
Abstract
Background:
The aim of this study is to clarify the critical organs that limit treatment scheme and also evaluate the validity of currently used critical organ threshold values in neuroendocrine tumor (NET) patients, receiving peptide receptor radionuclide therapy (PRRT) with Lutetium 177 (177Lu)-DOTATATE.
Materials and Methods:
Thirty-six NET patients (ages 16–73 years) who received 177Lu-DOTATATE treatment were evaluated retrospectively in this study. Dosimetric calculations were made using medical internal radionuclide dose method. For calculation of organ doses, Internal Dose Assessment at Organ Level/Exponential Modelling 1.1 software program was used. Follow-up data were used to determine the organ failure.
Results:
A total of 141 cycles and mean of 3.91 (±1.33) cycles were applied to the patients. A mean of 691 mCi (±257 mCi) 177Lu-DOTATATE infusion in total and a dose between 70 and 200 mCi per treatment was applied to patients. Seven of 36 patients reached 23 Gy renal dose limit. In these patients, although kidney doses were between 23 and 29 Gy, there was no diminution in renal functions during follow-up. Two of 36 patients reached total bone marrow dose of 2 Gy limit. Bone marrow suppression did not develop in these patients.
Conclusion:
The critical organs that seem to affect the treatment scheme in PRRT with 177Lu-DOTATATE are kidney and bone marrow. Although there are established threshold levels, derived from radiotherapy experience, more studies are needed to clarify these dose limits in systemic radionuclide therapies such as PRRT.
Introduction
Neuroendocrine tumors (NETs) account for only 1%–2% of all neoplasms. The incidence of NETs is higher in males and increases with age. NETs are found most commonly in the stomach, intestine, pancreas, and lungs in the body, but they can also originate in other tissues such as ovary and testes. Although NETs have usually good prognosis, they may be aggressive at times. 1
Clinical studies of patients who received peptide receptor radionuclide therapy (PRRT) for metastatic NETs demonstrate the long-term effectiveness of this treatment, which also allow patients to maintain a high quality of life. 2 The aim of radionuclide treatments is to provide the maximum radiation dose to the tumor tissue while ensuring that other organs are exposed to the minimum radiation dose. The best results in tumor destruction are obtained when the absorbed dose is close to, but not exceeding, the maximum acceptable dose for radiosensitive organs. In radiotherapy, the absorbed dose to organs at risk varies with their proximity to the radiation field. In PRRT, the individual kinetics of the used peptide determine the tissue activity distribution. In radiotherapy, the cumulative dose is given in 5 weeks in maximum. Treatments in PRRT are given at 6–8 week intervals, but since the total treatment is given in a period, as long as 1 year, the reaction of the cells to radiation may differ. Although the absorbed doses to organs and tumors are governed by a complex combination of factors in radionuclide therapies, accepted upper limit doses of critical organs in radionuclide therapies are adapted from the data of radiotherapy.
Lutetium 177 (177Lu), which is a medium-energy β−-emitter (maximum energy of 498 keV) with 6.73 d of physical half-time, also emits two additional γ-photons (208 and 113 keV in 11% and 6.4% abundance, respectively). This characteristic enables both the imaging and therapy with the same compound labeled with this radionuclide and allows dosimetry during treatment as well. 3,4 177Lu-DOTATATE is the mostly preferred radiopharmaceutical in PRRT, which binds to the somatostatin receptor type 2 in both primary and metastatic lesions of NET. Owing to the kinetic distribution of radiopharmaceutical in PRRT, it accumulates in some organs besides the targeted tumor tissue. The kidneys and the bone marrow are accepted to be the main dose-limiting organs during PRRT. 5,6
According to the data, derived from radiotherapy experience, 23 Gy is accepted to be the critical dose for kidneys and 2 Gy for bone marrow. 7 Critical organ doses are important in determining both the number of treatments, interval time between them, and also amount of radiopharmaceutical to be given to the patient in each treatment cycle. In general practice, four cycles of PRRT are given to the patients with the interval time of 6–8 weeks. The physiological state that varies from patient to patient leads to individual characteristics in each patient, which can only be included in the treatment decisions only if patient-based dosimetric approach is used. With the addition of personal dosimetric approach, both the number of treatment cycles and also the radiopharmaceutical dosage can be modified to increase the therapeutic effects of PRRT without causing additional deterministic effects or toxicities in the patient. In the literature, there are numerous articles that showed that renal doses up to 29 Gy is well tolerated in PRRT patients. 8
In this study, we aimed to determine the critical organs that limit the treatment scheme and also evaluate the validity of currently used critical organ threshold values in NET patients, receiving PRRT with 177Lu-DOTATATE.
