3.75 mm helical thickness, 0.8 s rotation time, and 0.531:1 pitch. The CT images were reconstructed in a matrix of 512 × 512 with a slice thickness of 1.25 mm. For whole-body imaging CT acquisition, tube voltage of 120 kVp, tube current of 10 mA, 3.75 mm helical thickness, 0.5 s rotation time, and pitch of 0.984:1 was used. Attenuation correction of PET images was CT based. The PET images for the brain were reconstructed in a matrix of 256 × 256 using ordered subset expectation maximization (32 subsets, 5 iterations) and a Z-axis Gaussian filter with full width half maximum of 2.5 mm. The whole-body PET images were reconstructed in a matrix of 192 × 192 using ordered subset expectation maximization (24 subsets, 2 iterations) and a Z-axis Gaussian filter with FWHM of 5.5 mm.
The reconstructed data were processed (Advantage workstation ADW 4.6, GE Healthcare) and images were obtained in trans-axial, sagittal, and coronal sections. The images were interpreted independently by two experienced nuclear medicine physicians on per-patient basis who were blinded to the patient's history. A region of interest was drawn carefully around the site of abnormal uptake of 68Ga-DOTA-CRH. The lesion activity was represented as maximum standardized uptake value (SUVmax).
Results
Synthesis of DOTA-CRH
