
Abstract
Purpose:
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic hepatic disease worldwide, with functional impairment of the mitochondria occurring from early stages. Technetium-99m methoxy-isobutyl-isonitrile (99mTc-MIBI) is a lipophilic agent trapped in the mitochondria. This study aims to evaluate the utility of 99mTc-MIBI heart/liver uptake ratio in screening for NAFLD during myocardial perfusion imaging (MPI).
Methods:
Seventy eligible patients underwent a 2-d rest/stress 99mTc-MIBI scan with a 2-min planar image acquired in rest phase, at 30, 60, and 120 min postradiotracer administration. Heart/liver uptake ratio was calculated by placing identical regions of interest on the heart and liver dome. All patients underwent liver ultrasound and were allocated into groups A, having NAFLD; and B, healthy individuals without NAFLD.
Results:
Mean count per pixel heart/liver ratios gradually increased over time in either group; nonetheless the values were significantly higher in group A, regardless of acquisition timing; with the p-value equal to 0.007, 0.014, and 0.010 at 30, 60, and 120 min, respectively.
Conclusion:
Determining 99mTc-MIBI heart/liver uptake ratio during rest phase in patients undergoing MPI may be a useful, noninvasive screening method for NAFLD; with no additional cost, radiation burden, or adverse effects in these patients. Trial registration number:
Introduction
Nonalcoholic fatty liver disease (NAFLD) is significantly correlated with metabolic syndrome and has become a global “pandemic” with increasing prevalence, affecting about 24.1% of the population. This umbrella term covers a wide spectrum of conditions, from simple hepatic steatosis to nonalcoholic steatohepatitis (NASH), ultimately leading to cirrhosis and hepatocellular carcinoma (HCC) in most severe cases. 1,2 NAFLD is associated with atherogenic dyslipidemia and an increased cardiovascular risk 3 with cardiovascular disease being the leading cause of death in these patients. 4
While liver biopsy remains the gold standard method of diagnosis, there is growing interest in implementing noninvasive diagnostic modalities, such as liver ultrasound, recommended as the first-line screening modality, and magnetic resonance spectroscopy (MRS). 5 Despite all, NAFLD remains an underdiagnosed condition and is generally underappreciated by primary health care physicians. 6 Myocardial perfusion imaging (MPI) with Technetium-99m methoxy-isobutyl-isonitrile (99mTc-MIBI) is a mainstay modality in diagnosis and management of coronary artery disease (CAD), as a noninvasive, accessible, cost-effective modality with relatively low radiation burden.
The 99mTc-MIBI is a lipophilic cationic agent predominantly retained in the mitochondria due to its significantly negative transmembrane potential. Therefore, it is also implemented in assessing the metabolic impairment and oxidative stress in various other mitochondrial diseases and neurodegenerative disorders. 7,8 Structural and molecular alterations of mitochondria, which are responsible for fatty acid oxidation, have a pivotal role in the pathogenesis of NAFLD. Mitochondrial function impairment occurs from the early stages of hepatic steatosis, gradually leading to oxidative stress and inflammation, eventually resulting in apoptosis of hepatocytes and fibrotic changes. 9,10
Considering the independent risk NAFLD poses for CAD as well as the significant correlation both have with metabolic syndrome, 3,4 NAFLD is likely more prevalent in candidates for MPI scan. This study aims to evaluate the potential role of determining the relative hepatic uptake of 99mTc-MIBI during rest phase MPI in screening NAFLD in patients referred for ruling out myocardial ischemia, thereby facilitating its early diagnosis, in-time treatment, and prevention of related cirrhosis and HCC.
Materials and Methods
Patient selection and allocation
This study was approved by the Clinical Research Ethics Committee of the Medical School of Shahid Beheshti Medical University (
This prospective, single-center study compromised 70 eligible patients who were referred for 99mTc-MIBI MPI to rule out myocardial ischemia during a period of 6 months. Patients with any documented cardiac disease, patients with high pretest probability of ischemic heart disease (IHD), patients with history of diabetes mellitus, regular alcohol consumption (>20 g per day), benign or malignant hepatic neoplasm, any kind of viral, metabolic, or autoimmune liver disease, as well as patients taking any hepatic steatosis-inducing medications (such as corticosteroids, Methotrexate, Tamoxifen, and insulin), were not included in the study. One hundred ninety-seven patients with low to intermediate/intermediate pretest probability of IHD, who were referred for MPI to rule out myocardial ischemia, underwent a 2-d rest/stress 99mTc-MIBI gated single-photon emission computed tomography (SPECT), from whom 127 patients with abnormal myocardial perfusion or significant soft tissue attenuation effects, defined as summed stress score (SSS) or summed rest score (SRS) >2, were excluded from the study. Acquisition details will be discussed in the following section.
