
Abstract
Objectives:
Differentiation of infection from sterile inflammation is still a major concern for clinicians. The 18F-WBC positron emission tomography/computed tomography scan has been considered a promising tool for accurate diagnosis of infection owing to its high specificity, but it renders the availability of a medical cyclotron a necessity. The aim of the present study was to determine the feasibility of labeling leukocytes and establish the protocol in a center without the availability of an on-site medical cyclotron. The secondary aim was to monitor radiation doses to occupational workers involved in labeling of leukocytes with 18F-FDG.
Materials and Methods:
Leukocyte separation was performed and leukocytes were radiolabeled with 18F-FDG in a sterile environment according to the procedure described by Bhattacharya et al. In vitro leukocyte viability was assessed using the trypan dye exclusion technique. Labeling efficiency and yield were also estimated for all radiolabeling procedures. Whole-body and extremity doses received by the personnel involved in the radiolabeling procedure were also estimated using pocket dosimeters.
Results:
Leukocyte labeling was carried out in 35 runs, during which there were two failed labeling attempts due to clotting of the blood sample. The total time involved in the whole procedure was around 2.5 h. The average labeling efficiency was 78.01% ± 6.99% (range 63.46%–86.54%), cell viability was 98%, and the cell suspension was stable up to 4 h. The mean dose was measured as 17 μSv at the chest level and 32 μSv at the extremity level, per procedure.
Conclusions:
Labeling of leukocytes with 18F-FDG is possible at a tertiary nuclear medicine setup without the availability of an on-site medical cyclotron, with reasonable labeling efficiency of 78.01% ± 6.99%. In addition, in-house labeling of leukocytes with 18F-FDG is safe and the radiation doses incurred by the personnel during the labeling procedure are well within the occupational dose limits established by the national regulatory authority.
Introduction
The differentiation of infection from sterile inflammation is still a major concern for clinicians. Although several radiopharmaceuticals have been used for imaging of infection and inflammation, in vitro labeled leukocyte imaging using white blood cells (WBCs) labeled either with 111In-oxine or 99mTc-HMPAO has been established as the gold standard. 1 However, these studies were limited to γ-camera scintigraphy, and image quality and resolution were unsatisfactory. 2 Positron emission tomography/computed tomography (PET/CT) with 18F-FDG, although being nonspecific, has the advantage of higher spatial resolution and less time consumption than its gamma camera counterparts.
The feasibility of labeling leukocytes in vitro with 18F-FDG was first demonstrated by Osman and Danpure. 3 The basic principle behind it involves accumulation of FDG mainly in metabolically active inflammatory cells, which undergo an oxidative burst during inflammatory and infectious processes. 4 The avidity of inflammatory cells for FDG has led to efforts at labeling leukocytes with FDG in vitro, in an attempt to have the synergistic advantages of specificity of labeled leukocyte study with the anatomical resolution of PET/CT.
However, radiolabeling of leukocytes with F-18 is an exhaustive and cumbersome procedure and is associated with certain disadvantages such as the requirement of high specific activity of F-18, which renders the availability of an on-site medical cyclotron a necessity. The authors in this study have replicated the procedure used by Bhattacharya et al. 5 for labeling of leukocytes and studied its feasibility and established the protocol for centers without the availability of an on-site cyclotron. The secondary aim of this study was to monitor radiation doses received by the occupational worker involved in labeling of leukocytes with 18F-FDG.
Materials and Methods
Leukocyte separation and radiolabeling with F-18
Leukocyte separation was performed in a manner described by Bhattacharya et al. 5 The patient was kept nil per oral for 4 h, and subsequently, 40 mL of venous blood was collected in a heparinized syringe that was then kept upright in a stand at 37°C for 60–70 min to separate the plasma. Leukocyte/platelet-rich plasma supernatant was collected slowly into two, 14-mL, conical plastic tubes using a syringe attached with a 21 gauge butterfly needle and thereafter centrifuged at 1500 rpm for 15 min.