The custom synthesized CRH peptide consists of 41 amino acids with mass 4740 Da. For radiolabeling with 68Ga, the peptide was coupled with DOTA bifunctional chelator. The sequence of peptide is DOTA-SEEPPISLDLTFHLLREVLEMARAEQLAQQAHSNRKLMEII-NH2. The retention time of DOTA-CRH peptide was observed to be 11.3–11.6 min. Based on area under the curve, the purity of chelated peptide was found to be >95%. The mass of DOTA-CRH was observed to be 5144 Da on mass spectra as given in Figure 1.
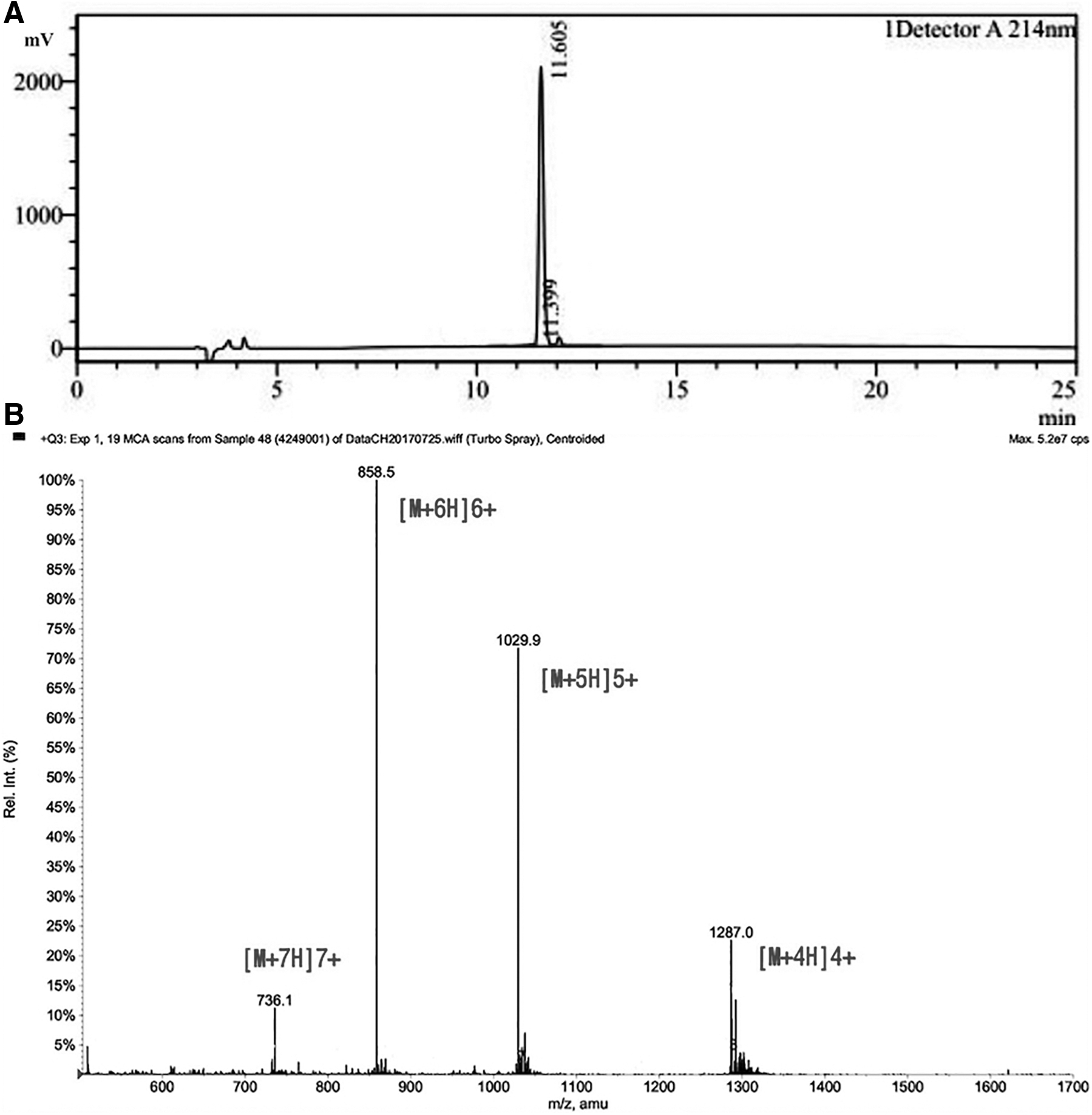
HPLC chromatogram
Radiolabeling of DOTA-CRH with 68Ga
68Ga eluted in the form of GaCl3 was directly used for radiolabeling without any concentration or purification. A maximum of 98% radiolabeling yield was achieved by incubating 25–100 μg of DOTA-CRH peptide with 10–22 mCi of 68Ga radioactivity at 95°C for 10 min at 3.5–4.0 reaction pH.
Quality control of 68Ga-DOTA-CRH
The radionuclide and radiochemical purity postpurification were found to be >99% in all preparations. At 2 h the radiochemical purity (RCP) was observed to be >98% indicating the stability of radiotracer till 2 h at room temperature as given in Table 1. The retardation factor (Rf) of 68Ga-DOTA-CRH was observed to be 0.0–0.1 on the ITLC-SG strip with sodium citrate buffer solution as the mobile phase (Fig. 2). The residual ethanol content (<4000 ppm) and endotoxins (<3.5 EU/mL) were well below the permissible limit 4000 ppm and 175 EU/V, respectively. The samples were found to be sterile on sterility tests. The in vitro stability in PBS at 1 and 2 h was observed to be >98% and 97%, respectively (Table 1). All the quality control tests indicated the suitability of radioactive preparation of 68Ga-DOTA-CRH for intravenous administration.