Materials and Methods
Patient population
This study included 36 (18 female and 18 male) NET patients (8 pancreatic NET, 6 thyroid medullary carcinoma, 2 pulmonary NET, 1 duodenal NET, 1 gastric NET, and 18 unclassified NET) who were treated in our clinic with 177Lu-DOTATATE between 2015 and 2018. Patient data were evaluated retrospectively. The treatment of all patients was completed or terminated by evaluating the general condition of the disease and the patient, along with dosimetric evaluation. The collection of human samples in this study were approved by the Ethics Committee of Istanbul University, Istanbul Medical Faculty (permission no. 2014-1971).
Treatment procedure
After review of clinical evaluation, biochemistry and 68Ga-DOTATATE positron emission tomography-computerized tomography (PET-CT) of patients diagnosed with NET, treatment compliance was decided. Patients who had high 68Ga-DOTATATE accumulation in tumor sites were accepted as eligible for radionuclide therapy. Prophylactic amino acid infusion was initiated 3 h before 177Lu-DOTATATE infusion to protect kidneys by reducing activity involvement in kidneys. After 3 h of amino acid infusion, patient received 177Lu-DOTATATE infusion intravenously for 30 min. The amino acid infusion continued for another 30 min after end of 177Lu-DOTATATE infusion. 9 The first treatment dose was determined by empirical method based on clinical experience and in following cycles, the dose was modified according to dosimetric results.
Dosimetric method
In this study, dosimetric calculations were made using the medical internal radionuclide dose (MIRD) method. Whole body and single photon emission computerized tomography-computerized tomography (SPECT-CT) images of patients were performed with a gamma camera, equipped with a CT scanner (GE Discovery NM670; General Electric Healthcare, Waukesha, WI) after each treatment to calculate the radiation dose absorbed by the critical organs. With the help of the gamma camera images obtained, the amount of activity accumulated in the organs and the whole body was calculated. For bone marrow dosimetry, blood samples were collected from the patients after each treatment. Blood samples were measured in well-type gamma counter (Biodex; Atomlab 930). With help of the values obtained from the well-type gamma counter, activity amounts in the blood were calculated. Using the MIRD calculation formula, radiation doses absorbed by critical organs were calculated using organ and blood activity. 10
Total blood activity determination
For bone marrow dosimetry, it is recommended to take blood samples 0.5, 1, 2.5, 4, 8, and 24 h after start of 177Lu-DOTATATE application in the literature. 11 After the completion of 177Lu-DOTATATE infusion, 1 cc blood sample was drawn at 5, 10, 20, 40, 60, 60, 90, 120, and 180 min and also at 20, 24, 48, and 96 h to perform bone marrow dosimeter calculations for this study. Blood samples of the patients were counted in the well-type counter for 1 min and background counts were extracted from these 1 min counts and net counts were obtained. To provide the standardization in the counts, measurements were made by placing in one type of tube. Total blood activities (Ablood) were calculated using blood sample measurements. Total blood activity was calculated by multiplying the counts per 1 cc blood and total blood volume for each patient. This factor determination is described in the Count-Activity Conversion Factor for Blood and Urine section.
Total urine activity determination
To determine the effect of the bladder activity to the dosimetric calculation, we ensured that the patients collected their urine four times in 6 h periods (in total 24 h) after the end of the infusion of 177Lu-DOTATATE. After each period, we measured the volume of the urine and a sample of 1 cc was taken from the urine. These samples were counted in the well-type counter for 1 min. After counting the background counts, they were extracted from sample counts and the net counts were obtained. To provide the standardization in the counts, measurements were made by placing in one type of tube. Total urine activity was calculated by multiplying the counts per 1 cc urine and total urine volume. This factor determination is described in the Count-Activity Conversion Factor for Blood and Urine section.
