
Abstract
Background:
Both everolimus and peptide receptor radionuclide therapy (PRRT) are approved as monotherapies for advanced neuroendocrine tumors (NETs). Research in animal models showed synergism between the two treatment modalities. This study evaluate the safety and efficacy of combining everolimus and PRRT for the treatment of unresectable NETs.
Methods:
Adult patients (≥18 years) with progressing and unresectable histologically confirmed grade 1–2 NETs of all origins were enrolled. Everolimus was started at a 5 mg daily dose and was increased after the initial three patients to 10 mg daily. Patients were treated concurrently with 177Lu-DOTATATE at an 8-week interval, with four cycles planned. Safety was the primary endpoint, with response rate and progression-free survival (PFS) being secondary.
Results:
Eleven patients were enrolled. The trial was terminated early for poor accrual. The median age was 51 years (18–64), and 4 were males. The median number of cycles of 177Lu-DOTATATE was 3, and the median cumulative dose was 300 mCi. The most frequent grade 1–2 toxicities were stomatitis (90.9%) and nausea (72.7%). Less frequent were fatigue (63.6%), anorexia, diarrhea, and skin changes (each at a 36.4% rate). Grade 3 toxicities occurred in 36% (fatigue, infection, pneumonitis, neutropenia, and stroke). No patient developed grade 4 toxicity. Treatment was stopped because of progression in three patients, and toxicity in another three patients; in addition, four patients were halted due to therapy interruption and in one patient who developed stroke. One patient achieved partial response, and nine patients had stable disease. One patient developed disease progression. At a median follow-up of 18.9 months, three patients died and one was lost to follow-up. The median PFS was 23.3 months.
Conclusions:
The combination of everolimus at a dose of 10 mg daily and 177Lu-DOTATATE appears not to be feasible. A larger trial at a lower dose of everolimus is warranted.
Introduction
The treatment of well-differentiated neuroendocrine tumors (NETs) requires a multidisciplinary approach. Treatment modalities might involve surgery, regional therapy, and systemic therapy. The offered therapy will depend on patients' symptoms and disease extent.
Both everolimus and peptide receptor radionuclide therapy (PRRT) were approved as systemic monotherapies for advanced NETs. Everolimus was approved for the treatment of adults with progressive, well-differentiated NETs of pancreatic or gastrointestinal (GI) origin with unresectable, locally advanced, or metastatic disease. This approval was largely based on the results of the RADIANT-2 study, 1 which included patients with advanced GI NETs, the RADIANT-3 study, 2 which included patients with progressive advanced pancreatic NETs, and the RADIANT-4 study, 3 which included patients with advanced, nonfunctional lung or GI NETs. On the contrary, PRRT was approved in January 2018 by the U.S. Food and Drug Administration (FDA) largely based on the NETTER-1 study, 4 after it has been in use for many years in Europe and in other parts of the world.
The combination of both is expected to result in enhanced antitumor efficacy. The preclinical data suggest a synergistic effect of the combination. 5,6 In addition, no overlap toxicities are expected from the combination, which might be taken as reassurance for no added toxicity. Several attempts have been made to combine other systemic therapies with PRRT with variable degrees of success. The systemic therapies used included but are not limited to capecitabine, temozolomide, 5-fluorouracil, somatostatin analogs, liver embolization, and everolimus. 7
This study aimed to evaluate the safety and efficacy of combining everolimus with intravenous radiolabeled lutetium-177 (177Lu)-DOTATATE therapy in the management of advanced-stage and unresectable grade 1–2 NETs.
Methods
Adult patients (≥18 years) with progressing and unresectable histologically confirmed grade 1–2 NETs of all origins were eligible for enrollment. Patients should have measurable disease as per RECIST criteria v1.1, 8 adequate performance status (World Health Organization grade 0–2), and adequate renal, hepatic, and bone marrow function. Patients were required to show tumor somatostatin receptor (SSTR) avidity on either technetium (99Tc) OctreoScan or gallium-68 (68Ga) Dotatate positron emission tomography scans. Patients were excluded if they had received prior everolimus or 177Lu-DOTATATE therapy. Prior octreotide therapy was allowed if within 30 d of registration for the trial.