The remaining 70 participants had their body mass index (BMI = Height/Weight 2 ) documented and underwent peripheral venous blood sampling after a 9-h fasting to check their biochemical profile and liver function tests (LFT), also including fasting blood sugar (FBS), triglyceride (TG), total cholesterol, aspartate aminotransferase (AST), alanine aminotransferase (ALT), albumin (Alb), and prothrombin time (PT). All patients underwent liver ultrasound examination, according to which were allocated into group A, patients with any degree of fatty liver disease; and group B, patients with normal results having no evidence of fatty liver disease.
Acquisition protocols and image processing
All patients underwent a 2-d rest/stress 99mTc-MIBI gated SPECT MPI, according to the European Association of Nuclear Medicine guidelines for MPI scan. 7 All 99mTc-MIBI Kits underwent thin-layer chromatography and radiochemical purity >95% was deemed acceptable for utilization. Following IV injection of 555 MBq 99mTc-sestamibi, a 2-min planar image of the thoracoabdominal region was acquired at 30, 60, and 120 min, in anterior view, with the patient lying supine. The standard rest SPECT was acquired, as per usual, at 60 min postinjection. On the day after, myocardial stress was achieved by exercise (Bruce protocol) or Dipyridamole injection (0.14 mg/kg/min over 4 min), with 740 MBq 99mTc-sestamibi injected at peak stress and acquisition performed as per routine. As the amount, type, and timing of fatty meal ingestion affect the hepatic clearance of 99mTc-MIBI, the authors had all patients drink 120 cc of whole milk of the same brand 10 min after radiotracer injection.
Images were acquired with a variable angle dual-head Evo-Voxel Siemens γ-camera with low-energy high-resolution collimator, 140 Kev photopeak setting, symmetrical width energy window of 10%, matrix 64 * 64, and zoom of 1.46, including the rest planar image (2 min duration, anterior view) and standard SPECT images (64 