
Abstract
This review discusses the strategies of preclinical studies intended for accelerator-based (AB)-boron neutron capture therapy (BNCT) clinical trials, which were presented at the National Cancer Institute (NCI) Workshop on Neutron Capture Therapy held from April 20 to 22, 2022. Clinical studies of BNCT have been conducted worldwide using reactor neutron sources, with most targeting malignant brain tumors, melanoma, or head and neck cancer. Recently, small accelerator-based neutron sources that can be installed in hospitals have been developed. AB-BNCT clinical trials for recurrent malignant glioma, head and neck cancers, high-grade meningioma, melanoma, and angiosarcoma have all been conducted in Japan. The necessary methods, equipment, and facilities for preclinical studies to evaluate the biological effects of AB-BNCT systems in terms of safety and efficacy are described, with reference to two examples from Japan. The first is the National Cancer Center, which is equipped with a vertical downward neutron beam, and the other is the University of Tsukuba, which has a horizontal neutron beam. The preclinical studies discussed include cell-based assays to evaluate cytotoxicity and genotoxicity, in vivo cytotoxicity and efficacy of BNCT, and radioactivation measurements.
Introduction
Mechanisms of boron neutron capture therapy
The mechanism of action of boron neutron capture therapy (BNCT) is as follows: first, a boron drug containing high levels of 10 B is administered to patients, which later accumulates in cancer cells; tumors are then irradiated with a neutron beam consisting mainly of epithermal neutrons. These epi-thermal neutrons lose energy in the body to become thermal neutrons; 10 B captures the thermal neutrons and undergoes an (n,α) reaction, producing α particles with a range of 9–10 μm and 7 Li nuclei with a range of 4–5 μm. These highly charged LET particles selectively kill cancer cells.
The neutron beam contains a mixture of fast neutrons, thermal neutrons, and γ-rays, including recoil protons produced by the elastic scattering of fast neutrons and hydrogen, protons produced by the (n,p) reaction of thermal neutrons with nitrogen, and dose delivery by γ-rays, although this is smaller than the dose delivered by the (n,α) reaction of thermal neutrons and 10 B. The two boron agents used in clinical studies are sodium borocaptate (BSH) and P-boronophenylalanine (BPA). BSH is used in the treatment of brain tumors, and accumulates by passive diffusion into the stroma at locations where the brain-blood barrier is disrupted. BPA, on the other hand, is taken up via L-Type Amino Acid Transporter 1 (LAT1); accumulation is specific as LAT1 expression is higher in various cancer types than in cells of normal tissue. 1
BPA was first shown to be effective in a clinical study of melanoma by Mishima and Kondoh, 2 and was later also reported to be effective in head and neck cancer and brain tumors. 3 Various other boron agents have been investigated and developed, but have not yet reached clinical practice, the details of which, can be found in other review articles. 3 In contrast to other particle beam therapies, such as proton beam and carbon beam that use the Bragg peak feature to physically concentrate the dose on the cancer tissue, BNCT is a particle beam therapy that uses the biological feature of selective boron drug uptake by the tumor to deliver the dose to the cancer tissue. There are high expectations for BNCT against tumors such as malignant gliomas, which are highly invasive to normal tissues and difficult to control with other particle therapy methods.