The platelet-poor plasma supernatant was removed and used for the final suspension of leukocytes, leaving the WBC pellet at the bottom of the tube. The white cell pellet at the bottom of the first tube was reconstituted with 2.5 mL of heparinized normal saline. Concentrated 18F-FDG (20–30 mCi) was added to the suspension. This radiolabeled suspension was kept at 37°C for 25–30 min, with gentle shaking every 5 min. During this time, the supernatant plasma was centrifuged at 2000 rpm for 25 min to obtain cell-free plasma.
After incubation, 12 mL of heparinized normal saline was added to the radiolabeled suspension, the tube was centrifuged at 1500 rpm for 5 min, and the supernatant was removed. The whole labeled cell suspension and supernatant were measured separately in a dose calibrator.
Labeling efficiencies (LEs) were calculated using the formula, LE = C/(C + W) × 100, where C is the cell-associated activity and W is the activity associated with the supernatant. The radiolabeled white cell sediment was reconstituted with 4 mL of the patient's own cell-free plasma and reinjected intravenously. The protocol has been shown in the flowchart (Fig. 1).

Flowchart showing the optimal procedure of labeling leukocytes with 18F-FDG.
Viability study
In vitro leukocyte viability was assessed using the trypan dye exclusion technique. One hundred microliters of the labeled cell suspension was transferred into a tube containing 250 μL of 0.4% trypan blue solution. The tube was allowed to stand for 5–15 min before determining the number of viable cells using a hemocytometer. Microscopic examination was performed on aliquots of labeled leukocytes at 1, 2, and 3 h after labeling.
Viable cells do not take up the dye, whereas nonviable cells do. Cell viability (V) was calculated using the formula, V = N/(N + B) × 100, where N represents the number of viable cells and B the number of trypan dye-containing cells. A minimum of 100 cells were counted for all viability measurements.
Stability test
Cell-free plasma (200–300 μL) was added to 0.5 mL of labeled leukocytes, kept at room temperature for 4 h, and centrifuged at 2000 rpm for 10 min. Radioactivity in the supernatant and labeled leukocytes was measured in a dose calibrator, and radioactivity that was eluted from the labeled cells was calculated as follows:
Personnel monitoring
Calibrated electronic pocket dosimeters (MYDOSE mini PDM, G-9679) based on solid-state (silicon semiconductor) detectors were used to measure the whole-body and extremity doses and both dose rate and accumulated dose were displayed. The measurement of these detectors ranged from 1 μSv to 1 Sv (0.1 mrem to 100 rem) for the dose and from 1 μSv/h to 100 mSv/h (0.1 mrem/h to 10 rem/h) for the dose rate. The accuracy was within ±10%, from 10 μSv to 1 Sv (from 1 mrem to 100 rem), and linearity was within ±20%, from 10 μSv/h to 100 mSv/h (from 1 mrem/h to 10 rem/h).
Dosimeters were worn at the level of the chest and on the dorsal surface of hands at the same position for each measurement. Each worker was provided with two electronic pocket dosimeters, one for the chest level and one for the extremity level, which were worn throughout the given task. The whole-body and extremity doses received by the worker were read directly from the dosimeters and recorded at the end of the task. The time spent for each procedure was recorded.
Patient studies
Patients with elevated CRP and ESR levels, presence of either suspected or documented bacterial infection, documented infection with unknown extension of the infection, and total leukocyte count >4000/mm3 were included in the study. Exclusion criteria were age <18 years, favorable clinical response to an antibiotic treatment applied for >7 d, and pregnant/lactating patients. The institutional ethics committee approved the study protocol, and written informed consent was obtained from all patients before participation.
For the 18F-FDG leukocyte scan, patients were instructed to fast for at least for 6 h before 18F-FDG-labeled leukocyte administration. First, CT images were acquired for attenuation correction. Second, PET images were acquired from the skull base to the mid-thigh or ankle (if indicated) at 2 min per bed position on a TruFlight Select time-of-flight PET scanner (Philips) after 60 min. PET images were reconstructed iteratively using the ordered set expectation–maximization algorithm with attenuation correction.