projections; 25 s/projection, 8-frame gated study, noncircular orbit). Images were processed by a nuclear medicine physician, blinded to patient allocations, using quantitative perfusion SPECT (QPS) (Fig. 1), and quantitative gated SPECT (QGS) software (Cedars-Sinai Medical Center Cardiac Suite), without correction of scattering or attenuation. As described above, patients with abnormal myocardial perfusion or significant soft tissue attenuation effects, defined as SSS or SRS >2, were excluded from the study.
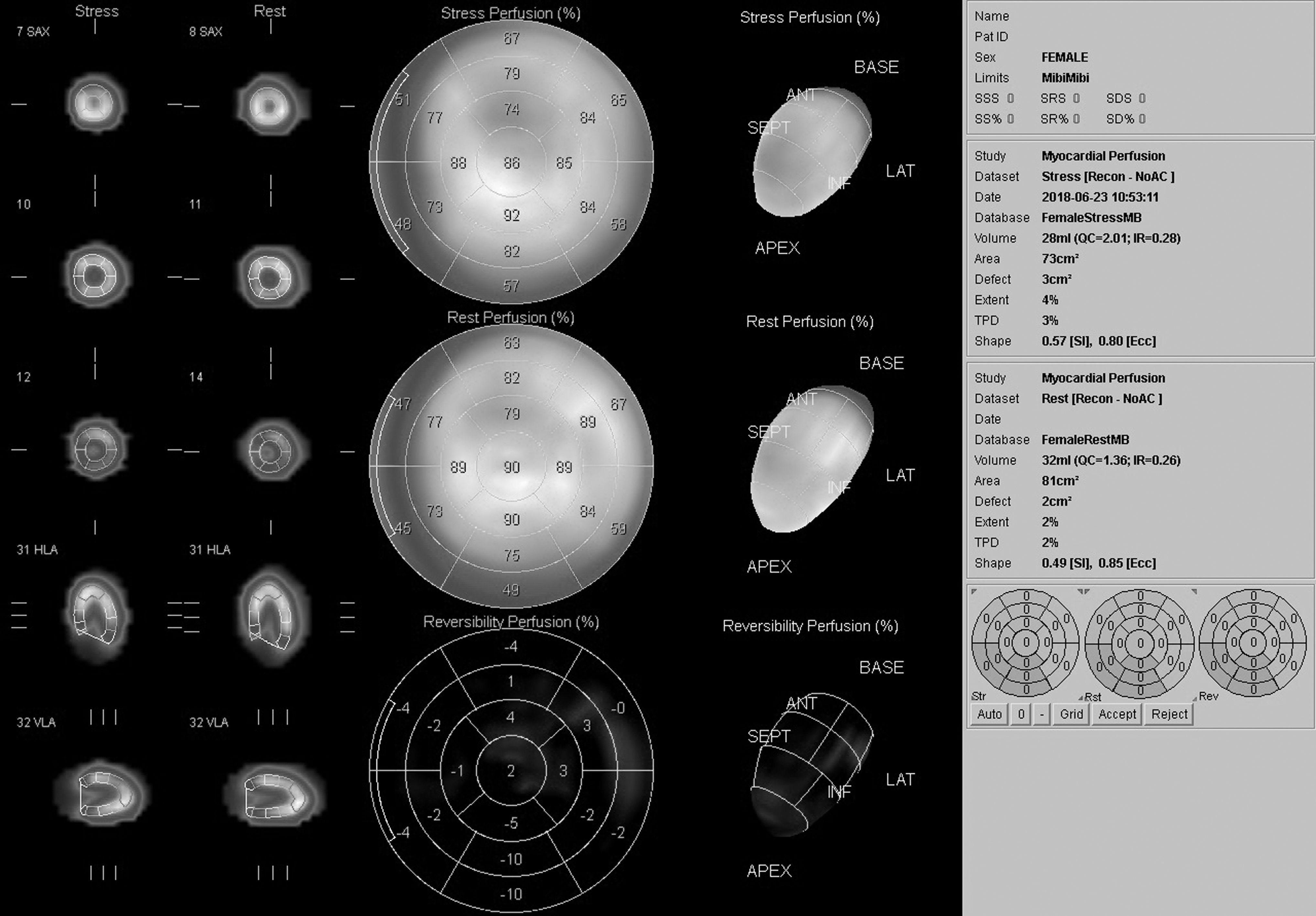
QPS (Cedars-Sinai Medical Center Cardiac Suite) enables automated quantification of perfusion defects during myocardial perfusion imaging. It divides the left ventricle into 17 standard segments and compares the registered counts in each segment with a normal population database. Scores are applied to each segment based on severity of the perfusion defect; 0, 1, 2, 3, and 4 indicate no defect, mild, moderate, severe defects, and absence of perfusion, respectively. The summed stress/rest score, sum scores of all segments, is used in assessing global left ventricle ischemia. Summed scores <4 are usually nonsignificant, often produced by soft tissue attenuation effects of breasts or the diaphragm. Patients with a summed stress or rest score of >2 were excluded from this study. QPS, quantitative perfusion single-photon emission computed tomography.
Hand-drawn regions of interest (ROI) were set on each planar rest image (three images per person at 30, 60, and 120 min), with identical size and shape ROIs placed on the upper segments of right liver lobe as well as anterolateral wall of the left ventricle, to minimize the interfering effects (such as scatter) of these adjacent organs (Fig. 2). The mean count per pixel values was obtained and the heart to liver ratios calculated, which considering that they had excluded patients with any cardiac disease or abnormal MPI results, would be an indicator of relative hepatic uptake.
