
Abstract
Immunotherapy with immune checkpoint inhibitors (ICIs) changed the treatment management in several solid metastatic tumors with very poor prognosis, in particular in melanoma stage IV since its introduction in 2011. However, it is not yet fully understood why some patients respond to ICIs and others not, and it is also unclear why melanomas are the most sensitive tumors to ICI treatment. Selection criteria for patient stratification are needed and several approaches are under evaluation. These include the PD-L1 expression in the tumor samples, assessment of the tumor mutational burden as well as radiological and molecular imaging techniques, such as positron emission tomography (PET)-CT and PET-MRI with 18F-fluorodeoxyglucose (FDG) or novel radiopharmaceuticals. In the near future, a more holistic approach based on the combination of imaging data and sequencing data and the development of radiogenomic signatures will be needed for a better characterization of immunotherapy response and selection of patients who will benefit from ICI therapy alone or in combination with chemotherapy.
Introduction
In the past years, immunotherapy has revolutionized the landscape of treatment for several solid tumors, mostly in advanced stage and with poor prognosis. The best example is metastatic melanoma with an expected overall survival between 6 and 7 months 20 years ago versus a 5-year survival rate of ∼50% in the current era after the introduction of immune checkpoint inhibitors (ICIs). 1 ICIs brought definitely a paradigm shift in the therapeutic management of metastatic melanomas and, moreover, changed the treatment paradigm in several other tumor types as well, either alone or in combination with chemotherapy, for example, in cancers of the lung, kidney, prostate, bladder, pancreas, head-and-neck, and many other solid organs, along with selected hematological tumors. 2
The first ICI was ipilimumab, a CTLA-4 inhibitor approved in 2011 by the FDA for metastatic melanoma, followed by the PD-1 inhibitors pembrolizumab and nivolumab in 2014. Interestingly, the combination of ipilimumab and nivolumab was very successful with a 5-year survival rate of 52% as compared with 44% for nivolumab alone and 26% for ipilimumab alone as demonstrated by Larkin et al. in the CheckMate 067 study, which included 945 patients with previously untreated, unresectable, or metastatic melanoma with known BRAF V600 mutation status. 3 In general, ICIs activate the patient's immune system by blocking the inactivation of T cells.
However, the therapeutic effect depends on the individual immune system and most probably some kind of pre-existing immune response is needed for a good therapeutic result, in terms of pre-existing tumor-reactive T cells before the treatment, as demonstrated by several pathological studies. 4 That being said, it is not yet fully understood why some patients respond to ICIs and others do not, and it is also unclear why melanomas are the most sensitive tumors to ICI treatment.
Selection of Patients for ICI therapy
Selection of patients who will benefit from ICI therapy remains a difficult task. One approach consists in assessing the PD-L1 expression in tumors. Newer results in colorectal cancer demonstrate a benefit of PD-1 inhibition therapy in patients with deficient mismatch DNA repair system (dMMR) resulting in microsatellite instability (MSI). For example, Wang et al. demonstrated higher response rates, higher progression-free survival (PFS), and a significant increase in T lymphocyte infiltration in patients with higher microsatellite instability (instability loci ≥3). 5 However, the PD-L1 expression does not have a predictive role in melanoma as demonstrated in a meta-analysis based on 1062 patients. 6
The results are different in patients with lung cancer. In a meta-analysis based on 2792 patients with small-cell lung cancer, a positive PD-L1 expression was a favorable, although not statistically significant, prognostic factor. 7 In patients with nonsmall-cell lung cancer, ICIs improve survival, and high PD-L1 expression in at least 50% of tumor cells can be used to select patients for pembrolizumab monotherapy, but PD-L1 expression is not a reliable biomarker according to recent results. 8,9 In patients with renal cell carcinomas, PD-L1 expression is not useful as a predictive biomarker, either. 10
One problem may be the heterogeneous PD-L1 expression within a tumor lesion and also between a primary tumor and its metastases, as demonstrated by several studies; for example, Tonse et al. report an overall discordance in PD-L1 expression in 19% of the brain metastases as compared with the primary tumor with the greatest discordance in the 1%–50% expression category. 11 Schoenfeld et al. evaluated PD-L1 and next-generation sequencing (NGS) on the same tissue sample in 1586 patients with lung adenocarcinomas and found that PD-L1 negativity was more common in primary than in metastatic samples.