Activity determination of organs on SPECT-CT and whole body images
To determine the distribution of radiopharmaceutical in the body and to calculate activities collected in the organs, whole body and SPECT-CT imaging was performed with the gamma camera at 4, 24, 48, and 96 h as mentioned in Sandström et al. 11 All imaging were performed with medium energy general purpose collimator and 20% energy window was centered on 208 keV photopeak. Whole body images were performed at a rate of 15 cm/min and the patient bladder was empty. SPECT images were performed with 128 × 128 matrix at 6° angles and 20 s at 360° in each angle. CT images were performed in the CT component of SPECT-CT device simultaneously.
CT-based attenuation correction was performed on SPECT images, and volume of interest (VOI) were detected by drawing the relevant areas of the organs.
Counts in the VOI plotted for the relevant organ were calculated. Total count was divided by the counting-activity conversion factor, which is described in the Count-Activity Conversion Factor for SPECT-CT and Whole Body Image section, and then the activity in the relevant organ was calculated. These procedures were repeated for all imaging after injection of 177Lu-DOTATATE of the patients.
Count-activity conversion factor determinations
The activity of radionuclide needs to be known to perform dosimetry calculations. Gamma rays are released in direct proportion to the activity of the radionuclide retained in the organ. When gamma cameras and gamma counters detect gamma rays, they provide numerical and visual results. From the obtained numerical value, the conversion factor must be determined to calculate the amount of measured radionuclide activity. We determined conversion factors that were used in the calculations with following methods.
Count-activity conversion factor for blood and urine
A common conversion factor was used for blood and urine. To set the standard for count-activity conversions, we measured 177Lu in the dose calibrator (Capintec CRC-15 BETA) and set it to ∼1 mCi. We then put this activity to a plastic cup filled with 2 L of water. After performing the remeasurement of empty injector, we calculated net activity by subtracting the empty injector measurement from filled injector measurement. The net activity was added into the water. After ensuring homogeneous distribution of the activity in water, 1 and 2 cc samples were taken and it was counted for 1 min in well-type gamma counter. Then background counts were determined and net counts were calculated. To minimize statistical errors, measurements were performed by placing them in uniform tubes and measurements were repeated for 5 times. Results were saved as counts per minute (cpm). To minimize the margin of error, the same process was repeated by adding 3 mCi 177Lu into 4 L of water. We calculated the counts per unit activity with the help of counts obtained from activities we measured. The average of these four measured values was calculated and used as a reference in the calculations. The count-activity conversion factor for blood and urine was calculated as (mCi/cpm). The obtained conversion factor was used to calculate activities in Total Blood Activity Determination and Total Urine Activity Determination sections.
Count-activity conversion factor for SPECT-CT and whole body image
Count-activity conversion factor was created for counts from SPECT-CT and whole body images of standard activity sources. An activity to create a standard activity sources was poured into water placed in a plastic bottle. Empty syringe was remeasured in dose calibrator. Net activity added into water was calculated by subtracting empty injector measurement from full injector measurement. Plastic bottle filled with water was scanned with the gamma camera. Scans were performed in the SPECT-CT and whole body protocols. Counts in all slices were calculated, the calculated counts were divided by net activity to generate counts per unit activity (count-activity conversion factor as counts/mCi).
Because size of organs and activity accumulated in the organs differ, these processes were repeated in different configurations to simulate activity of the patients' organs and repeated with 3.5, 8.5, 8.22, 20.1, and 30.3 mCi activities for different water volumes. Counts per unit activity (count-activity conversion factor) were calculated for SPECT-CT imaging of all different activities. The mean value of the results was calculated as count-activity conversion factor. The obtained conversion factor was used to calculate the activities in Activity Determination of Organs on SPECT-CT and Whole Body Images section.
Calculation of organ doses
Internal Dose Assessment at Organ Level/Exponential Modelling 1.1 software was used to calculate organ radiation doses.