BNCT clinical progress
In 1951, the first BNCT was performed at the Brookhaven National Laboratory (BNL) in the United States. The subject was a patient with glioma. From then until 1961, 63 patients were treated with BNCT at the BNL and the Massachusetts Institute of Technology (MIT). 4 After 1994, BNCT treatment was resumed using BPA at the epithermal neutron irradiation facility, but was suspended in 2003. 5 In Japan, basic research on BNCT started in 1959, and since 1968, Hatanaka and Nakagawa have performed BNCT of malignant gliomas using BSH at the Hitachi and other reactors, achieving a median survival time of 640 d in glioblastoma patients. 6 In 1987, after the success of preclinical study on malignant melanoma in both tumor-inoculated hamsters and spontaneous melanoma in pigs, 7 Mishima and Kondoh started clinical melanoma treatment using BPA. 2 As BPA is taken up by other cancer types, it has become a central agent in BNCT. 3
After the completion of the setting up for the epithermal neutron irradiation field, performance of BNCT resumed in the Kyoto University Research Reactor (KUR) and Japan Atomic Research Inst. Reactor (JRR-4) in the early 2000s. BNCT with epithermal neutrons was also started in European reactors in the late 1990s, 8,9 including in the Finnish reactor until 2012. Basic research began in Argentina, Korea, Taiwan, China, and Thailand, in the early 1990s. In 2003, BNCT for melanoma using mixed thermal and epithermal neutron irradiation was initiated in Argentina, yielding good results with an overall response of 69.3% and acceptable toxicity. 10 In 2010, a clinical trial for BNCT against head and neck cancer was started in Taiwan, 11 and BNCT for recurrent malignant brain tumors, including the brainstem, is also being performed. 12,13
At the Institute for Integrated Radiation and Nuclear Science, Kyoto University (KURNS), BNCT clinical studies were conducted from May 1974 to January 2020 at the KUR Heavy Water Neutron Irradiation Facility. More than 500 patients with BNCT have been treated for malignant and refractory brain tumors, head and neck cancer, liver cancer, malignant cutaneous melanoma, and mesothelioma. Among them, the median survival time of newly diagnosed glioblastoma treated with a combination of BNCT and X-ray was 23.5 months, while that of recurrent malignant glioma was 10.8 months after BNCT. 14 The median overall survival and progression-free survival of refractory and recurrent high grade meningioma were 29.6 months and 13.7 months after BNCT, which were superior compared with phase II clinical trial of sunitinib for patients with similar backgrounds (24.6 and 5.2 months, respectively). 15 The median survival time of recurrent and unresectable head and neck cancer post BNCT was 10.1 months, and the 2 year overall survival rate was 24%. 16 The overall control rate (CR + PR without recurrence) of the BNCT for cutaneous melanoma was 88% (7/8). 17
In 2008, the Cyclotron Irradiation System for BNCT (C-BENS) was installed at KURNS in collaboration with Sumitomo Heavy Industries Ltd. In this system, protons are accelerated to 30 MeV using a cyclotron, and neutrons are produced by the 9 Be (p,n) 9 B reaction. 18 Phase I/II clinical trials using this system for malignant glioma and recurrent head and neck cancer were conducted from October 2012 to April 2018. 19 –21 For recurrent malignant glioma, the 1-year survival rate and median OS of the recurrent glioblastoma cases were 79.2% and 18.9 months, respectively, while the occurrence of adverse events, such as brain edema, was well controlled by bevacizumab. 19 For head and neck cancer, the overall response rate for all patients was 71%, while the complete response/partial response rates were 50%/25% in recurrent squamous cell carcinoma (R-SCC) and 8%/62% in recurrent/locally advanced non-squamous cell carcinoma R/LA-nSCC, respectively. The 2-year overall survival rates for R-SCC and R/LA-nSCC were 58% and 100%, respectively. 21 In 2020, this system was approved as a medical device named NeuCure, and treatment for head and neck cancer using the same system covered by insurance was started at the Southern Tohoku BNCT Research Center and Kansai BNCT Medical Center.
Unlike reactor neutron sources, accelerator neutron sources can be installed in hospitals and are being developed by various research groups. In Japan, the C-BENS at KURNS, the National Cancer Center, the University of Tsukuba, Nagoya University, and others have developed accelerator neutron sources. The National Cancer Center is currently conducting clinical trials for malignant melanoma and angiosarcoma. 22 Outside of Japan, the accelerator is being developed in Finland, Russia, Argentina, China, South Korea, Taiwan, and other countries. In Finland, clinical trials are still in the preparation stage. 23,24 A variety of accelerators that are already conducting or will soon conduct BNCT clinical trials are listed in Table 1.
Current Status and Performance of Accelerators Intended for Boron Neutron Capture Therapy Clinical Trials
Preclinical studies using BNCT accelerators in Japan
In addition to the investigation of other pharmaceuticals and medical devices, as a preliminary step to conducting accelerator BNCT clinical trials on patients, preclinical studies using cells and animals should be conducted to demonstrate the biological efficacy and safety of accelerator-based (AB)-BNCT in accordance with the regulations and standards of the respective countries. To conduct preclinical studies, facilities, equipment, and researchers are needed to safely conduct biological experiments using biological specimens that have been activated after neutron irradiation. To expand the application of BNCT to various organs, it would be desirable to demonstrate its safety and efficacy in preclinical studies. Before BNCT clinical trials using C-BENS, in vitro and in vivo experiments with relevant cancer cell lines were conducted at the KURNS, (then known as the KUR Institute) and the biological effects of BNCT were confirmed by these preclinical studies. At that time, the BPA used in the accelerator BNCT trial was not approved by pharmaceutical affairs bodies in Japan. Stella Pharma Corporation (Osaka, Japan) provided good manufacturing practice (GMP)-grade BPA for preclinical and clinical trials as part of a corporate clinical trial, which was filed and approved as borofalan 10 B), a boron drug for BNCT, in 2020.