Accordingly, the predictiveness of PD-L1 expression on ICI response varied by organ. Molecular alterations of certain genes such as KRAS, EGFR, TP53, and STK11 as well as WNT pathway alterations are associated with PD-L1 negativity. They concluded that PD-L1 must be interpreted within the context of these features. 12
Tumor mutational burden (TMB) is another promising approach for the selection of patients for ICI treatment. FDA approved pembrolizumab in solid tumors with TMB ≥10 mutations/megabase based on the FoundationOne CDx assay and the results of the KEYNOTE-158 study, a single-arm phase II multicohort study of pembrolizumab in previously treated advanced solid tumors. 13 However, it is known that some tumor types with low TMB, such as recurrent glioblastomas, benefit from ICIs. 14
Furthermore, TMB results from targeted NGS can show considerable variability, especially when smaller panels are used and are affected by the spatial tumor heterogeneity. 15,16 Strickler et al. present in a recent perspective article further limitations of the use of TBM as an immunotherapy predictor, such as TMB thresholds across different solid tumors, the biochemical and cellular composition of the tumor immune microenvironment, differences in response between inflamed and noninflamed tumors, and conclude that although a patient with a BRAF wild-type melanoma is highly unlikely to respond to a BRAF inhibitor, patients with negative PD-L1 expression or a low TMB may respond to PD-1 inhibitors. 17 –19
Experimental ICIs and next-generation immunotherapeutics
New ICIs beyond CTLA-4 and PD-1 are presented in several recent review articles. 20,21 Such new therapies include next generation of anti-CTLA-4 and anti-PD-1 antibodies but also other ICIs, such as LAG3 inhibitors. LAG3 blockers may be used as a monotherapy or in combination with PD-1 inhibitors as an alternative therapy to CTLA-4 and PD-1 inhibition. In a trial with melanoma patients, the combination of relatlimab, a human IgG4 LAG-3 blocking antibody, with nivolumab demonstrated an improved PFS of 47.7% for the combination therapy versus 36% at 12 months for nivolumab monotherapy and a median PFS of 10.1 months versus 4.6 months accordingly.
In contrast, the incidence of grade 3/4 immune-related adverse events (irAEs) was higher for the relatlimab/nivolumab combination than for nivolumab monotherapy (18.9% vs. 9.7%), and also treatment discontinuation was 14.6% for the combination therapy versus 6.7% for nivolumab monotherapy. 22 Other experimental ICIs are discussed within the review article by Korman et al. 20 , whereas the newest development in next-generation immunotherapeutics for solid tumors, especially multispecific antibodies and cell therapies, has been covered in other recent reports. 23 –25
PET-Based Immunoimaging for Assessing Immunotherapy Outcomes
Positron emission tomography (PET)-based immunoimaging includes therapy monitoring of different immunotherapies or their combination as well as prediction of immunotherapy outcome based on dedicated nonflurodeoxyglucose (FDG) radiopharmaceuticals.