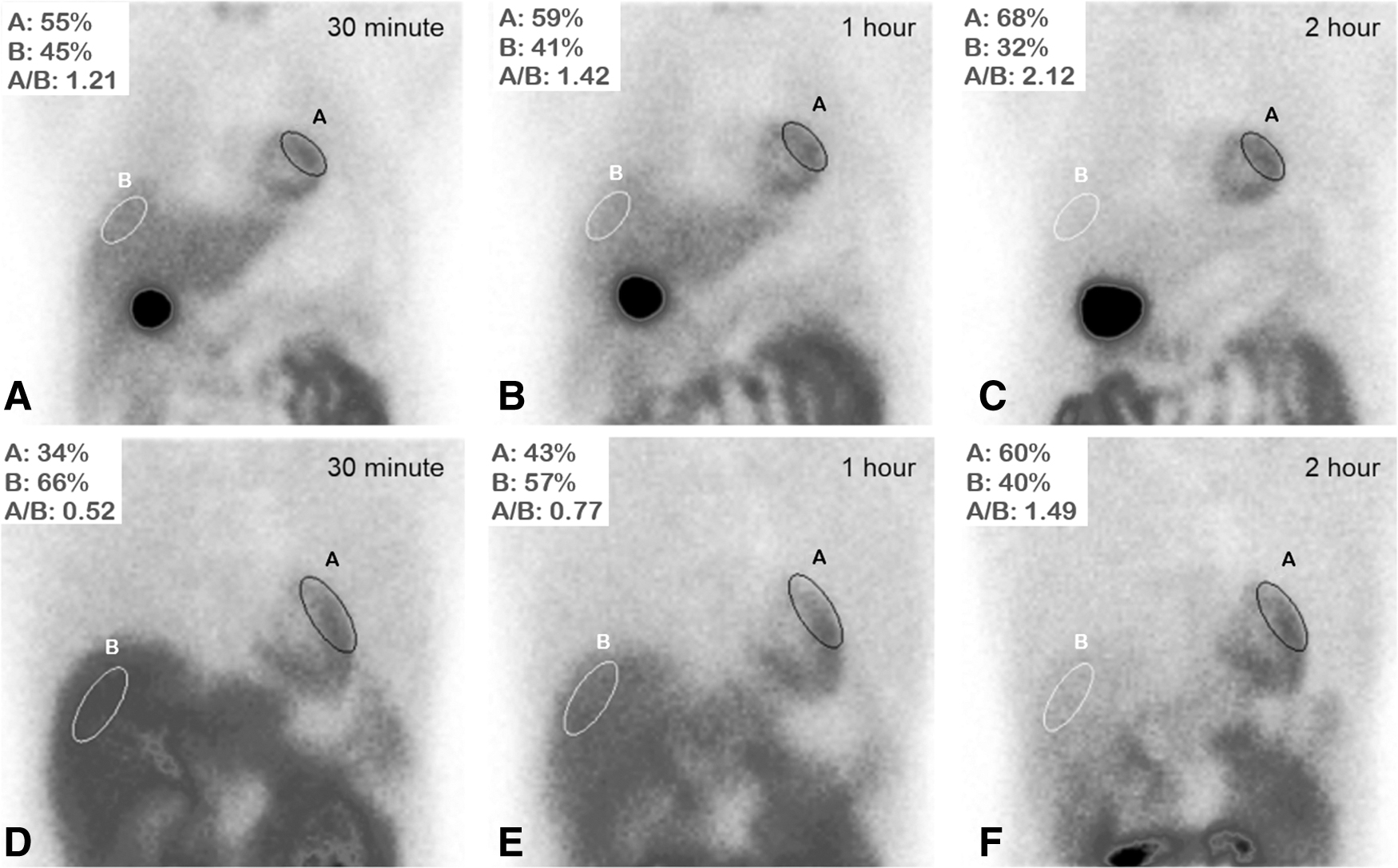
Two-min planar images of the thoracoabdominal region were acquired after IV administration of 555 MBq 99mTc-MIBI at 30, 60, and 120 min, in anterior view. Identical size and shape region of interests were placed on the upper segments of right liver lobe as well as anterolateral wall of the left ventricle. ROI uptakes were calculated based on mean count per pixel values. The percentiles attributed to A (the heart) and B (the liver) represent the uptake of each ROI relative to the summed uptake of both ROIs. A/B = Heart/Liver uptake ratio. Acquisitions
Statistical analysis
Quantitative and categorical or qualitative data were represented by the mean, standard deviation (SD), and numbers/percentages, respectively. They used the Kolmogorov–Smirnov test for the assessment of the normality of distribution. Mann–Whitney U-test was utilized to determine the statistical differences between two groups of normal and NAFLD patients. p-Value <0.05 was considered significant. Random forest classifier with five-fold cross-validation was used to develop a model based on clinical and scintigraphy findings to predict NAFLD, by implementing three different strategies (Scheme:
Results
Seventy patients, consisting of 24 males (34.3%) and 46 females (65.7%), with the mean age of 51.0 ± 9.0 years were categorized into groups A, having evidence of fatty liver disease (n = 30); and B, with normal liver (n = 40). The demographic, clinical, and laboratory characteristics of the participants are presented in Table 1. Age, gender, and LFT results (including AST, ALT, serum Alb, and PT) had no statistically significant difference among the groups (p-value >0.05). As expected, BMI, TG, and total cholesterol levels were significantly higher in group A (p-value = 0.000).