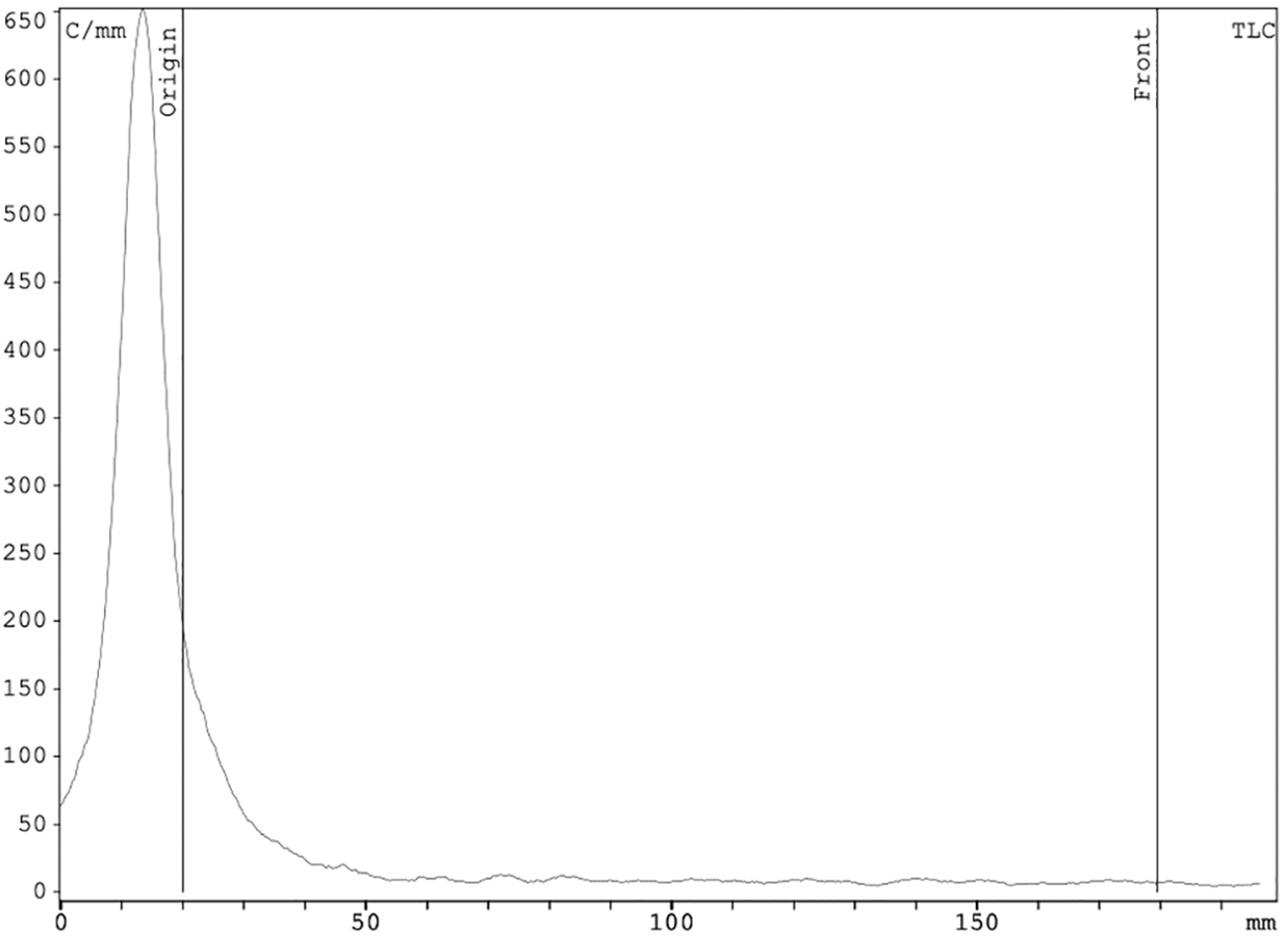
Radio-ITLC chromatogram of 68Ga-DOTA-CRH using sodium citrate as mobile phase. Only single peak was observed at the origin indicating absence of any free 68Ga (Rf 1.0). The Rf of 68Ga-DOTA-CRH was observed to be 0.0. ITLC, instant thin layer chromatography.
Stability Data of Ga-DOTA-CRH at Room Temperature and in Serum
DOTA-CRH, 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid-corticotrophin releasing hormone; RCP, radiochemical purity; RT, room temperature.