Clinical approach: use of 18 F-FDG for immunotherapy monitoring
In terms of molecular imaging, mainly PET-CT with the radiotracer 18 F-FDG is in use. 18 F-FDG PET imaging has nowadays a great impact on the diagnostics and therapy management of oncological patients and has gained increasing use worldwide. 26 In contrast, despite being a valuable tool in diagnosis, prognosis, and therapy monitoring, 18 F-FDG PET-CT has some limitations, mainly related to the unspecific tracer uptake. The current trend is toward more specific tracers, mostly peptides. Two successful examples are radiolabeled prostate-specific membrane antigen analogues and DOTA0-Phe1-Tyr3 octreotide, which clearly improved diagnosis and also facilitated therapeutic application of radionuclides in advanced prostate cancer and neuroendocrine tumors, respectively, resulting in longer patient survival. 27,28
The role of 18 F-FDG PET/CT in immunotherapy monitoring is increasing. Most data exist in melanoma, a highly 18 F-FDG-avid tumor. Despite the unspecific nature of the tracer, the wide use of 18 F-FDG demonstrated its usefulness in ICI monitoring (Fig. 1). Different response patterns have been reported, concordant with the those reported from CT studies, and different set of criteria for response monitoring are under evaluation, including changes in the standardized uptake value (SUV), number of new lesions, or their combination. 29 –31

Longitudinal FDG PET-CT studies in a patient with metastatic melanoma. MIP images before pembrolizumab therapy, after four cycles of pembrolizumab, and after two cycles of ipilimumab and nivolumab. The patient demonstrated a progression after four cycles of pembrolizumab with increase of the number of new lesions, increase of FDG uptake and functional tumor volume, and unfortunately a progression after a combined ipilimumab and nivolumab therapy. FDG, flurodeoxyglucose; MIP, maximum intensity projection; PET, positron emission tomography.
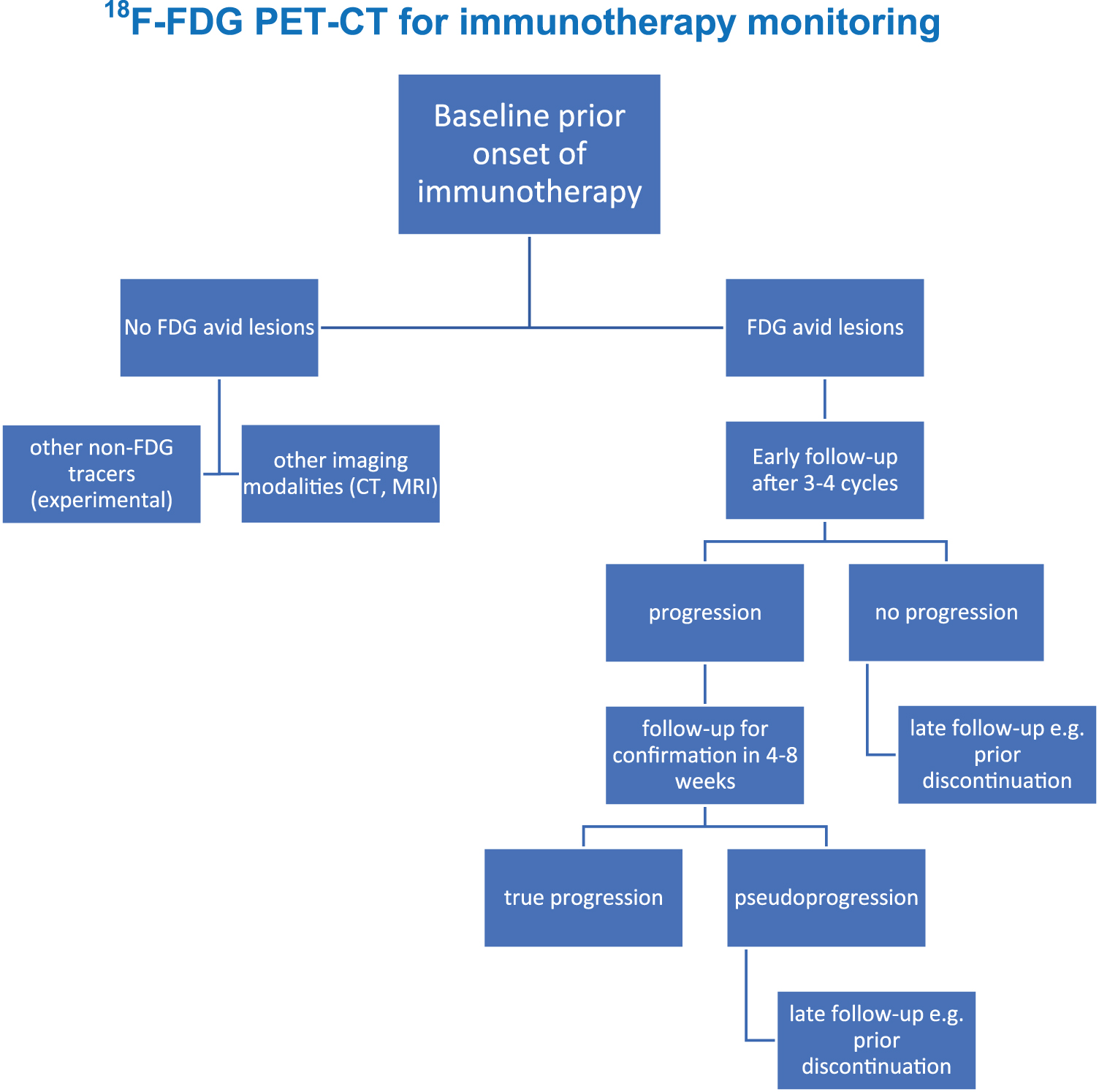
The first guidelines for immunoimaging with 18 F-FDG PET/CT have been recently published and provide a guidance for standardization of its use and interpretation of the PET/CT scans, in particular for the evaluation of response assessment. These guidelines recommend the use of a baseline study before the start of treatment, an interim PET-CT after three to four cycles and a study before ICI discontinuation.
