
Abstract
The authors review the results of 249 patients treated with boron neutron capture therapy (BNCT) at the Helsinki University Hospital, Helsinki, Finland, from May 1999 to January 2012 with neutrons obtained from a nuclear reactor source (FiR 1) and using
Introduction
Until recently, neutrons needed for boron neutron capture therapy (BNCT) could be obtained only from nuclear reactors. This was a substantial limitation for the method, since nuclear reactors are seldom dedicated for BNCT, are often located in remote areas, and are costly to use and to maintain for medical treatments. In the past, several nuclear reactors were utilized for BNCT treatments of cancer patients worldwide, but most have stopped to function as a BNCT facility. 1 The advent of proton accelerators as the source of neutrons with suitable energy for BNCT have created substantial interest, 2 and the first patients have already been successfully treated with accelerator-based BNCT in Japan since 2012. 1 –5
In this study, the authors review the Helsinki University Hospital (Helsinki, Finland) experience on BNCT. In Helsinki, a nuclear reactor (FiR 1) was used as the neutron source until the closure of the reactor facility for financial reasons in 2012, but now a proton accelerator-based facility located on the university hospital campus is being prepared for the first BNCT treatments. We review, in this study, the clinical results obtained with FiR 1 as the neutron source, describe the new proton accelerator-based treatment and the BNCT suite, and provide the plans for treating cancer patients with accelerator-based BNCT.
A Nuclear Reactor as the Neutron Source
The FiR 1 nuclear reactor
Neutrons for BNCT were obtained from the Finnish Research Reactor (FiR 1). FiR 1 was located at Otaniemi, Espoo, Finland, within the Helsinki metropolitan region and about 6 km from the Helsinki University Hospital. The reactor, a light-water-moderated 250 kW Triga Mark II nuclear reactor, was commissioned in 1962. It first functioned as a research reactor for neutron physics, neutron activation analysis, and isotope production until the mid-1990’s, when an epithermal neutron beam for BNCT was constructed at the reactor. A patient treatment room was made adjacent to the reactor, which required partial cutting of the reactor concrete shielding. The reactor building was renovated to a dedicated clinical BNCT facility that housed besides the treatment room also a neutron irradiation simulation room, a beam monitoring room, and a laboratory for blood boron concentration analyses. 6 Layout of the facility is presented in Figure 1.