Patient imaging
A total of 15 patients (6 men and 9 women) with mean age of 41.46 ± 15.93 years (range 21–64 years) were recruited in this pilot study. The demographics of patients are given in Table 2. Serial PET images up to 45 min followed by whole-body PET/CT images were acquired in 5 of the 15 patients (Fig. 3). Based on the mean SUVmax obtained from serial images, the optimum imaging time was observed to be 35–40 min postadministration of 3–5 mCi of 68Ga-DOTA-CRH. The physiological distribution of 68Ga-DOTA-CRH was noted in the liver and spleen with diffused uptake in bone marrow and pituitary. Excretion of 68Ga CRH was observed through the renal route as given in Figure 4.

A 63-year-old man (patient 1) with complaint of headache and disturbance in vision. MRI showed localized mass in sella and underwent serial brain PET and whole-body 68Ga-DOTA-CRH PET/CT imaging. Tracer uptake was noted in lesion on serial brain PET images
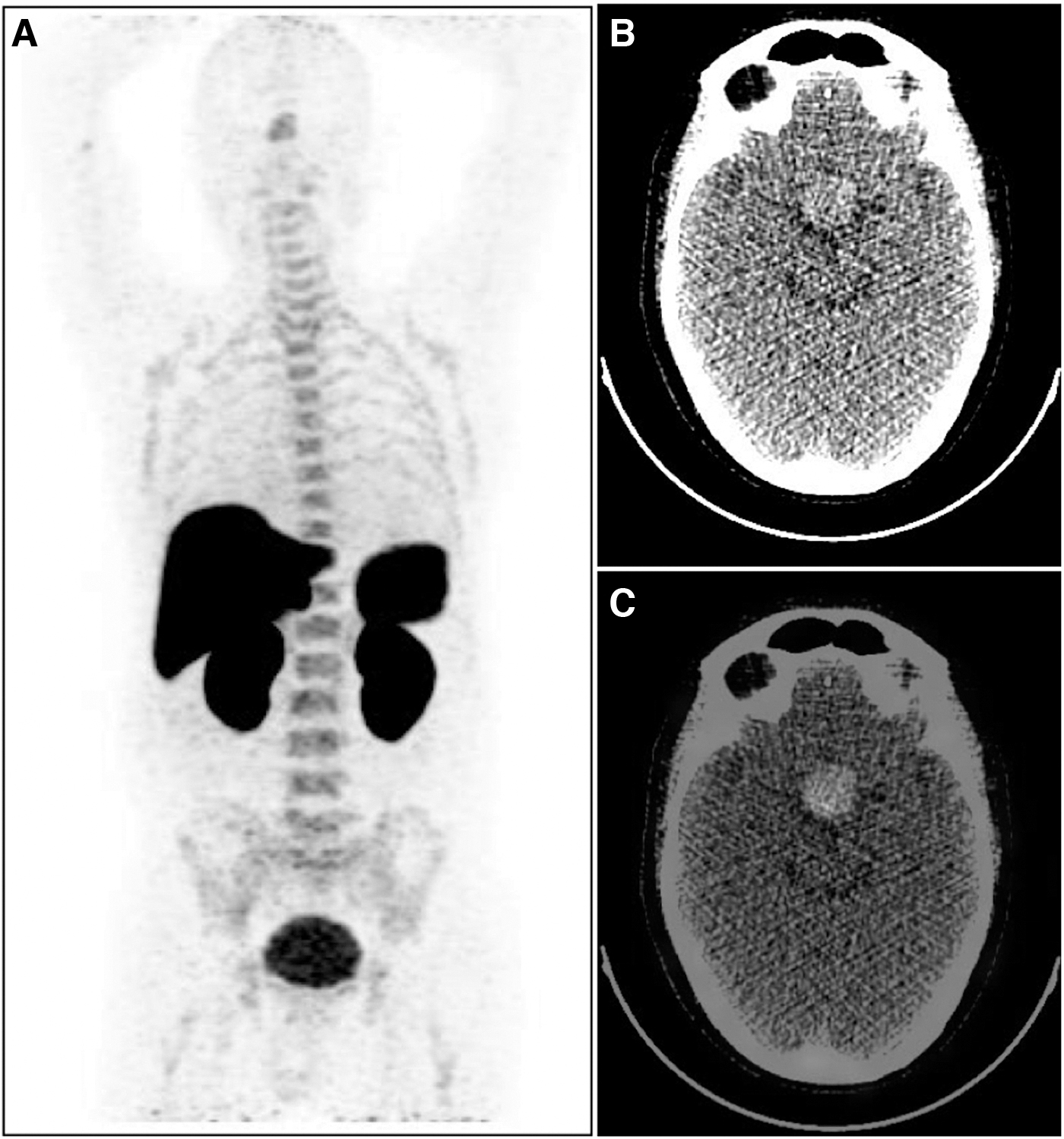
Whole-body image of 63-year-old man (patient 1) acquired 45 min post administration (90 s/frame) of 68Ga-DOTA-CRH. MIP image
Patient Details
B/L, bilateral; F, female; Lt, left; M, male; MRI, magnetic resonance imaging; NA, not applicable; Rt, right; SUVmax, maximum standardized uptake value; TSS, transsphenoidal surgery.