Furthermore, in case of progressive metabolic disease, a confirmatory follow-up study 4–8 weeks after the interim study is recommended to exclude atypical response patterns, such as pseudoprogression (Fig. 2). Moreover, it is recommended to describe the appearance, extent, severity, and variation of irAEs that may be observed in 18 F-FDG PET-CT within immunotherapy monitoring. 32
Of special clinical interest is also oligoprogressive disease (OPD), which occurs in ∼10%–20% of ICI-treated patients with lung and other cancers and offers the opportunity to prolong survival through the application of local ablative therapies (LATs) according to recently published randomized data from the consolidative use of radiotherapy to block oligoprogression study (NCT03808662). 33,34 Of note, other studies have shown that PET-CT can identify significantly more OPD cases suitable for LATs due to its higher sensitivity compared with plain CT. 35
Another interesting aspect is the visualization of irAEs. The activation of the host immune system by the ICI treatment may lead to inflammatory side-effects, known as irAEs due to the hyperactivation of the immune system. The toxicity profiles are different dependent on the ICI therapy used. CTLA-4 inhibitors cause often colitis or hypophysitis, whereas PD-1 inhibitors are related to thyroiditis, arthralgia, or pneumonitis. 36 Patients with mild irAEs do not require immunosuppressive treatment and ICI therapy can be continued or temporarily stopped.
In cases of severe irAEs, ICI discontinuation is required along with treatment of the side-effects. 37 Usually, irAEs are diagnosed clinically. Some irAEs, frequently asymptomatic, are diagnosed by imaging modalities, such as 18 F-FDG PET-CT. Sachpekidis et al. summarize in a review article the most common adverse events observed with 18 F-FDG PET-CT under immunotherapy as well as the impact of the irAEs on response assessment. 38 Importantly, there is increasing evidence that irAEs may be related to improved response rates and longer survival under immunotherapy, even after adequate control of “immortal-time bias,” which was an issue in some earlier reports. 39,40
The prognostic value of the 18 F-FDG uptake in lymphoid organs, such as the spleen, as well as their changes during immunotherapy, is another interesting aspect. However, the results in this field are still inconclusive, therefore, this issue remains open. Sachpekidis et al. demonstrated a poor performance of the tracer uptake in the spleen at baseline as well as of its changes during ipilimumab monotherapy for predicting clinical benefit in metastatic melanoma. 41 Schwenck et al. report on divergent results between mice studies and patient data.