Baseline Characteristics of All Patients (n = 70)
Bolded numbers: Values with statistically significant difference (P-value ≤ 0.05) among the groups.
BMI, body mass index; FBS, fasting blood sugar; TG, triglyceride; AST, aspartate aminotransferase; ALT alanine aminotransferase; Alb, albumin; PT, prothrombin time.
Regarding the intrahepatic 99mTc-MIBI uptake, the mean count per pixel heart/liver ratios gradually increased over time in either group; nonetheless, the values were significantly higher in group A, regardless of acquisition timing with the p-value equal to 0.007, 0.014, and 0.010 at 30, 60, and 120 min, respectively (Table 2).
Heart/Liver Uptake Ratio in Two Groups of Patients at Three Time Points
As for random forest classifier results (Table 3), the first strategy implemented all available paraclinical, demographic (age, sex, BMI), and scintigraphy (0.5, 1, and 2 h) data (true positive rate = 0.87, false positive rate = 0.15, precision = 0.88, AUROC = 0.95). The second strategy compromised lipid profile (TG, cholesterol), FBS, demographic (age, sex, BMI), and scintigraphy (0.5, 1, and 2 h) data and demonstrated similar accuracy to the first strategy without including AST, ALT, Alb, and PT (true positive rate = 0.86, false positive rate = 0.17, precision = 0.86, AUROC = 0.95). The third strategy only accounted for demographic (age, sex, BMI) and scintigraphy (0.5, 1, and 2 h) data to predict NAFLD (true positive rate = 0.76, false positive rate = 0.27, precision = 0.76, AUROC = 0.84). Repeating the third strategy by including single time point scintigraphy data at 1 h resulted in AUROC of 0.85, comparable to the accuracy of multiple time point measurements. Heart/liver uptake ratios higher than the threshold of 1.0, at 1 h postradiotracer injection, warrant further evaluation for potential NAFLD (Fig. 3).
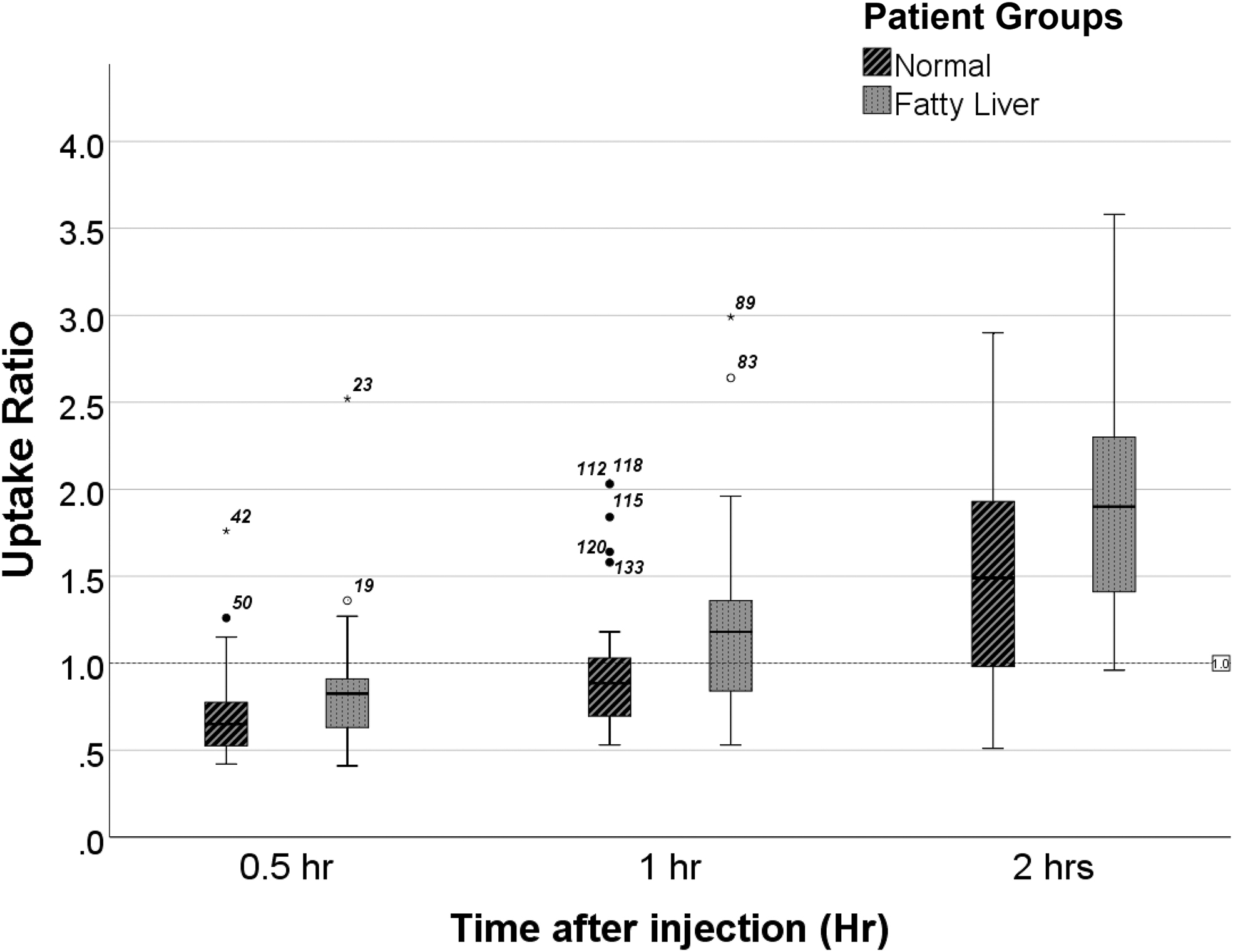
Comparison of the heart/liver uptake ratio in two groups of patients at three time points.
Random Forest Classifier Results Comparing the Accuracy of Different Models in Predicting Nonalcoholic Fatty Liver Disease
The star (*) marks the values which have been accounted for/included in each random forest classifier strategy.