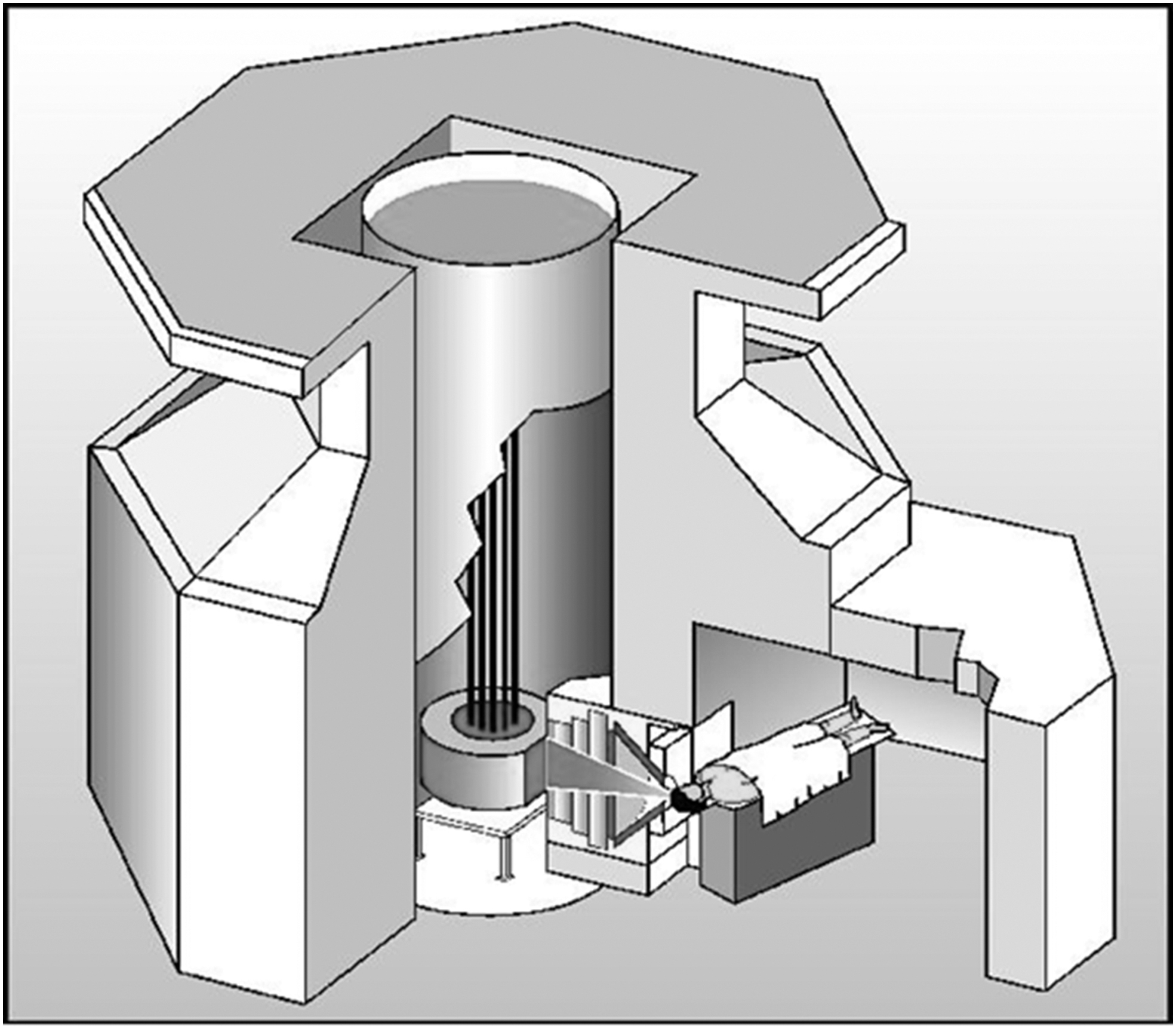
Schematic drawing of the BNCT facility at FiR 1. Courtesy of VTT Technical Research Center of Finland Ltd. BNCT, boron neutron capture therapy.
The FiR 1 neutron beam was moderated using Fluental™, composed of aluminum fluoride (69%), aluminum (30%), and lithium fluoride (1%). The beam epithermal (0.5 eV <E < 10keV) fluence rate was 1.1 × 109 neutrons/cm2/s, and the thermal (E < 0.5 eV) and fast neutron (E > 10 keV) fluence rates were 8.1 × 107 and 3.4 × 107 neutrons/cm2/s, respectively, when measured at the beam exit plane using a 14 cm diameter collimator aperture and the reactor was run at 250 kW power. 7 The fast neutron dose per epithermal fluence was 2 Gy/1013 cm−2 and the γ dose 0.5 Gy/1013 cm−2. The beam circular collimator aperture diameter options were 8, 11, 14, 17, and 20 cm.
Boronophenylalanine
The
Patients
Characteristics of the 249 patients treated with BNCT at FiR 1 from May 1999 to January 2012 and the number of treatments given are provided in Table 1. The administered
Characteristics of 249 Patients Treated with BNCT at FiR 1 from May 1999 to January 2012 and the Number of Treatments Given
The percentages may not add up to 100 due to rounding off.
WHO, World Health Organization.
Procedures
The study protocols of the clinical trials were approved by an Institutional Review Board and the Finnish Medicines Agency before starting any of the trial procedures. The trials were carried out according to Good Clinical Practice and the World Medical Association Declaration of Helsinki. All trial participants provided written informed consent before starting the trial-related procedures.
The trial-related procedures are described in detail in the respective publications. 6,9 –11 In brief, staging examinations usually included physical examination, computed tomography (CT) of the trunk and the tumor site, and contrast-enhanced MRI of the tumor site. Positron emission tomography (PET) using 18 F-fluoro-BPA as the tracer was performed in selected cases before BNCT. The three-dimensional (3D) Monte Carlo (MC) software package SERA (INEEL/MSU, Idaho Falls/Bozeman, ID) was used for BNCT dose planning.