The contents of preclinical studies in two Japanese facilities, the National Cancer Center and the University of Tsukuba's Proton Beam Therapy Center, which are currently conducting studies for accelerator BNCT clinical trials, are discussed below as reference examples.
Preclinical Studies of AB-BNCT System Utilizing the Vertical Downward Neutron Beam
Although the irradiation geometry of horizontal neutron beams has been predominantly used in reactor-based BNCT systems for biological and clinical trials of BNCT research, the geometry of a vertical downward thermal beam was initially set up in the Massachusetts Institute of Technology Research Reactor (MITR), which was originally constructed for NCT. This horizontal beam port was only later set up for converter-based epithermal neutron beam irradiation. Therefore, there is a paucity of accumulated experience in preclinical studies for vertical downward neutron beams. For the AB-BNCT system, the National Cancer Center in Japan 22 and Novosibirsk State University in Russia 25,26 have been constructed for the irradiation geometry of vertical downward epithermal neutron beams (Table 2).
The Facilities of Boron Neutron Capture Therapy Systems with Vertical Downward Neutron-Beam
AB-BNCT, accelerator-based-boron neutron capture therapy.
The safety and efficacy of BNCT should be confirmed in the preclinical evaluation of AB-BNCT for use as basic data in clinical trials. Therefore, both cells and animals should be used in experimental systems. However, middle- and larger-sized animals are difficult to use frequently because of regulations on radioactivation levels and medical laws. Small rodents, such as mice, with a specific pathogen-free (SPF) state, are more convenient for use in preclinical studies. However, unavoidable differences exist between small rodents and humans, such as tissue and organ positioning, biological properties of tumors and normal tissues, distribution profiles of boron carrier drugs, and sensitivity to radiation. Therefore, consultation with regulatory authorities is necessary before starting preclinical evaluation.
General schemes of preclinical study plans require the actual planning of clinical trials for specific cancer types. Preparation of GMP-level drugs is necessary, as is planning a close-to-good laboratory practice (GLP) level facility and management setup. For safety evaluation, cell-based and animal model studies should be planned. AB-BNCT system generates neutron beam and the neutron itself has biological effects, because of recoiling hydrogen nuclei produced by collisions with fast neutrons: [1H(n,n’)1H]. Therefore, the relative biological effect (RBE) of neutron beam (hydrogen dose) should be evaluated as one of the doses besides boron dose, nitrogen dose, and γ-ray dose. Determination of the neutron (hydrogen) dose RBE for a specific AB-BNCT system is necessary for dose calculations.
Cytotoxicity and genotoxicity in the absence and presence of boron drugs can be tested using several cancer-cell lines, ideally in normal cells. With animals, such as SPF mice, local and systemic toxicities in the acute phase and long term can be evaluated. The design of irradiation geometry and shielding materials for neutron beams and checking the radioactivation level of animals after a neutron beam is also necessary.
Cancer cell killing assays and tumor xenograft models can be used to evaluate the efficacy of BNCT. For long-term observation of late treatment effects, it may be necessary to transfer the animals from irradiation facilities, such as medical facilities, to outside facilities where close-to-GLP level observation is possible, although it is required to check the radioactivity level of the animals beforehand. The above-mentioned safety and efficacy evaluation of the AB-BNCT system should be conducted in comparison with other radiation treatments, usually photon beam irradiation. Therefore, in AB-BNCT preclinical studies, the same series of experiments should be simultaneously planned and conducted with photon-beam irradiation.