S, strategy; Chol, cholesterol; H/L, heart/liver; TP, true positive; FP, false positive; Precis, precision; AUROC, area under receiver operating characteristic curve.
Discussion
NAFLD is the leading cause of chronic liver disease worldwide with its growing prevalence paralleling increasing cases of metabolic syndrome. While early stages of hepatic steatosis are rather benign, it may progress to NASH, cirrhosis, and eventually HCC. 1 –6 Most cases will not develop high-grade NASH and cirrhosis; however, given its high prevalence, even small percentages translate to significant numbers. Pharmacologic treatment of NAFLD, specifically NASH-related fibrosis, is under extensive research; nonetheless, risk factor modification in early stages and preventing further progression remains the most appropriate measure. Therefore, developing noninvasive, accessible, simple methods of screening and diagnosis is of utmost importance. Liver biopsy remains the gold standard of diagnosis, unsuitable for screening due its invasive nature, potential complications, and cost. Serum biomarkers have proven to significantly underestimate the presence of NAFLD. The most commonly implemented radiological methods are ultrasound and MRS; however, the cost-effectiveness of screening the general population by them is still under debate. 11
Our study indicates that rest phase heart/liver uptake ratio of 99mTc-MIBI is significantly higher in patients with NAFLD, proposing it as a simple screening method in patients already undergoing MPI to rule out myocardial ischemia, who are at a higher risk for NAFLD as well, with no additional cost, radiation burden, or complication.
As expected, we observed a gradual rise in heart/liver ratios in either group. Decay-corrected data revealed consistent myocardial uptake values while liver uptakes gradually decreased overtime, which is explained by the physiologic clearance of 99mTc-MIBI from the liver. 12 NAFLD patients demonstrated significantly higher heart/liver ratios regardless of measuring time, including at 1 h postinjection, which is the usual time point when rest phase acquisition is performed.