The patients were usually followed up at 4- to 12-week intervals after BNCT. Tumor imaging was usually carried out with CT and/or MRI, which were performed at a few months' intervals during the follow-up. 6,9 –11 Treatment response was evaluated using the RECIST criteria (Response Evaluation Criteria in Solid Tumors criteria), 12 and adverse effects using the National Cancer Institute common terminology criteria. 13
Clinical trials
Four clinical trials evaluating the safety and efficacy of
Clinical Trials Carried Out Using Neutrons from the FiR 1 Nuclear Reactor
Clinical trial registration was not generally available when the trial was carried out.
The main results of the four trials are summarized in Table 2. In general,
Patients treated outside of clinical trials
A slight majority, 141 (56.6%) out of the 249 patients, received BNCT outside of a clinical trial. Most of these patients had either recurrent head and neck cancer (91 [64.5%] out of 141) or malignant glioma progressing after prior radiotherapy (39 [27.7%] out of 141), and the remaining 11 patients had either meningioma (n = 7), melanoma (n = 3), or lymphoma (n = 1). These patients were considered not to have a viable standard therapy option available and were treated with BNCT on a compassionate basis.
Combination and sequential treatments
There is limited data available about treatments that combine BNCT with systemic targeted cancer therapies. We initiated a dose escalation trial (NCT00927147) where cetuximab, a chimeric monoclonal antibody directed to the epidermal growth factor receptor, was administered to patients who had inoperable, locoregionally recurrent squamous cell head and neck cancer after prior conventional radiotherapy. In this trial, intravenous cetuximab was administered after completion of neutron irradiation on the same day as BNCT (day 1). The cetuximab starting dose was 250 mg/m2, infused over 2 h. Using a 3 + 3 dose escalation design, the day 1 cetuximab dose was first escalated to 400 mg/m2, and then up to a maximum cetuximab dose consisting of 400 mg/m2 on day 1 (2-h infusion), 250 mg/m2 on day 7 (1-h infusion), and 250 mg 2 on day 14 (1-h infusion). The planned maximum cetuximab dose level was reached in the trial, but the trial was prematurely discontinued after enrolling 18 patients due to the closure of FiR 1, which led also to loss of the trial sponsor.
Besides cancer treatments administered concomitantly with BNCT, also sequencing of BNCT with other cancer therapies seems feasible. We treated a few patients who had locoregionally recurrent, inoperable head and neck cancer with BNCT followed about 4 weeks later by conventional intensity-modulated radiotherapy plus weekly intravenous cisplatin. The results were considered promising, 14 but remain anecdotal. In conclusion, further research on sequential treatments consisting of BNCT, conventional radiotherapy, and systemic cancer therapy are warranted.
Accelerator-Based BNCT Facility
The BNCT facility
The Helsinki University Hospital and Neutron Therapeutics, Inc., (Danvers, MA) initiated a joint project to install a compact accelerator-based neutron source on the hospital campus in 2016. The international recommendations for a BNCT facility were considered when designing the facility and during its construction. 15,16 The building housing the facility is located next to the hospital cancer clinic and connected to the hospital with a service tunnel, which brings the hospital resources and the infrastructure readily available for patients to be treated with BNCT.