Results
Leukocyte separation and radiolabeling with 18F-FDG
Leukocyte labeling was carried out in 35 batches using the optimized procedure shown in Figure 1. There were two failed labeling attempts due to clotting of the blood sample. One sample was processed at a time to prevent any cross-contamination of samples, which is always a concern in in vitro labeling techniques. The total time to perform the whole procedure was around 2.5 h. For the in-house labeling procedure, the average amount of 18F-FDG used was 967.55 ± 94.72 MBq (26.15 ± 2.56 mCi.).
Labeling was done by a skilled radiation worker, proficient with the procedure, under a sterile environment. The labeling efficiency demonstrated by the current study was 78.01% ± 6.99% (range 63.46%–86.54%), as shown in Table 1 (details in Supplementary Table S1). Mean activity injected into the patients was 348.2 ± 51.4 MBq (9.4 ± 1.4 mCi). During labeling, leukocytes were exhaustively collected from plasma at the end of the sedimentation period and were handled very gently. Occasional swirling of the leukocyte suspension during incubation was carried out to improve labeling efficiency.
Amount of Starting Activity of 18F-FDG Used, Injected Activity of 18F-FDG Leukocytes, Labeling Efficiency, and Yield of the Procedure
Radiation exposure
All the 33 radiolabeling procedures were done by two (Radiation worker 1, n = 16, and Radiation worker 2, n = 17) qualified personnel behind an L-shield while following the three cardinal principles of radiation safety: time, distance, and shielding wherever possible. The staff were also well versed with the procedure so as to spend as little time as possible during the labeling procedure. They received a mean whole-body radiation dose of 17 μSv per procedure when an average activity of 962 MBq (26 mCi) was handled for an average time of 2 h 35 min, as shown in Table 2 (details in Supplementary Table S2).
Effective Whole-Body Dose and Extremity Dose Received by Radiation Workers and the Time Taken for Each Procedure of Radiolabeling of Leukocytes with 18F-FDG
The mean extremity dose received by the radiopharmacists was 32.78 μSv/procedure for the right hand and 32.18 μSv/procedure for the left hand (Table 1). There was no significant difference between the mean doses received by the two radiation workers.
Viability
The mean cell viability of 18F-FDG-labeled leukocytes, using the trypan blue dye exclusion technique, was found to be 98%.
Stability
The labeled cell suspension was found to be stable up to 4 h, with only 2%–3% of radioactivity found in the supernatant separated from the cell suspension that had been kept at room temperature for 4 h.
Patient studies
18F-FDG-labeled leukocytes were injected into 33 patients. Normal biodistribution of 18F-FDG-labeled leukocytes was primarily noted in the reticuloendothelial system. 18F-FDG-labeled leukocytes were found to concentrate more prominently in the spleen, liver, and bone marrow. Faint urinary bladder, cerebral, and myocardial uptake was seen in WBC PET/CT because of free 18F-FDG, but no gastrointestinal uptake was seen (Fig. 2).

Figure showing biodistribution patterns of 18F-FDG-labelled leukocytes PET/CT and 18F-FDG PET/CT. MIP and fused coronal images of 18F-FDG labelled leukocytes PET CT
Discussion
The concept of in vitro 18F-FDG labeling of leukocytes can be considered an important tool to demonstrate infection. This was demonstrated by the study done by Osman and Danpure. 3 They found that 87% of uptake of 18F-FDG inside a WBC pellet is found in granulocytes and the uptake was dependent on the concentration of glucose in the labeling medium.