For Preclinical Studies of CICS-1 at the National Cancer Center
The BNCT system CICS-1 installed at the National Cancer Center Hospital (NCCH) has a linear accelerator and a solid-lithium target with irradiation set-up of a neutron beam in the vertical downward direction. The beam port is 22 cm in diameter. For the AB-BNCT system CICS-1, a phase I study investigating treatment for malignant cutaneous melanoma and angiosarcoma was planned with the use of BPA-based boron drugs. 22 Preclinical studies should be designed to fit these diseases. Skin damage should be evaluated because the treatment of skin cancers was planned for the clinical trials; however, mucosal damage is not expected in the clinical trials, so it was considered possible to omit to measure mucosal damage as readout from preclinical studies.
Cell-based models
For safety and efficacy, cell-based experiments to determine the RBE of neutron beams (hydrogen dose) were planned. Cell survival was assessed by colony formation assay to measure cytotoxicity, and micronuclei measurements for the evaluation of genotoxicity as end points were planned. Angiosarcoma is a rare cancer, and it is difficult to obtain established human angiosarcoma cell lines; however, melanoma cell lines could be included. Survival of melanoma and other cancer cells by clonogenic colony formation assays can be carried out both in the absence and presence of different concentrations of boron compounds. Micronuclei evaluation has also been used to assess the genotoxicity of chemicals and radiation. 27,28 After neutron irradiation in the presence of boron compounds, an increase in the frequency of micronuclei was observed in a boron concentration-dependent manner in cancer cells, as previously reported for a nuclear reactor-based BNCT system.
Animal models
For safety evaluation with animal models, small rodents and larger-sized animal models 26,29 are usually necessary to evaluate the in vivo toxicities associated with chemo-radiotherapies; however, because abundant evidence in the form of clinical trial data with reactor-based BNCT with BPA has been accumulated and consideration of biological differences in risk organs and tissues may be possible, it was considered reasonable to carry out only mouse experiments for preclinical studies.
Radioactivation of mice
Dr. Satoshi Nakamura of the NCCH investigated the radioactivation levels of C57BL/6 mice strain after 60 min of irradiation with CICS-1 under therapeutic conditions. 24Na, 38 Cl, 42 K, 56Mn, 80mBr, and 82Br were the predominant radioactivated nuclides. 30 24Na showed the highest contribution to the dose rate, which agrees with a previous report. 31 The saturated radioactivity of a mouse was confirmed to be below the lower limit of the IAEA regulations. 32
Effect of local irradiation on hematological profiles and skin damage
The effect on hematological profiles, including white blood cells, red blood cells, and platelet counts after local irradiation of the hind legs using 6 LiF containing shielding plates in the absence and after administration of boron drug could be investigated. Skin doses may be the limiting dose for the treatment of skin cancers in clinical trials; therefore, pre-planned skin doses for clinical trials were considered reasonable to observe in mouse models. Skin damage can also be assessed using the reported skin damage score. 33
Biological effects in- and outside of irradiation field
Since the downward vertical irradiation beam is utilized in the BNCT system, biological effects inside and outside the irradiation field were investigated by measurement of cell survival using colony formation assay, and then with mouse models by whole body irradiation with neutron beam in the absence or after the administration of the boron drug. Hematological profiles were further evaluated. Examples of measuring the effect on the irradiation field and the surrounding area are shown in Figure 1. Mice were placed in plastic cases without anesthesia.

Geometry for the evaluation of biological effects in- and out-of-field of neutron beam irradiation of the AB-BNCT system with a vertical downward neutron-beam. AB-BNCT, accelerator-based-boron neutron capture therapy.
Biological effects of beam-depth direction
To evaluate the biological effects of the beam-depth direction effect, measurement of intestinal crypt regeneration on day 3.5 can be performed. This measurement has been extensively used to obtain in vivo RBE values of photon beams and proton, carbon-ion, and epithermal neutron beams (without the addition of boron drug) for BNCT. 34 We applied this measurement of intestinal crypt regeneration both in the absence and following administration of boron drug to assess the RBE in comparison with gamma irradiation. These RBE values can be used for comparison with other AB-BNCT systems, other particle beams, or gamma/x-irradiation. Previously, the Balb/cA mouse strain was used for this purpose; however, we used C57BL/6 mice because this strain is easily available and its radiation sensitivity is lower than that of the Balb/cA strain. 35 Our experiments validated that the C57BL/6 strain can be used for this purpose.