The facility layout is presented in Figure 2. In this two-floor facility, the proton accelerator room and the neutron source, the beam control room, the treatment preparation room, and the treatment room are located on the ground floor, and the boron laboratory and the office rooms on the second floor. 17
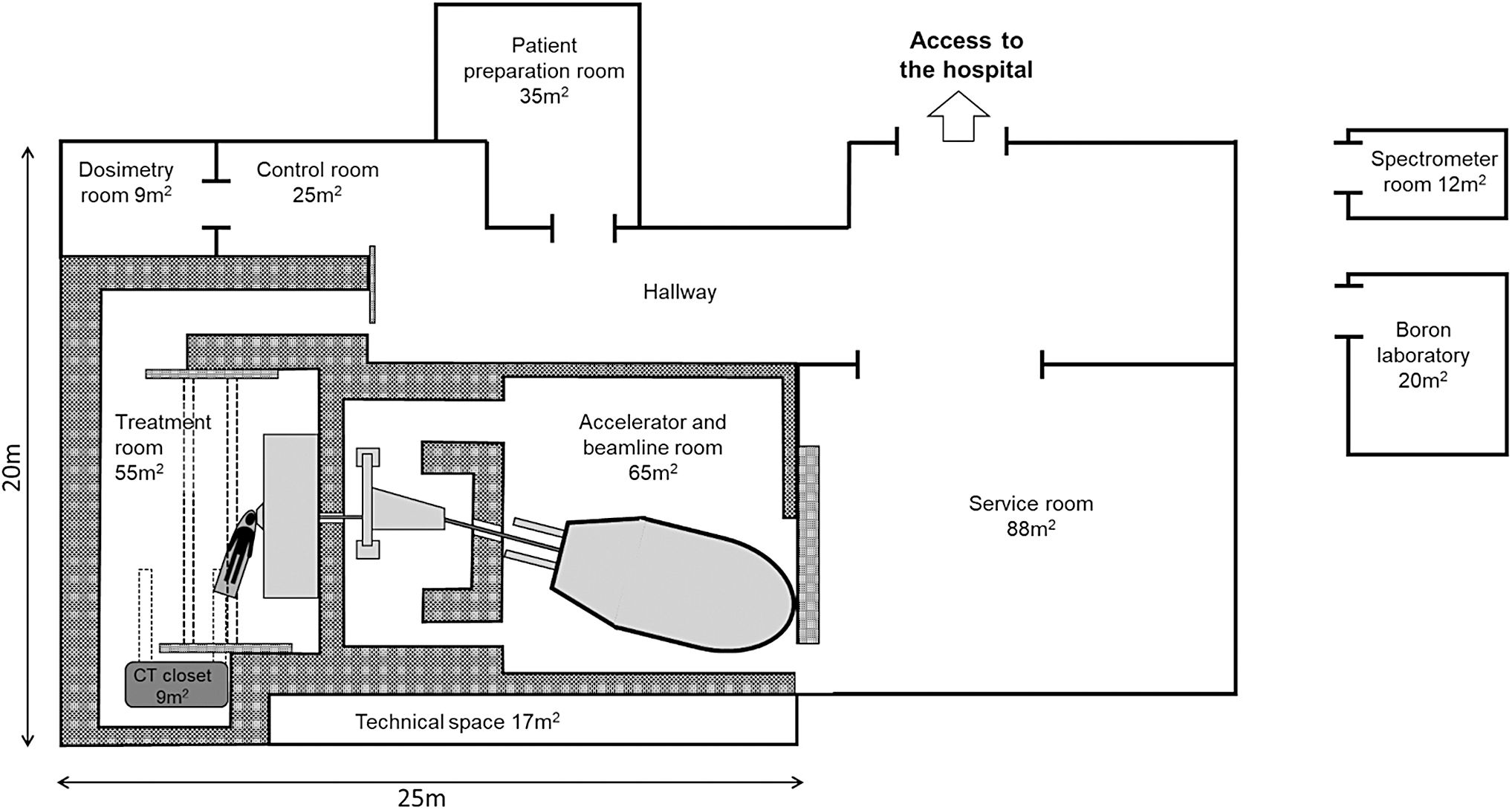
The layout of the BNCT facility equipped with the nuBeam neutron source. The proton accelerator and the neutron source system, and the treatment room are located on the ground floor. The boron laboratory, the spectrometer room, and the office rooms are located on the second floor. BNCT, boron neutron capture therapy.
The treatment room
The patient treatment room shielding is composed of heavy concrete, which is covered with borated or lithiated plastic for neutron absorption. Patient positioning is performed for radiation with a 6-axis robotic image-guided patient positioning system Exacure (BEC GmbH, Reutlingen, Germany). In-room imaging is performed with a rail-mounted Somatom Confidence RT CT scanner (Siemens Healthineers, Erlangen, Germany), located behind neutron shields during neutron irradiations (Fig. 3).

The nuBeam treatment room. The CT scanner (right), the robotic image-guided patient positioning system (middle), and the beam shaping assembly and the beam shutter (left) are shown. Courtesy of Neutron Therapeutics, Inc. CT, computed tomography.