Subsequently, many studies were done on humans and animals using the same radiotracer. 6 –10 This provided the rationale of using 18F-FDG-labeled leukocytes for localization of occult infection. In addition, it was associated with the advantages of high specificity of labeled leukocytes and high spatial resolution of PET/CT and significantly reduced imaging time compared with the SPECT-based counterparts (67Ga requires 48–72 h and 99mTc- or 111In-labeled leukocytes require up to 24 h). 10
To the authors' knowledge, this is the first study showing the feasibility of F-18 FDG labeling of leukocytes in a tertiary center without an on-site medical cyclotron and monitoring of personnel during the labeling procedure.
18F-FDG labeling of leukocytes in the current study was a multistep procedure and required around 2.5 h. The leukocyte labeling efficiency is quite variable because of several factors such as proficiency of the radiation worker, blood sampling, volume of plasma obtained, incubation time, and temperature of the reaction. Different studies have quoted different labeling techniques as well as their labeling efficiency.
The labeling efficiency demonstrated in the study by Schauwecker 11 ranged from 24% to 96% (41%). Forstrom et al. 12 reported a labeling efficiency of 62.7%, which was further enhanced to 78.1% by mixing during incubation. In another study done by Rini et al., 10 the mean labeling efficiency of 72% ± 8% for 18F-FDG-labeled leukocytes was reported.
In a study done by Lafont et al., 13 the average labeling efficiency of 18F-FDG-labeled leukocytes in six healthy volunteers was reported as 90.8%. The mean labeling efficiency demonstrated by the current study was 78.01% ± 6.99% (range 51%–92%) in 33 batches, which was slightly lower than that reported by Bhattacharya et al. 5 (81% ± 17%). One of the factors known to be conducive for high labeling efficiency is the requirement of high specific activity of 18F-FDG for labeling leukocytes.
Since Bhattacharya et al. 5 had the advantage of an on-site cyclotron, which allows the usage of high specific activity 18F-FDG, it could be the reason for their higher labeling efficiency compared with that calculated in this study. The authors received 18F-FDG from a commercial cyclotron, and despite all their efforts, a time equivalent to 1.5 half-life of F-18 (∼3 h) would elapse for it to reach their center before the labeling started, which results in slightly lower specific activity. This difference also resulted in the usage of a higher amount of starting activity, 1110 MBq, at their center compared with 370 MBq used by Bhattacharya et al. 5