The effects on hematological profiles can be simultaneously measured to confirm the biological effects in the beam depth direction. We measured the effect of neutrons and BNCT in the beam-depth direction using three layers of the mouse model, as shown in Figure 2. Mice were administered BPA at a dose of 500 mg/kg body weight 30 min before irradiation. The small intestine was divided into 10 sections, and the crypt numbers were counted. The crypt number can be expected to decrease the most at the top position, and the effects are expected to be less dependent on the depth.
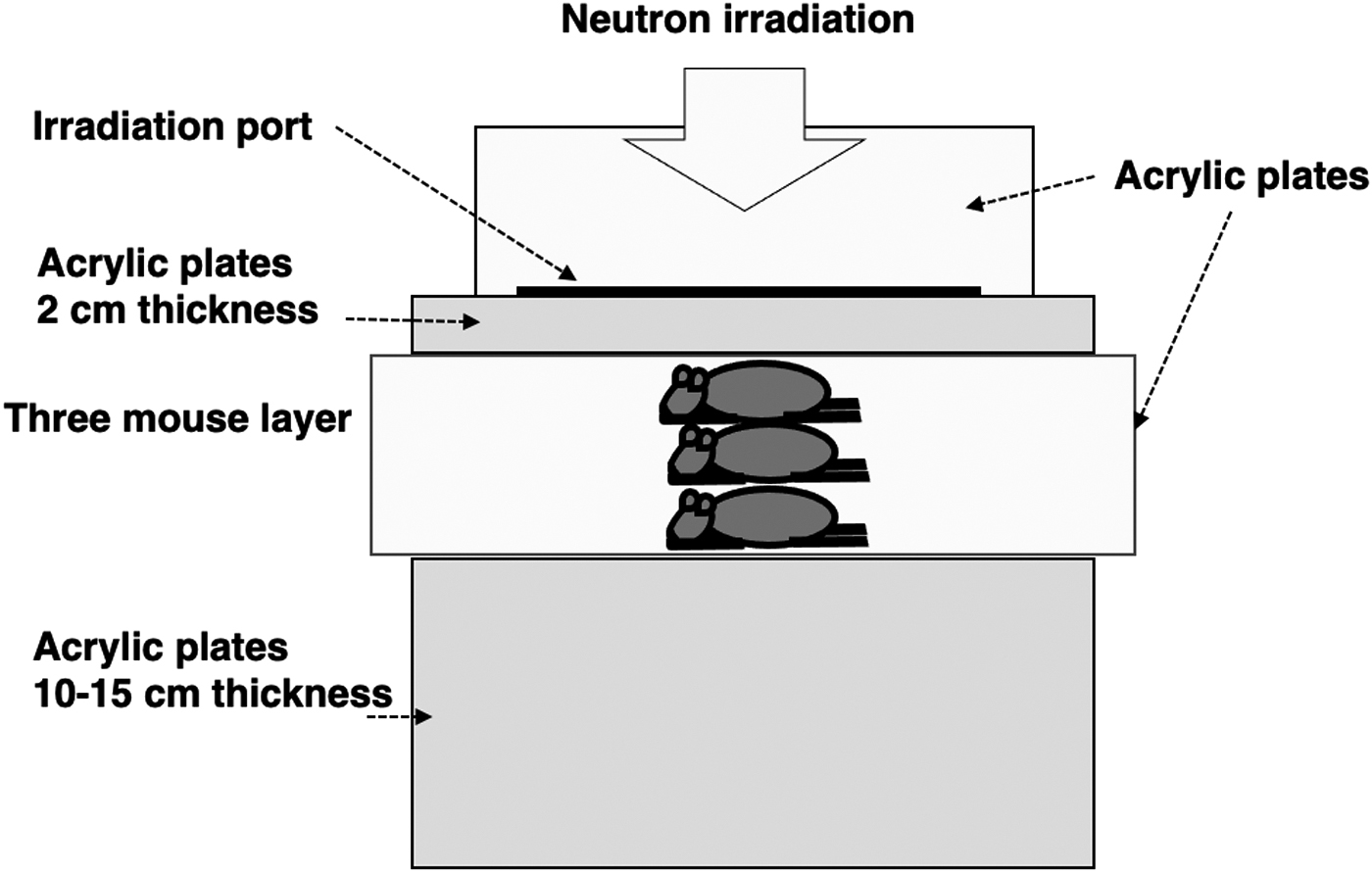
Geometry for the evaluation of biological effects of beam-depth direction of AB-BNCT system with vertical downward neutron-beam.