ICI-treated mice demonstrated an increase in the spleen 18 F-FDG uptake during therapy, whereas no significant differences were observed in patients. 42 Furthermore, Prigent et al. showed that an increase in SLRmean (spleen SUVmean/liver SUVmean) >25% at 3 months after initiation of immunotherapy, compared with baseline, is associated with poor outcome (overall survival) in melanoma patients. 43
Novel radiopharmaceuticals
Visualization of cancer-associated fibroblasts
Another novel approach consists in the use of fibroblast activation protein inhibitor (FAPI) imaging in oncological patients, since it is known that FAP is overexpressed in the cancer-associated fibroblasts of many solid tumors. Until now, different radiolabeled FAPI analogues, labeled either with 18 F or with 68Ga, have been tried in small patient collectives. Most of the reported results are within retrospective studies. Some data exist on the comparison of FAPI radioligands with 18 F-FDG for diagnostic purposes.
Giesel et al. studied retrospectively 71 patients with different tumor types and demonstrated comparable tumor uptake for different 68Ga-FAPI ligands and 18 F-FDG but lower 68Ga-FAPI uptake in most normal organs, resulting in equal or higher tumor-to-background ratio and better tumor detection in some individual patients with low 18 F-FDG-uptake tumors, such as ovarian cancer and pancreatic cancer. 44 Chen et al. compared in a prospective study 68Ga-FAPI-04 with 18 F-FDG in 75 patients with different tumor types and reported a higher detection rate for FAPI (98.2%) than for FDG (82.1%) and a better sensitivity in the detection of lymph node (86.4% vs. 45.5%) as well as bone and visceral metastases (83.8% vs. 59.5%). 45
Similarly, Wang et al. reported better results for 68Ga-FAPI than for 18 F-FDG in 34 patients with advanced lung cancer, in particular for the detection of metastases in the brain, lymph nodes, bone, and pleura. 46 Qin et al. reported a high diagnostic performance for 68Ga-FAPI in tumors of the gastrointestinal tract with low 18 F-FDG uptake, such as some gastric tumors or already treated colorectal metastases. 47 Further prospective studies are needed to clarify the impact of FAPI analogues in comparison with 18 F-FDG for diagnosis and therapy management.
These first results demonstrate, however, that FAPI may have superiority in tumors that exhibit low 18 F-FDG uptake. No data exist on the use of FAPI for immunoimaging at the moment. It is open up to now whether combined double tracer studies with 18 F-FDG and FAPI may improve imaging and monitoring of low uptake 18 F-FDG tumors after immunotherapy, such as some types of lung adenocarcinomas.
Prediction of immunotherapy response: PD-1 and PD-L1 imaging, T cell tracking
Another approach for immunoimaging consists in the use of tracers, which are related to the PD-1 and PD-L1 expression. The idea is to perform whole body PD-1 or PD-L1 imaging to better stratify patients for immunotherapy with ICIs. The advantage of this approach is the assessment of the whole-body expression of these targets and not just in a biopsy probe, since tumors are quite heterogeneous. The first studies in patients with nonsmall-cell lung tumors and the tracers 89Zr-nivolumab, 89Zr-atezolizumab, or 18F-BMS-986192 have already been published. 48,49 The authors demonstrated a significant heterogeneity of these traces between patients, as well as within different tumor lesions of the same patient.