Both CE-MRI and 68Ga-DOTA-CRH PET/CT were able to delineate ACTH secreting corticotropinoma in all 15 patients (Table 2). Macroadenoma and microadenoma were observed in 6 and 9 patients, respectively. A representative image is given in Figure 5. The mean SUVmax of lesions was 2.95 ± 1.37 (range 1.2–6.2). The imaging results were also confirmed by the histopathology of excised tissue.
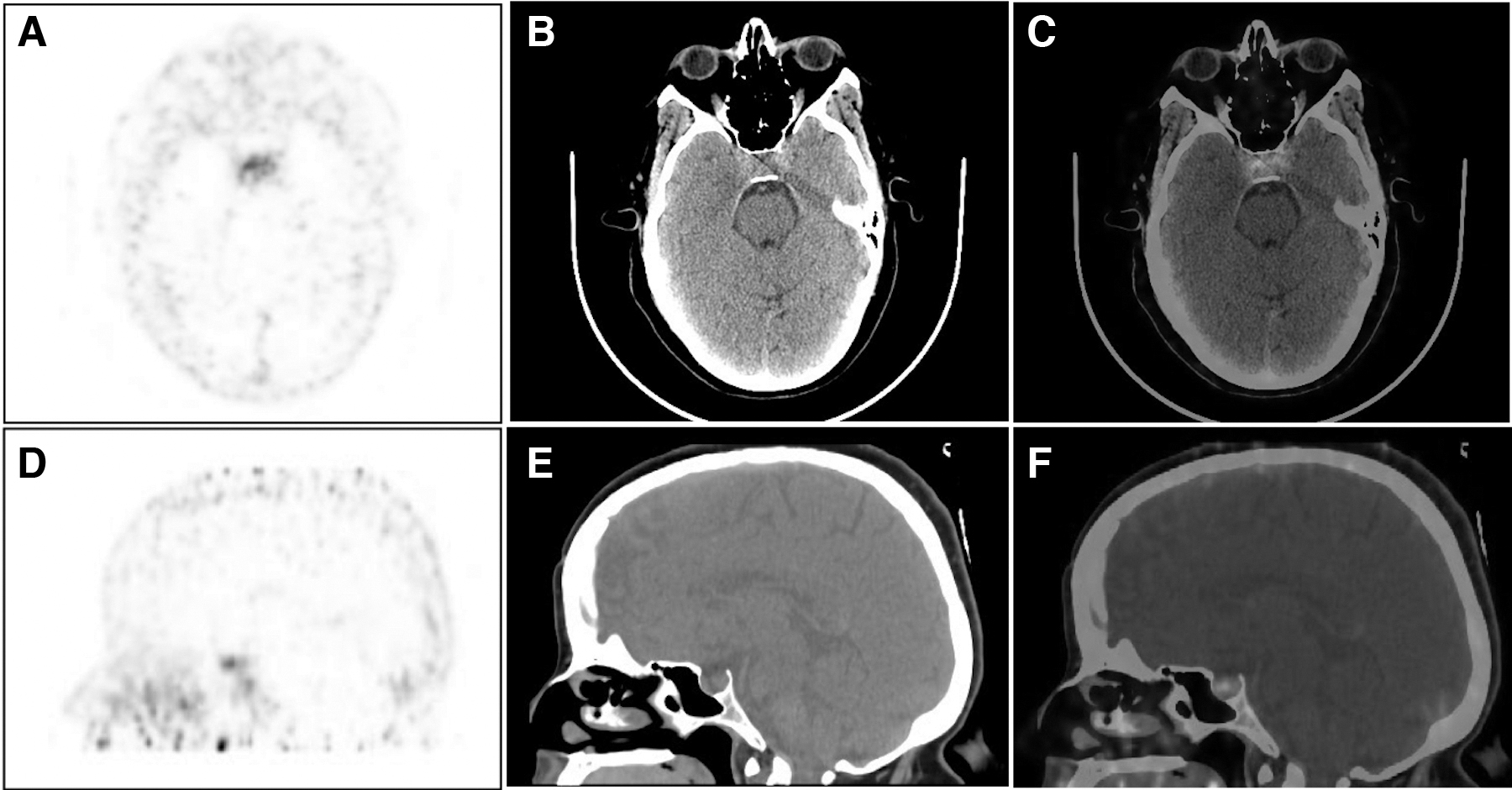
A 23-year-old woman with history of weight gain, muscle weakness, swelling of face, and differentially enhancing lesion along lateral aspect of sella on MRI underwent 68Ga-DOTA-CRH PET/CT imaging
Discussion
Accurate delineation of ACTH-secreting lesions in Cushing's disease is a clinically challenging task. Multiple biochemical tests like 24-h UFC, late-night salivary cortisol, DST, and CRH stimulation test are needed to be performed. 8,9 Because of the small size (<1 cm, mean diameter 6 mm) of the lesion at the time of biochemical diagnosis, the false-negative results on pituitary MRI are high. To enhance the detection efficiency of imaging, spoiled gradient recalled (SPGR) acquisition MR sequences are preferred leading to 15%–30% higher lesion detection as compared with other available MRI sequences. 