Xenograft treatment models for efficacy evaluation
To assess the in vivo efficacy of BNCT, its effect on tumor growth delay can be tested, including on melanoma xenograft models in the absence and after administration of boron drug by local irradiation of neutron beam in comparison with local gamma/x-irradiation. Other tumor cell types can be included in these evaluations, and analysis of tumor growth delay and evaluation of tumor histopathologic characterization can be conducted.
Progress in Nonclinical Trials Using a Newly Developed Accelerator Neutron Source at the University of Tsukuba
At the University of Tsukuba, a reactor-based BNCT clinical study was started in 1994. 36 The neurosurgery group first performed intraoperative neutron irradiation using thermal neutrons, followed by non-craniotomy irradiation using epithermal neutrons. A previous case study of glioblastoma treated with BNCT was reported by Yamamoto et al in 2009. 37,38 Although this was a study of a small number of cases, a survival benefit was observed compared with standard treatment at the same time. However, fuel problems in nuclear reactors and the Great East Japan Earthquake of 2011 have greatly hindered the use of nuclear reactors.
The newly developed neutron source of the University of Tsukuba
The Ibaraki Prefecture, Tsukuba University, High Energy Accelerator Research Organization (KEK), and other organizations have started to develop a new neutron source that does not depend on nuclear reactors. A novel AB neutron source was established, and a proton beam of 2.1 mA current to the target became continuously available from 2019 (Table 1). The tentative name of this source is iBNCT. 38 Figure 3 shows the schema of the iBNCT system, including the building, beam transport system, irradiation room, and accelerator. This system uses a linear accelerator, a beryllium target, and 8 MeV proton beams, and is designed to achieve low activation and high power. Since its initiation in 2015, the project has gradually increased the current while correcting problems, and is now operating stably at a stable output power for everyday treatment. 39 Preclinical studies are currently being conducted with the aim of achieving approval from the Pharmaceuticals and Medical Devices Agency to progress into clinical trials.

iBNCT Facilities. The upper left panel
Preparations and measures for non-clinical studies
The planned physical measurements are listed below:
• Distribution study for neutron flux and gamma ray dose
The neutron detector consisted of gold wires, and the gamma ray dose rate was measured using thermoluminescence dosimeters. A water phantom was used to measure the spatial distribution by placing detectors.
• Leakage radiation with whole body phantom.
The whole-body phantom was set up at the beam port to estimate the leakage of radiation outside the beam port. Detector measurements and Monte Carlo simulations were subsequently performed.
• Residual gamma dose after mice irradiation
Seven minutes after the accelerator stopped, the residual gamma dose rate was measured around the beam port. The residual gamma dose of iBNCT was 40 μSv/hr.
We are currently in the process of starting biological experiments, and nonclinical studies are being conducted as a preparatory step for clinical trials. However, several issues arose that still need to be resolved during the laboratory-setup phase.
First, non-clinical studies require the handling of un-sealed radioisotopes (RIs). Irradiated animals would be activated and must be treated with unsealed RIs. Radiation control regulations differ in each country, but in Japan, the handling of living and unsealed sources requires a very special environment. Laboratory equipment needs to be improved before conducting experiments with living, unsealed sources. In the facility, an exhaust system for handling RIs and a system for storing and draining the activated liquid are both needed. Equipment for safety cabinets for researcher safety is also necessary. The procedures require notification of changes in the use of RIs to the central ministry and approval. This is a difficult procedure depending on the type of nuclide used. In principle, RIs can be used and disposed of without being removed from the radiation-controlled area. To remove RIs from the laboratory, the facility must be licensed to manufacture and sell RIs, and the recipient must be able to handle RIs.
Facilities for conducting animal experiments must be equipped inside the radiation-controlled area to handle RIs. Drafts must be established for the use of anesthetics and toxic substances. All facilities for the biological experiments were set up in a radiation-controlled area. Radiation contamination inspections are required before any items are taken out of the laboratory; as a rule, irradiated items may not be taken out of the laboratory. As a facility, an SPF level clean breeding environment, registration of laboratory animal breeding facilities, and the Animal Experiment Plan were approved by the Ethics Committee of our university. The animal breeding facility was equipped with temperature and humidity control, data log storage, and automatic lights on and off. Disposal cages were used for decontamination.