On the treatment day, the patient is positioned onto the robotic couch using an earlier prepared mask and with vacuum pillows. The patient's position is automatically adjusted to match the planning CT and/or MRI images captured before irradiation, and the robotic couch is used to move the patient accurately to the treatment position.
The neutron source
The nuBeam (Neutron Therapeutics, Inc.) neutron source consists of a proton accelerator and a lithium target that converts the proton beam to neutrons. The proton accelerator is a single-ended electrostatic Cockcroft–Walton-type accelerator. The proton beam energy is 2.6 MeV, and the beam is designed to operate with a proton current of 30 mA. Neutrons are produced inside an optimized Beam Shaping Assembly (BSA), located in the treatment room. Within the BSA, the proton beam is directed to a cooled, rotating, solid lithium target, where a low-energy neutron beam is generated from the p-Li reaction and the subsequent passage through an optimized neutron moderator. 18
The neutron beam was designed to meet the recommendations of the International Atomic Energy Agency (IAEA) TECDOC 1223 document, 15 and to have a roughly similar beam spectrum to the one used at the FiR 1 reactor. The neutron beam is monitored with two neutron monitors and one γ monitor located close to the beam exit port. The beam circular delimiters, produced from enriched 6 Li polyethylene, have the same aperture diameter options as were available at the FiR 1 reactor facility (8, 11, 14, 17, and 20 cm).
Dosimetry
The BNCT facility uses a neutron activation analysis method for thermal and epithermal neutron flux dosimetry and a paired ionization chamber method for neutron and γ radiation measurements. 19 The measurements are performed in air within a cylindric polymethylmethacrylate (PMMA) phantom of 20 cm diameter and 24 cm in length, and in a large water phantom (MP3-PL Hi-Tech 3D water phantom solution for particle therapy treatment machines; PTW, Freiburg, Germany). In addition, end-to-end testing is performed in a small cubic 20-cm-wide water phantom to enable image-guided phantom positioning, and 3D measurements of the dose and the neutron flux distributions.
Neutron activation analysis, based on the conversion of stable isotopes to radioactive isotopes upon irradiation with neutrons, is a well-known and widely used method for measuring the neutron fluence. The method is advantageous when measuring mixed neutron plus γ irradiation, since activation foils or wires are not sensitive to γ radiation, and activation of the elements is directly related with the neutron fluence within a certain energy range. 16 The daily quality assurance is performed in a PMMA phantom using diluted Al-Au and Al-Mn activation foils (1% wt Au or Mn, respectively), with a diameter of 12 mm and thickness of 0.2 mm (Goodfellow Cambridge Ltd., Huntingdon, United Kingdom). The beam profile is measured with a set of activation wires (Al-Mn; Mn 2.6% wt), length 10 mm, and diameter 0.76 mm (Goodfellow Cambridge Ltd.).
Neutron beam characterization is performed with a stack of activation foils that consist of various materials, with or without a cadmium cover that eliminates low-energy neutrons from the beam. 16 Activity of the foils or wires is measured with a high-purity γ spectrometer (GEM Coaxial P-type PopTop HPGe γ-Ray Detector; ORTEC, Zoetermeer, the Netherlands) with an integrated Cryo-cooling System, an MCA DSPEC-50 multichannel analyzer, and the LVis analysis software. The γ energy range is set from 40 to 2000 keV.
The paired ionization chamber method is used for estimating the neutron and γ ray doses absorbed to a reference tissue. 19 At the facility, a methane-based tissue-equivalent gas-filled A-150 plastic-walled Exradin T2 chamber (Standard Imaging, Inc., Middleton, WI) is paired with an extra-pure argon-filled magnesium-walled Exradin M2 chamber (Standard Imaging, Inc.), and a portable, single channel, high-precision reference class electrometer DOSE-1 (IBA, Louvain-la-Neuve, Belgium) is used to measure the absorbed dose.