10,26 –28 IPSS, being invasive in nature, remains the gold standard technique for accurate diagnosis of ACTH-dependent Cushing's disease. The IPSS is an expensive procedure and requires dedicated facility and expertise manpower. Functional imaging with suitable biomarkers may prove beneficial for accurate diagnosis of ACTH-dependent Cushing's disease. CRH is known to be the key regulator of the HPA axis. 23,24 The authors herein report the targeting of overexpressed CRH receptors using 68Ga-labeled synthetic CRH peptide and its preliminary PET/CT imaging experience in patients for differential diagnosis of ACTH-dependent Cushing's syndrome.
In this study, 25–100 μg of DOTA-CRH peptide was used for 2–5 patients, respectively. The amount is proportionate to the quantity used in other 68Ga-based radiopharmaceuticals. 29 –31 The radiolabeling yield (95%–98%) of DOTA chelated synthetic CRH peptide was comparable with other 68Ga-labeled radiopharmaceuticals. 29 –34 Depending upon the number of patients, the amount of peptide to be used for radiolabeling can be regulated. This approach will help in the judicious use of peptide along with restraining the saturation of CRH receptors with cold peptide. All the quality control tests were at par with the standards. The RCP of >99% was achieved for all batches and the residual ethanol and pyrogen content were within the permissible limits indicating competence of the radiopharmaceutical for human administration.