Our findings are in concordance with findings of Masuda et al, who evaluated 26 patients with biopsy-proven NAFLD by performing laboratory tests and a 99mTc-MIBI liver scintigraphy. They acquired a 2-min planar image of thoracoabdominal region in anterior view 10 min after bolus injection of 600 MBq 99mTc-MIBI in rest phase. Mean count per pixel liver/heart ratios were calculated by defining ROIs in the right upper lobe of liver and the heart. They categorized the patients into non-NASH/simple hepatic steatosis (n = 4), borderline NASH (n = 11), and NASH (n = 11) and reported that the relative hepatic uptake was significantly lower in NASH and borderline NASH compared with both the non-NASH group and the healthy population (based on existing literature).
They observed a significant correlation between the liver/heart ratio and degree of NASH. 13 Aside from the small number of patients and not having a control group with the same exclusion criteria, a prominent limitation of this study is that the effect of reduced cardiac uptake in CAD and other cardiomyopathies is not accounted for, as stress-phase MPI scan was not performed. 13,14 The 99mTc-MIBI uptake portrays the mitochondrial function of cells 8 and NAFLD has been established as a disease of the mitochondria, with functional alterations of the mitochondria present even at early stages of hepatic steatosis. These functional alterations lead to gradual impairment of fatty acid oxidation, resulting in oxidative stress and in turn leading to inflammation (NASH), hepatocyte apoptosis, and fibrosis in advanced stages, 9,10 justifying the observed decreased hepatic uptake of 99mTc-MIBI in NAFLD patients compared with healthy individuals and possibly a correlation between relative uptake ratio and disease severity.
We developed a model to predict NAFLD based on patient's demographic, laboratory, and scintigraphy (at 0.5, 1, and 2 h) data. The model's strength while excluding laboratory data, which may not be always available, decreases to 0.84 AUROC, which is still sufficient enough for a screening tool. Employing single time point scintigraphy measurement results at 1 h post-tracer injection, the time rest-phase MPI acquisitions usually take place, yields a comparable accuracy (AUROC = 0.85), alleviating the need for multiple acquisitions, with heart/liver uptake ratios higher than the threshold of 1.0 warranting evaluation for potential NAFLD (Fig. 3). Naturally, implementing the model in larger populations with result in a more accurate threshold. Several studies have focused on evaluation and comparison of the diagnostic performance of noninvasive methods for screening NAFLD. Bril et al, evaluated the accuracy of liver ultrasound for the diagnosis of NAFLD in overweight and obese patients.
They found the performance of US (parenchymal echo alone) rather modest, and significantly worse than MRS (AUROC: 0.82 [0.69–0.94] vs. 0.96 [0.90–1.00]; p = 0.04). Implementing echography parameters improved the AUROC (0.89 [0.83–0.96]). 15 Another study assessed the accuracy of hepatic ultrasound score, based on hepatic attenuation and the anteroposterior diameter of the right hepatic lobe, in predicting NAFLD. Its best performance (cutoff point ≥1 point) had AUROC of 0.85. 16 The results were less favorable in children, at optimum screening cut points aiming for a specificity ≥80%, US had only mediocre performance with AUROC of 0.70. 17 Fatty liver index (FLI), NAFLD liver fat score (NAFLD-LFS), hepatic steatosis index (HSI), visceral adiposity index (VAI), triglyceride × glucose (TyG) index, and Zhejiang University (ZJU) index are noninvasive and nonimaging indexes, based on a complex list of laboratory data, employed to predict NAFLD. 18,19
The AUROCs of FLI, LFS, HSI, VAI, and TyG for predicting hepatic steatosis has been determined 0.83, 0.80, 0.81, 0.92, and 0.9, respectively. However, they had relatively poor performance in distinguishing moderate and severe steatosis, with fibrosis and inflammation identified as significant confounding factors. 18 Another study evaluated HSI, ZJU index, and FLI for predicting NAFLD, with their AUROC determined 0.874, 0.886, and 0.884, respectively. 19 Considering all these data, the accuracy of our scintigraphy-based model for predicting NAFLD (AUROC of 0.85) is acceptable and comparable to other commonly used US and laboratory-based indexes. This method is not intended to compete with liver ultrasound as a first-line screening modality, but may be a useful method in screening NAFLD in patients already undergoing MPI to rule out myocardial ischemia. As a secondary finding of MPI in this setting, it has the prominent advantage of having no additional cost, radiation burden, or side effect.