Patients were treated with everolimus at an oral dose of 10 mg daily. However, to avoid unexpected toxicity, the first three patients were treated at a dose of 5 mg daily, which was escalated to 10 mg thereafter if no dose-limiting toxicity was found. Everolimus can be started within 8 weeks before the first cycle of 177Lu-DOTATATE therapy. The treatment cycle consisted of 4 weeks of therapy. Long-acting octreotide therapy was stopped at least 4 weeks before the administration of PRRT. Patients were treated with 177Lu-DOTATATE up to a cumulative dose of 800 mCi (29.6 GBq). On average, four treatment cycles, each cycle consisting of 100 to 200 mCi (3.7–7.4 GBq), were to be given at treatment intervals of 8 weeks (±1 week) concurrently with everolimus.
Before each administration, patients were to be well hydrated with intravenous fluid followed by intravenous administration of amino acid infusion consisting of a combination of 25 g of lysine plus 25 g of arginine (LysArg) or a commercially prepared mixture of AA (Vamin 18: Fresenius-Kabi) in 500 mL of dextrose 5%/normal saline infused over 8 h. Patients were clinically evaluated every 4 weeks for toxicity according to the National Cancer Institute Common Terminology Criteria V3.
Efficacy evaluation was performed by computerized tomography or magnetic resonance scan every 3 months until disease progression. Response was assessed according to the published Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1. 8 The patient underwent 68Ga-Dotatate scan before each 177Lu-DOTATATE therapy and 177Lu Scan at the end of each 177Lu-DOTATATE therapy. The statistics in calculating the needed number of patients included a proposed response of the combination of 20% compared with the expected 5% with everolimus. The calculated number of patients was 30 given a power of 80 and type 1 of 0.05.
The primary endpoint was safety of the combination, with secondary endpoints including an objective response rate (RR) and progression-free survival (PFS).
All patients signed written informed consent. The protocol was approved by the Research Ethics Committee of the hospital and the Saudi Food and Drug Authority. The trial was registered at
Results
Eleven patients were included from August 2013 to October 2016, and the study had to be terminated because of poor accrual. Patient baseline characteristics are shown in Table 1. Of note, 9 of the 11 patients had gastroenteropancreatic origin. In addition, the liver was involved in 10 of the 11 treated patients.
Characteristics of 11 Patients with Neuroendocrine Tumors Treated with Everolimus and 177Lu-DOTATATE
NET, neuroendocrine tumors; WHO PS, World Health Organization performance status.
No dose-limiting toxicity was seen in the first three patients receiving everolimus 5 mg daily; accordingly, treatment was continued at 10 mg once daily for the rest of the patients. The dose of everolimus had to be reduced to 5 mg daily because of toxicity in three patients. In another two patients, the dose was reduced to 5 mg every other day. Toxicity that led to dose reduction was mostly from everolimus and includes recurrent stomatitis, fatigue, anal fissure. Neutropenia and renal toxicity also lead to dose reduction and could be attributed to both everolimus and 177Lu-DOTATATE. The median number of 177Lu-DOTATATE sessions was three, and the median cumulative administered dose was 300 mCi. The reasons for discontinuation of treatment were as follows: toxicity in four patients, progression in three, and interruption for other reasons in four patients.
No patient completed the four planned cycles of 177Lu-DOTATATE therapy. The most frequent grade 1 and 2 toxicities were stomatitis (90.9%), nausea (72.7%), and fatigue (63.6%). Additional toxicities occurred at a rate of 36.4%, with anorexia, diarrhea, skin, and nail changes. Overall, grade 3 toxicities occurred in 36% and included infection, fatigue, pneumonitis, and neutropenia. One patient developed thrombotic stroke with severe hemiplegia. No grade 4 toxicity was recorded (Table 2). One patient achieved a partial response, and nine achieved stable disease as their best response. One patient had disease progression. At a median follow-up of 18.9 months, the median PFS was 23.3 months (Fig. 1). Seven patients were still alive, three died, and one patient was lost to follow-up. Upon progression, 10 patients received either one or two subsequent lines of therapy, which included chemotherapy, sunitinib, somatostatin analog, everolimus (off trial), radiation, or transarterial radioembolization.