Patient follow-up
After each treatment cycle, the complete blood count (CBC), renal, and liver function tests in all patients were measured in every 2 weeks until next treatment cycle. At the end of the last treatment cycle, the same procedure was repeated for 6 weeks. At the end of 3 months, the same procedure was repeated, along with 68Ga-DOTATATE PET-CT and in necessary cases, magnetic resonance imaging of the abdomen for evaluation of response to therapy. If no additional therapy was necessary according to clinical evaluation, the patients were checked in every 3 months with CBC, renal, and liver function tests. The decision of additional therapy cycles was given according to clinical evaluation along with dosimetric findings.
Results
The ages of 36 patients were between 16 and 73 years, with a mean of 54.66 (±12.89). A total of 141 cycles and a mean of 3.91 (±1.33) cycles were applied to the patients. One patient received 1 cycle, 6 patients 2 cycles, 2 patients 3 cycles, 19 patients 4 cycles, 3 patients 5 cycles, 4 patients 6 cycles, and 1 patient received 7 cycles. A mean of 691 mCi (±257 mCi) 177Lu-DOTATATE infusion in total and a dose between 70 and 200 mCi per treatment was applied to the patients. The demographic information of the patients, the number of treatment cycles, the total amount of radiopharmaceutical they received, and the results of the dosimetric calculations are given in Table 1. The median follow-up time was 20 months (2–61 months).
The Number of Treatment Cycles, the Total Amount of Radiopharmaceuticals, and the Results of the Dosimetric Calculations of All Patients
In 141 cycles of PRRT with 177Lu-DOTATATE in 36 patients, kidney doses were calculated as mean dose of 2.41 (±0.67) Gy/100 mCi (1.19 Gy/100 mCi [min] and 4.35 Gy/100 mCi [max]); bone marrow doses were calculated as mean dose of 0.120 (±0.067) Gy/100 mCi (0.035 Gy/100 mCi [min] and 0.336 Gy/100 mCi [max]); liver doses were calculated as mean dose of 1.27 (±1.31) Gy/100 mCi (0.503 Gy/100 mCi [min] and 6.75 Gy/100 mCi [max]); spleen doses were calculated as mean dose of 3.97 (±3.17) Gy/100 mCi (0.09 Gy/100 mCi [min] and 18.22 Gy/100 mCi [max]), and whole body doses were calculated as mean dose of 0.15 (±0.05) Gy/100 mCi (0.074 Gy/100 mCi [min] and 0.277 Gy/100 mCi [max]). When the organ doses were evaluated, kidney and bone marrow doses seemed to be critical in PRRT with 177Lu-DOTATATE.
Among 36 patients examined, the only patient who received just one treatment cycle was a child of 16 years whose total kidney dose was calculated as 3.05 Gy. The PRRT had to be terminated due to cholestasis.
The kidney doses of 6 patients who received two treatment cycles did not exceed the upper limit of 23 Gy. Three patients died during follow-up period and in the other 3 patients the treatments were terminated due to poor condition.
The kidney doses of 2 patients who received three treatment cycles did not exceed the upper limit of 23 Gy. Treatments were terminated due to poor condition.
Fifteen of 19 patients who received four treatment cycles had kidney doses <23 Gy. In 2 of these patients, grade 1 nephrotoxicity occurred during follow-up period with no need for an intervention. Kidney doses of remaining 4 patients were calculated between 23 and 29 Gy. In 2 of these patients, grade 1 nephrotoxicity occurred during follow-up period with no need for an intervention. In 1 of these patients, additional radionuclide treatment was planned. Although there was no diminution in renal function, with additional treatment dose, the kidney dose would exceed 29 Gy. Therefore, additional treatment was not given to the patient.
In 3 patients who received five cycles of treatment, in none of the patients any nephrotoxicity occurred, although in 2 of these patients, the kidney doses exceeded 23 Gy. In 1 of those patients, although an additional treatment was planned due to good response, the PRRT scheme had to be terminated in order not to exceed the critical kidney dose of 29 Gy.
In 4 patients who received six treatment cycles, the kidney doses of 3 patients were just below the threshold level and in the remaining patient it was >23 Gy. In this patient, although an additional treatment was planned due to good response, the PRRT scheme had to be terminated in order not to exceed the critical kidney dose of 29 Gy. In none of these patients, any nephrotoxicity occurred during follow-up period.
In 1 patient who received seven treatment cycles, kidney dose did not reach the upper limit of 23 Gy. No nephrotoxicity occurred during follow-up period.