Normally, procedures and steps are required to move the RIs if they are housed in a different building or location once they leave the radiation-controlled area. The iBNCT facility had a biological experimental area directly above the irradiation room. Therefore, we installed a 20 cm-wide passageway through the ceiling separating the upper and lower sections and a manual winch to raise and lower the cages. This allows animals and cells to be moved into the biological experimental area without leaving the radiation-controlled area.
Figure 4 shows the atmospheric pressure configuration of the biological laboratory area. The animal breeding rooms have the highest negative pressure, front rooms have medium pressure, and the working rooms have low negative pressure. This prevents scattering of radiolabeled materials to the outside. The histopathological examination could not be performed within the radiation-controlled area. Because the analysis of tissue samples inevitably requires that samples be taken outside the facility once, and to conduct the experiment under GLP standards, we established a multi-center GLP experiment implementation system that allows for the sale of RI and the transfer of specimens with collection and disposal (Fig. 5). The consulting company and the University of Tsukuba decided to separate the work and conduct it as a multi-testing site. The University of Tsukuba will be responsible for animal care and measurement, while the company will conduct the GLP test, drug administration, blood sampling, and others.
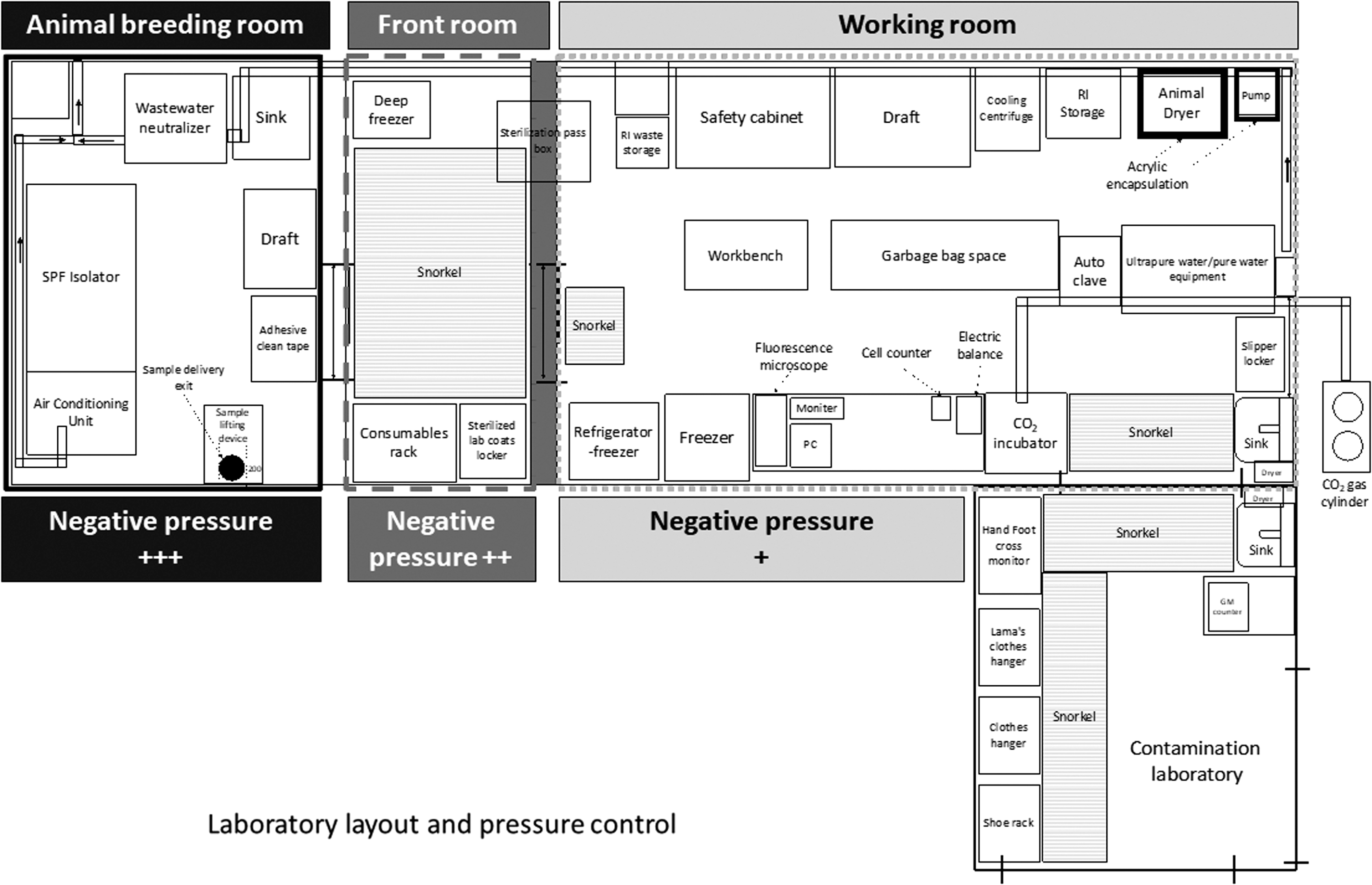
Atmospheric pressure configuration of the biological laboratory area. The animal breeding rooms have the highest negative pressure, front rooms have a medium pressure, and the working rooms have a low negative pressure.