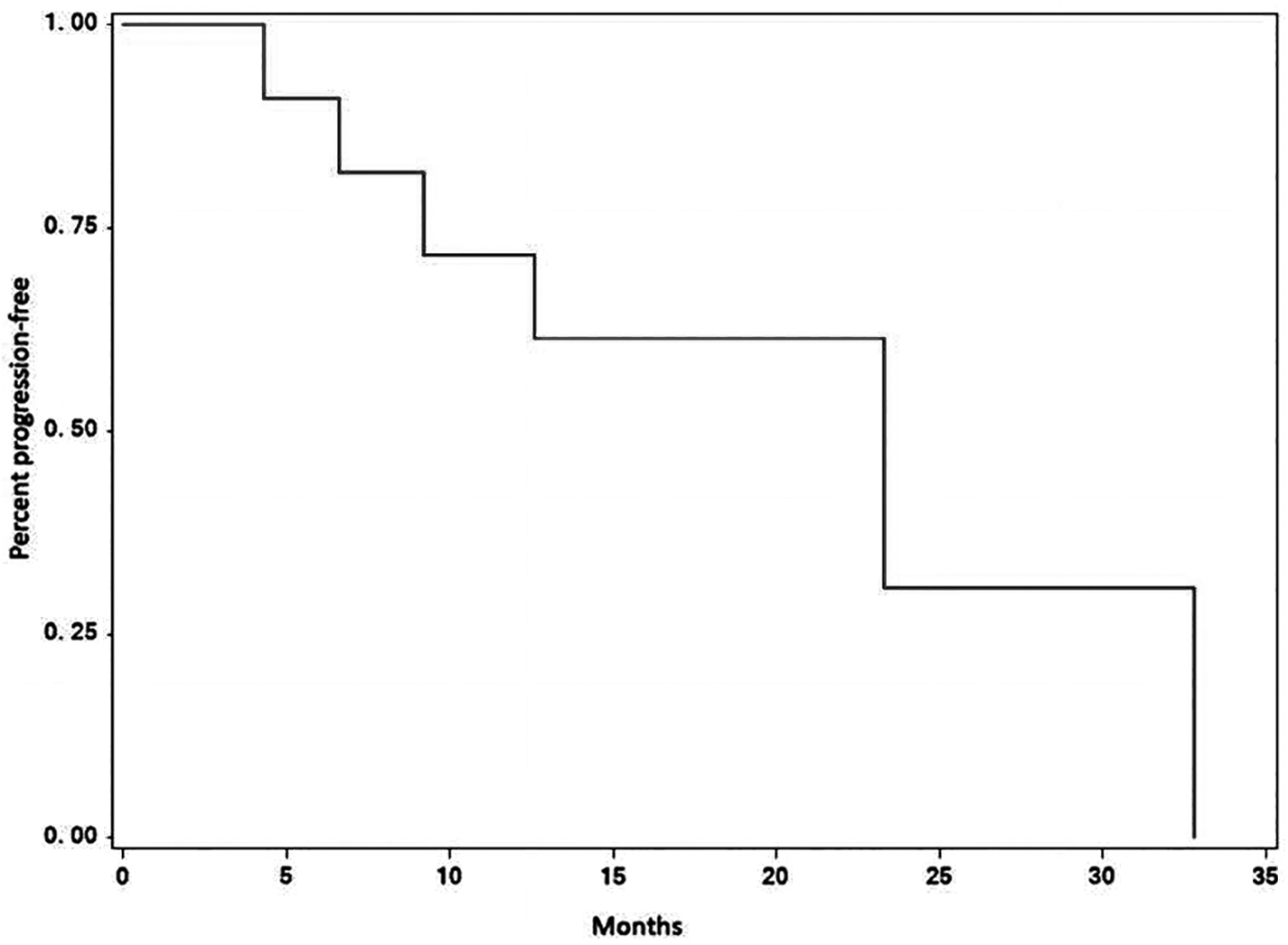
Progression-free survival of 11 patients with NETs treated with everolimus and 177Lu-DOTATATE. NETs, neuroendocrine tumors.