68Ga-DOTA-CRH was observed to be well tolerated by all the patients, similar to the other 68Ga-labeled PET tracers like PSMA-11 and DOTANOC/TATE, which are used routinely for prostate cancer and neuroendocrine tumor imaging, respectively. This is a pilot study imaging overexpressed CRH R1 receptors in Cushing's disease using 68Ga-labeled synthetic CRH peptide. Hence, serial PET brain images were acquired initially in five patients to determine the optimal imaging time. Whole-body PET/CT imaging was also performed to recognize the physiological distribution of 68Ga-DOTA-CRH. Six known cases of pituitary macroadenoma were deliberately included to observe uptake of 68Ga-DOTA-CRH. The radiotracer physiological distribution was in corroboration with the receptor (CRH-R1 and CRH-R2) expression in pituitary and peripheral organs like liver, pancreas, gastrointestinal tract, spleen, adrenal glands, heart, lymphocytes, and thymus as reported in literature. 35 –37
Receptor-based radiotracers like Tc-99m TRODAT (SPECT tracer), 18F FDOPA, 18F FES, 18F FDG, 68Ga PSMA-11, 68Ga DOTATATE, and 68Ga RGD, and so on, have been used for imaging various receptors expressed in different oncological and nononcological conditions. This receptor-based imaging helps in assessing the overall tumor burden along with identification of tumor receptor expression. 38,39 In the case of Cushing's disease, MRI is the modality of choice for imaging the pituitary gland. However, because of the small size and location of pituitary microadenomas in Cushing's disease, the false-negative imaging rate is very high (30%–50%). 40,41 In addition, currently available receptor-based PET imaging tracers 18F FDG and 68Ga DOTATATE are helpful only in the differential diagnosis of EAS. In this study, CRH imaging was able to delineate the ACTH pituitary corticotropinoma in all the 15 patients. The overexpression of CRH-R1 has been reported in cases of pituitary adenomas. 24,42,43 The same was also evident from localized increased radiotracer uptake in pituitary regions on the 68Ga-DOTA-CRH PET/CT scan of patients. The imaging outcomes were in correlation with MRI and histopathological findings of surgical samples. The study indicates that receptor-based imaging may play a significant role in the accurate diagnosis of ACTH-dependent Cushing's disease noninvasively. This is a pilot study to provide a proof of concept for the role of CRH receptor imaging in the differential diagnosis of Cushing's disease. In the future, the role of CRH receptors in ectopic Cushing's syndrome needs to be further explored. The results from this study will encourage multicentric imaging trials enrolling more patients to further confirm the role of CRH receptor-based imaging in Cushing's disease.
Conclusion
DOTA chelated synthetic CRH peptide was successfully synthesized and radiolabeled with 68Ga generating good radiolabeling yield. Receptor-based PET/CT imaging with 68Ga-DOTA-CRH has opened opportunities to delineate the source of ACTH access noninvasively. In this study, 68Ga-DOTA-CRH was able to detect ACTH secreting pituitary adenoma in all patients. In addition, further evaluation in higher number of patients and comparison with other present modalities is under progress.
Footnotes
Authors' Contributions
J.S.: Conceptualization and designing of study, radiolabeling optimization, and QC of 68Ga DOTA-CRH, and final article editing. R.V.: Optimization of radiolabeling and QC of 68Ga DOTA-CRH, data processing, article writing. R.W.: Conceptualization and designing of study, patient referral and management, interpretation of data, and article editing. A.C.: Preparation and QC of 68Ga DOTA-CRH. N.R.: Patient's PET/CT image acquisition and data processing. H.S.: PET/CT image analysis. R.K.: PET/CT image analysis. B.R.M.: PET/CT image analysis and article editing.
Disclosure Statement
J.S., R.W., and B.R.M. have patent for Corticotrophin Releasing Hormone Peptide for Positron Emitting Tomography Imaging in Cushing's Syndrome pending.
Funding Information
No funding was received for this work.