Our study demonstrated no significant difference in age, gender distribution, AST, ALT, serum Alb, and PT levels among the groups; whereas BMI, TG, and total cholesterol levels were expectedly higher in NAFLD patients. These findings are in line with existing literature as LFTs are proven to be neither sensitive nor specific in screening for NAFLD and are normal in about 50% of NAFLD patients. 20,21 On the other hand, hyperlipidemia is reported to be significantly associated with NAFLD. Nakahara et al, reported hyper-LDL cholesterolemia and hypo-HDL cholesterolemia in 37.5% and 19.5% of biopsy-proven NAFLD patients 22 and another study has determined TG as the strongest predictor of NAFLD among other parameters. 23
Study limitations
This study has some limitations that should be considered. While liver ultrasound is currently recommended as the first-line screening method for NAFLD; liver biopsy remains the gold standard of diagnosis, despite being rarely performed for this sole purpose. Regarding its invasive nature, possible complications and significant cost, acquiring pathological correlation for all included patients in this study was not feasible, nor ethical. The relatively small number of patients as well as limited accuracy of ultrasound did not allow us to further categorize NAFLD patient-based grade of disease. To prevent the interfering effect of microvascular disease, possibly reducing hepatic uptake and/or rest phase myocardial activity, diabetic patients were excluded from the study. They could not perform CT scan-based attenuation correction, which may have affected the results as the BMI was significantly different among the two groups.
Also, the type, amount, and timing of fatty meal ingestion after MIBI injection, protein binding, and lipophilicity of the radiotracer complex may affect the hepatic clearance and plasma concentration of MIBI, thereby affect the heart/liver uptake ratios. Therefore, in addition to maintaining a uniform patient preparation, each center should analyze their own patient data and determine cutoffs based on the standard protocols of their department. To ensure better signal-to-noise ratios, the relative hepatic uptake was calculated on an additional 2-min planar acquisition. Future studies are required to assess the feasibility of using routine SPECT projections, preferably using hybrid SPECT/CT scanners with accurate attenuation correction, omitting the need for additional acquisitions, for this measurement.
New knowledge gained
To their knowledge, this is the first study which: Assessed the feasibility of determining relative hepatic uptake of 99mTc-MIBI during rest-phase MPI scan in screening patients for NAFLD Evaluated the effect of different acquisition timings on the results, and Developed a model to predict NAFLD during MPI, based on patient's demographic, laboratory, and multiple time point scintigraphy data
In comparison with the single previously reported study addressing this matter, their study compromised a significantly larger population, including a control group and was performed in MPI setting with all participants undergoing stress phase as well. Having only patients with normal myocardial perfusion included enabled us to omit the interfering effects of reduced myocardial uptake due to any simultaneous ischemic or nonischemic cardiomyopathy.
Conclusions
With regard to the independent risk NAFLD poses for CAD as well as the significant correlation both have with metabolic syndrome, NAFLD may be more prevalent in candidates for MPI scan. Calculating rest-phase 99mTc-sestamibi heart/liver uptake ratio in patients who have been referred for MPI scan to rule out myocardial ischemia may be implemented as a feasible screening tool for NAFLD in this population, with an acceptable accuracy, comparable to several other noninvasive US or laboratory-based screening methods, warranting further evaluation of the patient. Being a secondary finding of MPI scan gives it the prominent advantage of having no additional cost, radiation burden, or adverse effect in this population.
Footnotes
Acknowledgment
The authors wish to show their appreciation to all the patients who graciously participated in this study.
Authors' Contributions
All authors have made substantial contributions to conception, design, as well as acquisition of patients data; have been involved in drafting and revising the article; have given final approval of the version to be published with each of them having participated sufficiently in the work to take public responsibility for appropriate portions of the content; and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethics Approval Statement
This study was approved by the Clinical Research Ethics Committee of the Medical School of Shahid Beheshti Medical University (Trial registration number:
Disclosure Statement
All of the authors, including Ghazal Norouzi, Sara Nikdel, Elahe Pirayesh, Yazdan Salimi, Mahasti Amoui, Hamidreza Haghighatkhah, Mohammad Ali Ghodsi Rad, Elmira Javanijouni, and Sepideh Khoshbakht are employed by Shahid Beheshti University of Medical Sciences, School of Medicine, which primarily focuses on education and medical research.
Funding Information
No funding was received for this article.