Diagram of the organization of multiple laboratories. The consultation company is responsible for the implementation and assurance of GLP. Since pathological studies cannot be performed at the University of Tsukuba facility due to the lack of facilities and expert staff, the RI is sold from the university to the company and collected and disposed of at the University of Tsukuba after completion of the study. GLP, good laboratory practice; RI, radioisotopes.
Radioactive waste is an important issue. These were collected by the Japan Radioisotope Association for a fee and sent for disposal. Cost can be reduced by reducing the volume to the maximum possible extent. In addition, since samples that may decompose are not eligible for collection, animals used in experiments are freeze-dried and disposed of in a state where they will not decompose, while reducing their weight as much as possible.
Experimental procedures
Nonclinical procedures were discussed and documented by the parties involved. First, pilot studies should include cell experiments and tumor growth inhibition studies using cancer-carrying animals. These are not subject to GLP testing and can be conducted independently.
We would also evaluate radiation leakage by performing micronucleus formation studies on some cell lines. The GLP experimental details were as follows: a general toxicity test and genotoxicity testing using the micronucleus formation test were performed. Evaluation items for the toxicity tests included general observation, blood sampling, body weight, and organ pathology. In summary, an overview of the development of AB neutron source at the University of Tsukuba and preclinical studies that are being conducted to prepare for clinical trials, were introduced.
Remarks
The initiation of clinical studies will not mark the end of preclinical studies. Various research points and questions can be generated or may be left over during preclinical studies intended to set up particular clinical studies for AB-BNCT systems. To further optimize AB-BNCT, boron drug development, and other applications of NCT in other cancer types, cell-based and animal model-based general preclinical studies are expected to be explored. Further considerations for the use of new biological models using spheroids or other experimental models are expected to be developed for preclinical studies of AB-BNCT systems.
The accelerator type, target reaction, beam axis, beam energy (MeV), beam current, and present status at each institute are shown.
Footnotes
Acknowledgments
We would like to thank Yoshinori Sakurai, Takushi Takata, Hiroki Tanaka, Yuko Kinashi, Minoru Suzuki, Shinichiro Masunaga in KURNS, and Koji Ono from the Kansai BNCT Center; Satoshi Nakamura, Masamichi Ishiai, Hiroshi Igaki, and Jun Itami from the National Cancer Center; Yoshio Imahori, Masaru Nakamura in Cancer Intelligence Care Systems, Inc.; and Hiroaki Kumada, Akira Matsumura, and Hideyuki Sakurai from the University of Tsukuba for their help in completing this study.
Authors' Contributions
N.K. contributed to writing the abstract and introduction, M.M. & S.I. contributed to writing the section “Preclinical studies on vertical downward neutron beam-based AB-BNCT system” and K.N. & Y.M. contributed to writing the section of “Progress of non-clinical trials using a newly developed accelerator neutron source at the University of Tsukuba.”
Disclosure Statement
This work was partly supported by research funds from the Cancer Intelligence Care Systems, Inc., (M.M.). The sponsors had no role in writing this article.
Funding Information
This work was supported in part by the National Cancer Center Research and Development Fund (grant numbers H26-A-18 and H29-A-8) and by research funds from Cancer Intelligence Care Systems, Inc., (M.M.).