The metallic parts of the large water phantom tend to activate in the neutron beam, including the screws in the thin entrance window, the metallic scanning rails, and the support of the scanning detector. The activation source is mainly 56Mn that has a short half-life (2.6 h), but a small amount of 51Cr was also detected in the metal parts (half-life, 27.7 d). To minimize the activation, special supports were printed using polylactic acid (PLA) and a Ultimaker 2 + 3D-printer (Ultimaker BV, Zaltbommel, Netherlands) that increases the distance between the scanning rail and the ionization chamber or the activation detectors. In addition, ionization chambers contain a small amount of copper that activates to 64Cu (half-life, 12.7 h).
Blood boron analysis
Since direct methods to measure tumor 10 B content during neutron irradiation are not generally available for clinical use, 20 tumor boron concentration is usually estimated using the blood boron concentration and tissue-to-blood boron ratios derived from boron biodistribution studies. 21 We plan to estimate tissue boron concentrations also with PET using fluorine-18-labeled BPA-F as the tracer ( 18 F-BPA-F). 22
The whole blood boron concentration is measured with ICP-OES 8,23 using an Agilent 5100 ICP-OES instrument (Agilent Technologies, Inc., Santa Clara, CA) equipped with a Meinhard-type nebulizer and a double-pass glass cyclonic spray chamber. Quantification of boron is optimized with the instrument software, setting the radiofrequency generator power at 1300 W, the nebulizer gas flow rate 0.70 L/min, the auxiliary gas flow rate 1.0 L/min, and the plasma gas flow rate 12 L/min. The background is negligible close to the selected boron emission lines (analytical line, 249.772 nm; control line 249.667 nm), where the iron signal intensity is <0.1% that of boron when the concentrations are equal. Four calibration solutions (0, 1, 2, and 5 μg/mL) are prepared by mixing the boron stock, the beryllium stock, Triton X-100 (0.1%), and fresh blood from a patient, and a 4-point calibration curve is applied for all measurements using these solutions.
For blood boron content analysis, a blood sample of ∼0.5 g is collected and added to 4.5 g of a solution containing 1 mg/kg beryllium (detected at wavelength 313.042 nm), and 0.1% Triton X-100, and after vigorous shaking, the solution is filtered with a syringe filter (5.0 μm) before the boron content measurement with ICP-OES. Each sample is analyzed as a duplicate.
Treatment planning
Treatment planning is based on full MC simulation with a patient model deduced from Dicom (CT, MRI, and PET images). The dose engine for patient dose calculation was developed by Neutron Therapeutics, Inc., on top of the GEANT4 MC toolkit. 24 The dose engine is operated through the RayStation treatment planning system (RaySearch Laboratories AB, Stockholm, Sweden) that is used to define the patient geometric model and the target volumes, organs at risk, and their tissue compositions. 25 In addition, RayStation is used for reporting of the doses delivered. The dose engine also provides activation reaction rates for Mn and Au at user selected points in the treatment plan, thus enabling comparison of Mn and Au foil activation calculated by the dose engine and the actual dosimetry measurements with activation detectors, and, therefore, estimation of dose uncertainty in the treatment plans.
Radiation safety and residual radioactivity
Despite careful selection of the treatment room materials, the neutron beam might cause activation of the materials resulting in residual radioactivity. Residual activity depends on the neutron fluence, the activation cross-sections of the target nuclei, and the decay rate of the activated products. To minimize residual activity and unnecessary radiation exposure, the treatment room interior walls, the doors, the ceiling, and the floor are coated with lithiated plastic covers that efficiently slow down and absorb neutrons without producing long-lived activated nuclei. The treatment room walls are built of heavy concrete to absorb secondary γ radiation, and the room ventilation is designed to remove activated products ( 3 H, 40Ar) from the air.
Inside the treatment room, a red signal light indicates radiation output from the neutron source. A continuous-action γ dose rate monitor is installed in a corner of the treatment room to allow measurement of the residual radiation. A red light outside of the treatment room shows when the radiation is on or when the residual dose rate inside the treatment room is too high for the personnel safe entry into the room. Under normal circumstances, the personnel can enter the treatment room almost immediately after shutting down the neutron beam, because a lead beam shutter can be driven in front of the beam aperture, the major source for residual activity in the treatment room.