Despite the lower specific activity, the authors were successful in having a comparable and reasonable average labeling efficiency of 78.01% ± 6.99% and getting a good quality image. The 18F-FDG-labeled leukocytes were injected into patients for evaluation of occult infection and also compared with 18F-FDG to evaluate its incremental value, as shown in Figures 3 and 4; however, the clinical results will be shown in a separate study.

Figure showing superior diagnostic efficacy of 18F-FDG leukocyte PET/CT in finding an additional site of infection. MIP and fused coronal images of the 18F-FDG leukocyte PET/CT scan
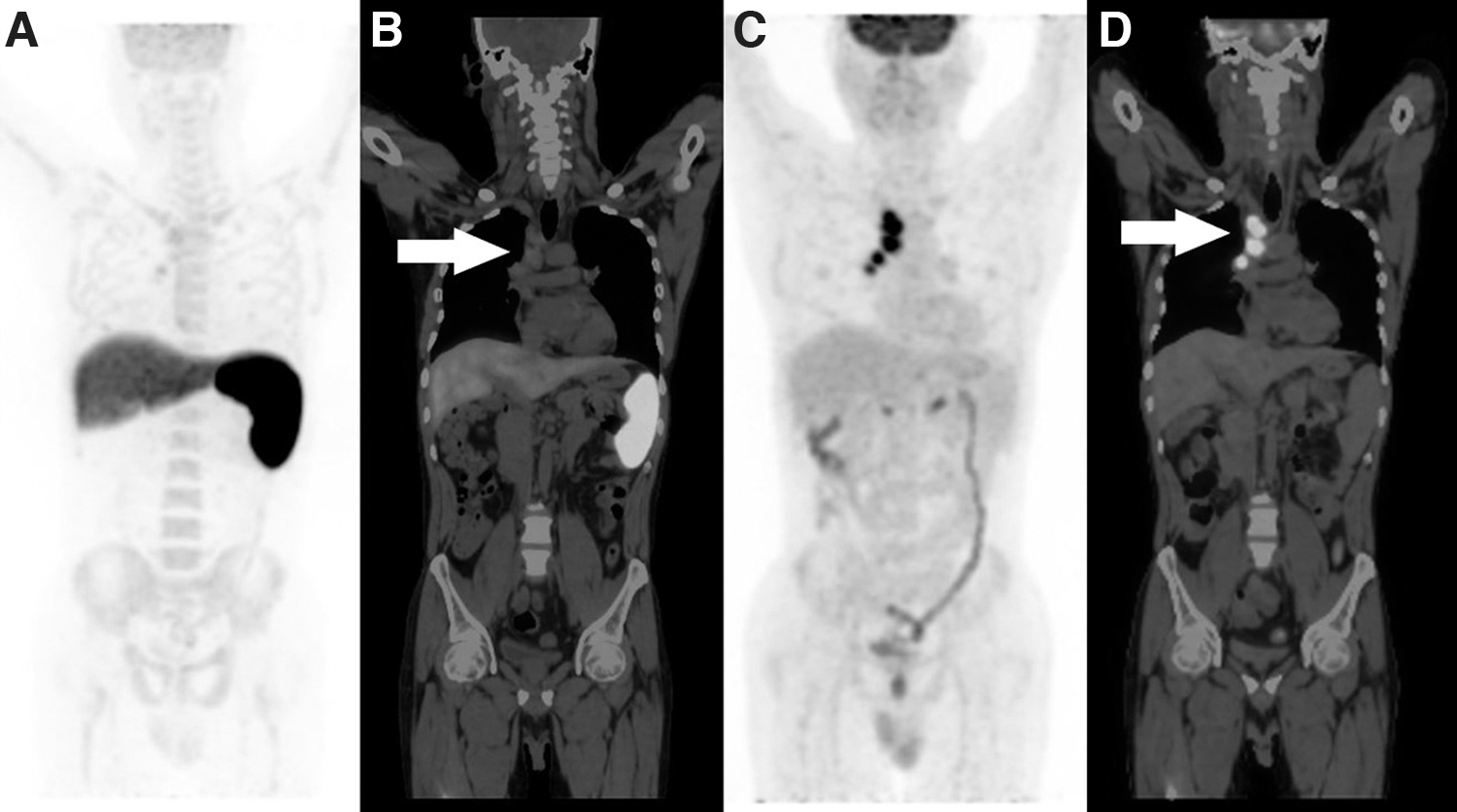
Figure showing superior diagnostic efficacy of 18F-FDG leukocyte PET/CT. MIP and fused coronal images of the 18F-FDG leukocyte PET/CT scan
Nevertheless, the authors emphasize that the diagnostic performance of 18F-FDG-labeled leukocyte PET/CT is higher than the till date gold standard 99mTc-HMPAO owing to the high spatial resolution of PET/CT and early whole-body imaging. In view of the above discussion, the authors can also conclude that labeling of leukocytes with 18F-FDG is also possible at a tertiary health care nuclear medicine setup without the availability of an on-site cyclotron.
In the present study, the mean cell viability of 18F-FDG-labeled leukocytes, using the trypan blue dye exclusion technique, was 98%, which was comparable with that reported by Forstrom et al. 12 (100%) and Bhattacharya et al. 5 (99%).
Since 18F is associated with the emission of very high gamma energy of 511 keV photons and manipulation with the activity can be performed for the longer time of 2–2.5 h, significant radiation exposure to their hands, particularly the fingers, is expected. Therefore, conducting monitoring of radiation workers is of prime importance as it can serve as a guide to determine if any modification is needed in work practices and also to evaluate the numbers of procedures that can be conducted safely per year by complying with regulatory limits.