Kidney doses per 100 mCi 177Lu-DOTATATE of all patients are given in Figure 1.

The kidney doses of all patients per 100 mCi 177Lu-DOTATATE. 177Lu-DOTATATE, Lutetium-177-DOTATATE.
When this study was evaluated in terms of total bone marrow doses; 2 patients reached the critical dose of 2 Gy limit. One of these patients received four cycles and the other patient received six cycles of treatment. Serious change in bone marrow reserve did not develop in these patients, during follow-up period with no need for an intervention. Critical bone marrow dose was not reached in other patients. Bone marrow doses per 100 mCi 177Lu-DOTATATE of all patients are given in Figure 2.
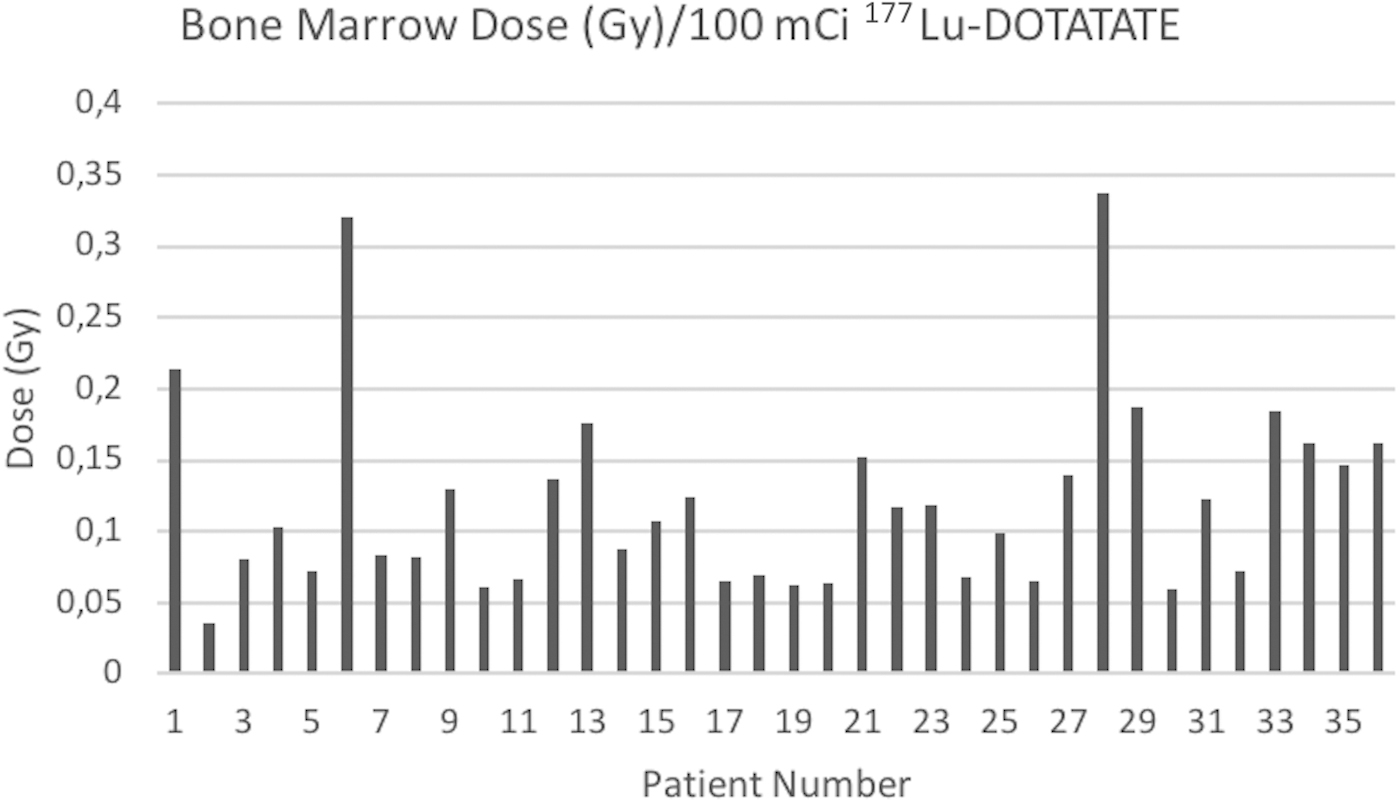
The bone marrow doses of all patients per 100 mCi 177Lu-DOTATATE.