All-Grade Toxicities in 11 Patients with Neuroendocrine Tumors Treated with Everolimus and 177Lu-DOTATATE
Discussion
Everolimus has shown activity in various subtypes of NETs, as seen in several studies. In the RADIANT-3 trial, patients diagnosed with progressive advanced pancreatic NETs were randomized to everolimus or placebo. The results confirmed an increase in PFS by 6.4 months (from 4.6 months with placebo to 11 months with everolimus; hazard ratio [HR] 0.35, confidence interval [95% CI] 0.27–0.45; p < 0.001). 2 There was a nonsignificant trend toward overall survival benefit. 2
The RADIANT-4 trial 3 included patients with NETs of GI and lung origin. Patients were randomized to everolimus 10 mg versus placebo. The median PFS was 11 months in the everolimus group and 3.9 months in the placebo group [HR 0.48, 95% CI 0.35–0.67; p < 0.00001]. Reported all-grade toxicity in this trial compared with the RADIANT-4 trial showed more stomatitis (91% vs. 60%), fatigue (72.7% vs. 30%), and infections (45.4 vs. 29%), but similar rates of diarrhea (36% vs. 30%), noninfectious pneumonitis (18% vs. 16%), and hyperglycemia (9% vs. 10%). 3
PRRT has been shown to be effective for patients with progressive SSTR-positive NETs. The multicenter prospective phase III NETTER-1 trial 4 evaluated the efficacy of 177Lu-DOTATATE (given as 7.4 GBq every 8 weeks, four intravenous infusions) in combination with 30 mg octreotide long acting release (LAR) versus 60 mg octreotide LAR alone (every 4 weeks) in patients with progressing advanced well-differentiated midgut NETs. The findings showed the superiority of 177Lu-DOTATATE to high-dose octreotide in PFS, with 30 events occurring in the 177Lu-DOTATATE arm compared with 78 in the octreotide arm at the time of the updated analysis (HR 0.21, 95% CI 0.14–0.33 p < 0.0001).
The median overall survival at a median follow-up of >76 months was 48.0 months in the 177Lu-DOTATATE arm and 36.3 months in the control arm. The HR was 0.84 (95% CI 0.60–1.17), with nonstatistically significant p = 0.30. RR was also higher in the 177Lu-DOTATATE arm (18% vs. 3%). Treatment was also associated with a symptomatic improvement and time to quality-of-life deterioration in several scales, including global health status, physical functioning, fatigue, pain, and diarrhea. 9
Treatment with 177Lu-DOTATATE is generally well tolerated; however, in 3%–4% of patients, an irreversible bone marrow toxicity, such as leukemia or bone marrow dysplasia, might develop. Mild renal injury, which could be long term, has been reported in 30% of patients. 10
Everolimus has been found in previous reports to have radiosensitizing activity in cell lines from breast, 11 colon, and pancreatic cancers. 12 Multiple preclinical studies have been conducted to evaluate both the safety and efficacy of the combination of everolimus and PRRT and to understand the mechanism of synergism at the cellular level. One study by Bardram et al found that a combination treatment with 177Lu-DOTATATE and everolimus had a greater antitumor effect in mice than the agents administered separately. 5 In addition, Prasad et al concluded in their study that mTOR inhibitors were able to enhance radiosensitivity in three out of five NET cell lines. 6
On the contrary, other investigators showed that the combination treatment was less effective compared with PRRT alone in an in vivo rat tumor model. 13 The theoretical explanation by the authors is that everolimus might have resulted in immune suppression and therefore progression of disease. 14 The combination has been expected to enhance antitumor efficacy, and because of the lack of overlap in toxicities between everolimus and PRRT, the toxicity was expected to be fair and manageable. A phase I study (NETTLE study) 15 explored the safety of the combination when 16 patients were treated in three successive cohorts with everolimus daily doses of 5, 7.5, and 10 mg. The maximum tolerated dose was 7.5 mg. Everolimus was given for only 24 weeks, from cycle 1 to cycle 4 of PRRT. The most common toxicity was hematological. Seven patients (44%) achieved a partial response. No one progressed during the 24-week treatment period.