According to the 2007 recommendations of the International Commission on Radiological Protection (ICRP), the effective radiation dose to personnel should not exceed 20 mSv/y averaged over 5 years or 50 mSv in any year. 14 Whole-body radiation exposure to the staff performing the labeling procedure, as ascertained by the chest electronic pocket dosimeter, varied from 15 to 22 μSv (17 ± 1.4 μSv) and the extremity dose varied from 25 to 36 μSv per procedure. Three factors responsible for the radiation dose are the amount of radioactivity handled, time of manipulation with the radioactivity, and distance at which the radioactivity is held.
Many studies were found in the literature reporting the whole-body and extremity radiation doses incurred by personnel while handling, injecting, and scanning 18F-FDG patients; for example, Zeff and Yester 15 reported a whole-body dose of 8.9 μSv, Chiesa et al. 16 reported 8.5 μSv, Biran et al. 17 reported 7.2 μSv, and Benatar et al. reported 6.5 μSv, 18 but only one study by Bhattacharya et al. 5 was found reporting on the radiation dose received by radiation workers during labeling of leukocytes with 18F-FDG for direct comparison. They also used electronic pocket dosimeters, which were worn at the chest level, and reported a lower whole-body effective dose in the range of 4–10 μSv (5.6 ± 1.4 μSv) received by the staff performing the labeling procedure for each patient.
However, it is difficult to compare these doses between institutes because of the variability in the conditions in each individual facility, such as the procedure, the activity handled, staff proficiency, and shielding devices. The authors could conclude that the major reason for a higher dose in the current study could be the amount of starting activity, which is handled by the staff. The starting activity in the current study was approximately threefold higher than used in the study by Bhattacharya et al. (26.6 ± 2.56 mCi vs. 11.5 ± 1.6 mCi) and hence, higher the radiation exposure.
Even if a higher mean whole-body effective dose of 17 μSv received by an occupational worker during one procedure is considered, it would allow ∼1100 such procedures to be performed per year before reaching the regulatory authority-stipulated annual limit of 20 mSv averaged over 5 years. Thus, assuming six cases per week, potentially 312 procedures per year could be performed, which are far fewer (28%) than the number it would take to reach the allowed limit.
The mean dose to the extremities of a radiation worker was 32 μSv, ranging from 25 to 36 μSv/procedure. If the same radiation worker were to continue to work for a whole year, the worker could perform over 1500 procedures before reaching the threshold for the extremities (50 mSv; i.e., one-tenth of the annual extremity dose limit of 500 mSv). The readings from the chest and wrist thermoluminescent dosimeter badges were 0.5 and 0.56 mSv, respectively, for both the radiation workers engaged in labeling of leukocytes with 18F-FDG as well as the routine departmental work during the 6-month monitoring period.
These doses were well within permissible limits and were not significantly higher than the doses received by workers who performed routine departmental work alone. Therefore, the chances of exceeding the prescribed annual limit for these workers were unlikely in the authors' practice, although staff were always motivated and trained to keep the cardinal principles of radiation safety in mind.
In addition, this study reported comparable doses to the left and right hands as both hands were used equally in the labeling procedure.
Conclusions
This study confirms that labeling of leukocytes with 18F-FDG is possible at a tertiary nuclear medicine setup without the availability of an on-site medical cyclotron, with reasonable labeling efficiency of 78.01% ± 6.99%.
In addition, in-house labeling of leukocytes with 18F-FDG is safe and the radiation doses incurred by the personnel during the labeling procedure are well within the occupational dose limits established by the national regulatory authority.
Footnotes
Acknowledgments
The authors acknowledge Prof. Anish Bhattacharya of the Department of Nuclear Medicine, PGIMER, Chandigarh, and his team who shared the protocol and helped with the labeling technique.
Authors' Contributions
All authors contributed significantly to the content of the article. The manuscript has been seen and approved by all authors.
Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
The study was not funded by any funding agency.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.