Discussion
The PRRT is a well-tolerated radionuclide treatment in NET patients with favorable therapy response rates. Although there was a trend in limiting PRRT to four cycles before dosimeter methods have been developed, with the use of dosimeter methods, doses specific to each patient could be determined and treatment number could be increased. 5 In our patient group, 8 patients out of 36 patients (22%) had more than four cycles of 177Lu-DOTATATE treatment with no toxicities or side-effects. When deciding the number of treatments, the general condition of the patient and critical organ doses should be considered. Our study demonstrated in similar manner with the literature that the limiting critical organs in the treatment of 177Lu-DOTATATE were kidney and bone marrow.
In radiotherapy, absorbed dose limit of 23 Gy is used for the kidneys. 7 There are many studies showing that the dose of 23 Gy to the kidney is not a certain criterion for radionuclide therapies. Most studies adopted kidney absorbed dose thresholds between 23 and 27 Gy. 11 –14 Bergsma et al. suggested to increase the kidney maximum absorbed dose up to 28 Gy. 13 This was supported by the fact that half of the patients in their patient group did not reach 23 Gy after four cycles of 7.4 GBq 177Lu-DOTATATE. 15 In our patient group, 15 of 19 patients (79%) who had four cycles of 177Lu-DOTATATE treatment did not reach 23 Gy. Moreover, in 8 patients who had more than four cycles of therapy, 5 patients (62.5%) did not exceed 23 Gy. Because of the lower dose rates in PRRT, higher absorbed doses can probably be accepted, and Konijnenberg et al., 8 in view of the results of 3D imaging, argued for a limit of 29 Gy to the kidneys. In our whole group, only 7 patients out of 36 patients (19%) had kidney doses between 23 and 29 Gy. In only 2 patients, grade 1 nephrotoxicity occurred with no need of an intervention. In the median follow-up of 30 months (19–61 months) of these 7 patients, in none of the patients renal dysfunction occurred. In our study, a cautious approach was adopted by accepting 29 Gy as the limit for the absorbed dose and 3 (8%) patients were not given additional planned therapies not to exceed this threshold level. We think that more studies are needed to be able to determine the exact renal dose limit in PRRTs.
With knowledge from experience gained from radiotherapy applications, it is important not to expose the bone marrow to doses >2 Gy to prevent bone marrow hypoplasia. 16 In our study, only 2 patients (5.5%) reached 2 Gy, the upper limit for bone marrow, among 36 patients. Bone marrow suppression was not observed in these patients in the follow-up period of 36 months. The mean bone marrow dose was 0.120 (±0.067) Gy/100 mCi in our study. Looking at similar studies in the literature, bone marrow doses per 100 mCi was 0.12 (range, 0.09–0.16) Gy in the study by Sandström et al. 11 and 0.08 (±0.111) Gy in the study by Forrer et al. 17 Both in our study and also in the other studies in the literature, the radiation dose to bone marrow is quite low in PRRT. There are blood-based and SPECT-based bone marrow dosimeter methods. It is necessary to establish a standard for all different methods and determine the bone marrow upper limit dose for PRRTs. 17
The major limitation of our study was the small patient group, which did not allow us to make further analysis among different subgroups.
Conclusion
Dosimetric measurements should be performed to determine the tolerable radiation doses and to provide maximum safe treatment cycles to PRRT patients since critical organ doses vary among the patients. When evaluated in general, the critical organs for PRRT are kidney and bone marrow. The established threshold levels, derived from radiotherapy experience, especially for the kidneys, do not seem appropriate for systemic radionuclide therapies such as PRRT. More studies with larger patient numbers may clarify the exact dose limits for critical organs.
Ethical Approval
Ethics committee approval was obtained from the Ethics Committee of Istanbul University, Istanbul Medical Faculty (permission no. 2014-1971).
Footnotes
Disclosure Statement
There are no existing financial conflicts.
Funding Information
This study was funded by Research Fund of Istanbul University (project no. 49588).