This study was terminated after enrolling 11 patients because of poor accrual attributed to the rarity of the disease in addition to the strict inclusion criteria, which allowed only a small fraction of screened patients to be enrolled. Another factor for poor accrual was being a single-center study.
In this study, the first three patients treated with everolimus at 5 mg daily experienced no dose-limiting toxicity. Hence, the dose was escalated in the rest of the patients to 10 mg daily. However, it appears that 10 mg of everolimus combined with 177Lu-DOTATATE at the specified dose was not well tolerated. This is evident by the required dose reduction to 5 mg in three patients and to 5 mg every other day in another two patients (2.5 mg daily) in addition to the no dose-limiting toxicity encountered in the first three patients who received everolimus at a dose of 5 mg daily In addition, none of the patients was able to finish the four planned doses of 177Lu-DOTATATE therapy.
This is supported by the finding that only one out of the three patients who received everolimus at 10 mg in the NETTLE study was able to finish the four planned doses of 177Lu-DOTATATE therapy, while 10 of the 13 patients who received everolimus at 5 or 7.5 mg daily completed the four planned doses. 15 The toxicity profile of the combination in this study was nonoverlapping. The most common toxicities were GI toxicity and fatigue, and they were mainly everolimus-related toxicities. Four out of 11 patients (36%) developed grade 3 toxicities, and no one developed grade 4 toxicities. However, it appears that there was an increase in the incidence of all the grade toxicities, as evident by the 90% incidence of stomatitis, 72.7% incidence of nausea, and 63.6% incidence of fatigue. The lower 177Lu-DOTATATE-related toxicity in this study might be related to the lower dose used compared with the NETTER 1 trial.
In the NETTER-1 trial, 4 where patients were treated with only 177Lu-DOTATATE PRRT, 41% of the patients developed grade 3 or 4 toxicities. On the contrary, the RADIANT-32 and RADIANT-43 trials reported grade 3–4 toxicities in 37.7% and 45.5% of the patients, respectively. The importance of selecting an appropriate dose for systemic therapy when combined with PRRT has also been illustrated by Nicolini et al. In their study, patients with advanced gastroenteropancreatic NET were treated with the combination of 177Lu-DOTATATE and metronomic dose of capecitabine at 1500 mg per day. Thirty-seven patients received the above therapy, 17 of them had to have a dose reduction of capecitabine to 1000 mg per day, and 30 completed the planned PRRT. 16
This study protocol was strict about patient compliance with therapy and prompted removal from the study for nonadherence to the timing of 177Lu-DOTATATE treatment or for interruption of everolimus treatment for more than a certain duration. Four out of 11 patients (36%) were removed from the study due to interruption of therapy, which might have resulted in undertreatment and therefore a lower overall RR. One patient (9%) achieved a partial response, and nine patients (82%) maintained stable disease, in contrast to 44% achieving a partial response in the NETTLE study. 15 In the NETTER-1 trial, 4 the overall RR was 18%.
This study has many limitations. Most importantly, the premature closure of the trial resulted in a small number of patients. In addition, it was a single institutional trial that resulted in poor patient accrual.
Conclusions
The combination of everolimus at a dose of 10 mg daily and 177Lu-DOTATATE PRRT appears not to be feasible in this patient population. However, a larger study examining the combination with a lower dose of everolimus is warranted. Since this study did not reach the target accrual, the above conclusion should be considered only for the purpose of hypothesis generation.
Footnotes
Acknowledgments
The authors wish to thank Ms. Leilani Cabangon for the excellent job of coordinating all aspects of the study. They also thank Novartis Pharmaceuticals for funding this investigator-initiated study.
Authors' Contributions
All authors contribute equally to this work and are in agreement with the article.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Disclosure statement
No competing financial interests exist.
Funding Information
This study was supported by a grant from Novartis Pharmaceuticals (grant number: CRAD001KSA04).