Regular measurements of the background radiation level at the facility are made with a Camberra InSpector™ 1000 Digital Hand-Held Multichannel Analyzer (Mirion Technologies, Inc., Atlanta) capable for identifying activated elements. Residual long-term activation was studied at various facility locations during the accelerator maintenance period after a few hundred hours of neutron irradiation. No significant increase in the background radiation activity was detected.
From a radiation safety perspective, the accelerator room and the treatment room are classified as controlled areas. The treatment room is equipped with a last-man-out switch to ensure that only the patient remains inside the treatment room during irradiation. The control room and the patient preparation room are classified as supervised areas. The personnel working at the facility are considered as Class A radiation workers.
Commissioning of the facility
Before starting the facility construction, a preliminary approval was applied from the Finnish Radiation Safety Agency (STUK) for the construction, and a new license was applied before starting neutron production to prepare the facility for commissioning. Commissioning started in 2019 when the first neutrons were produced, and with the first tasks to characterize the neutron beam properties and to develop protocols for dosimetric measurements and quality assurance. The second part of the commissioning process includes comprehensive verification and validation testing of the system focusing on preparations for clinical studies. The BNCT facility verification and validation protocols were planned in accordance with international recommendations for neutron capture therapy, and for external radiotherapy where applicable. These recommendations include the IAEA TECDOC-1223 document, 15 the NRG report 21425/03.55339/C 16 , and the International Electro-technical Commission (IEC) standard 60601-2-64 and 62667. 26,27
The facility testing aims at patient safety, and verification and validation of the neutron beam delivery and dosimetry protocols, the treatment planning, the patient imaging and positioning system, and the treatment workflow. After commissioning, the STUK will review the facility before treating patients.
Preclinical Models, and Planned Treatments with Accelerator-Based BNCT
Preclinical models
Approval of novel boron carrier compounds that have high uptake in tumors compared with healthy tissues is of paramount importance for the future development of BNCT. The currently used agents,
Planned clinical trials
The first patients treated with accelerator-based BNCT are planned to be treated within the context of a clinical trial, called the Safety Trial. The Safety Trial will largely replicate the Phase I/II trial carried out at the FiR 1 nuclear facility as the neutron source, 9,10 except that the neutrons are generated using an accelerator instead of a nuclear reactor. The Safety Trial study protocol has been approved by a Helsinki University Hospital Institutional Review Board.
The patient population of the Safety Trial will consist of patients with locally recurrent or persistent head and neck carcinoma after conventional radiotherapy or chemoradiotherapy. The tumor needs to be considered inoperable by head and neck surgeons and with no distant metastases detected in the staging examinations. The primary endpoint is the objective response rate to
Once the safety of
The hospital research strategy includes collaboration with other BNCT centers in carrying out nonrandomized and randomized multicenter trials. In the European Union (EU), authorization is needed for manufacturing and import of investigational medicinal products (IMPs) with a few exceptions.
29
One exception is preparation of individually prescribed IMP doses in hospital if the hospital has a GMP authorization to prepare pharmaceuticals and the pharmaceutical will be used in the hospital setting in the same EU member state. This exception may allow multicenter trials to be conducted within the EU using
Patient treatments outside of clinical trials
As in the previous trials at the FiR 1 nuclear reactor, it is the intention to treat selected individual cancer patients with accelerator-based BNCT outside of clinical trials when proven medical interventions either do not exist or are considered ineffective. Such BNCT treatments will be based on informed consent following the principles of the World Medical Association Declaration of Helsinki.
Conclusions
The efficacy results obtained with
Footnotes
Disclosure Statement
H. Koivunoro is employed by Neutron Therapeutics Inc. H. Joensuu is the Chairman of the Scientific Advisory Board of Neutron Therapeutics, Inc., the Chairman of the Scientific Advisory Board of Orion Corporation, Orion Pharma, and the Chairman of the Scientific Committee of Maud Kuistila Foundation; he has received a honorarium for speaking from Deciphera Pharmaceuticals, has been full time or part time employer or consultant of Orion Pharma, and owns stocks of Orion Pharma and Sartar Therapeutics. No further potential conflict of interest was reported by the authors.
Funding Information
This work was supported by the Comprehensive Cancer Center of the Helsinki University Hospital, Finland.