Another very new approach is the use of the so-called T cell imaging. First results have been recently published using a 89Zr-anti-CD8 minibody (89Zr-IAB22M2C) in six patients with solid tumors, including melanomas, lung tumors, and hepatocellular carcinomas. A prominent uptake was observed not only in the spleen, bone marrow, liver, and normal lymph nodes but also in tumor lesions ca. 2 h after the tracer injection with most tumor lesions best detectable by 24 h p.i. 50
The authors used also 18 F-FDG for comparison and found both concordant and discordant results, suggesting that each tracer reflects different molecular processes. Ideally, multitracer studies with 18 F-FDG, PD-1, or PD-L1 ligands as well as T cell imaging may be used for immunotherapy monitoring because they provide complementary information, which is valuable for stratification of therapy.
Finally, newer immune checkpoints beyond CTLA-4 and PD-1/PD-L1 have been studied, such as the T cell immunoglobulin and immunoreceptor tyrosine-based inhibitory motif (ITIM) domain (TIGIT) receptor. TIGIT is expressed on CD4 and CD8 T cells, on natural killer cells and regulatory T cells. Recently, first human studies have been published using a Ga-68-peptide antagonist (68Ga-GP12) for PET imaging of the TIGIT expression. 51 The authors studied two patients with lung adenocarcinoma and found an enhanced uptake in both primary and metastatic lung tumors comparable with 18 F-FDG but with lower values, indicating that each tracer provides different molecular information. Moreover, the expression of TIGIT in the primary tumors was confirmed by immunohistochemistry.
Figure 3 shows an overview of the novel radiopharmaceuticals already mentioned.

Selected PET radiopharmaceuticals for immunoimaging. CAF, cancer-associated fibroblasts; FAPI, fibroblast activation protein inhibitor; 18 F-FLT, F-18-fluorothymidine.
Conclusions
In conclusion, and contemplating the future of molecular imaging, the adoption of fourth-generation PET-CT scanners with extended field of view, which provide higher sensitivity, faster scanning protocols, application of less tracer activity, and more sophisticated reconstruction and image evaluation algorithms based on artificial intelligence (AI) approaches, will further improve immunotherapy monitoring in solid tumors. 52 All these features will facilitate longitudinal PET-CT studies due to less radiation dose and allow late imaging (e.g., for 89Zr tracers). The development of AI-based radiogenomic signatures may also aid in this direction.
New dedicated tracers, specifically targeting PD-1 and PD-L1 inhibitors as well as T cell imaging, will complement 18 F-FDG and improve stratification as well as the assessment of immunotherapy outcome based on noninvasive imaging techniques. The combination of imaging data and sequencing data of tumor probes, including whole genome sequencing, RNA sequencing, exome sequencing, and gene expression, will provide a more holistic approach for the characterization of immunotherapy response in the near future and will allow a stratification of therapeutic approaches.
In addition, pivotal studies in small series suggest that longitudinal radiological assessment with novel molecular tracers combined with serial assays of cell-free DNA could facilitate earlier detection of disease progression, improved distinction from pseudoprogression, increased yield of OPD, and better prediction of long-term benefit than each method alone. 53 –56 Large prospective multicenter studies will be essential to confirm these promising signals; expand the scope of immunoimaging in the routine setting; and characterize the optimal combination of tracers, protocols, and radiogenomic signatures for immunotherapy assessment.
Footnotes
Authors' Contributions
A.D.-S. conceived the original idea and wrote the article. C.S., J.C.H., and P.C. revised the article and contributed to the final version.
Disclosure Statement
P.C. has received research funding from AstraZeneca, Novartis, Roche, and Takeda; speaker's honoraria from AstraZeneca, Novartis, Roche, and Takeda; support for attending meetings from AstraZeneca, Eli Lilly, Gilead, Novartis, and Takeda; and personal fees for participating to advisory boards from Boehringer Ingelheim, Chugai, Pfizer, and Roche, all outside the submitted study. J.C.H. received honoraria from Bristol Myers Squibb (BMS), Merck Sharp & Dohme (MSD), Novartis, Roche, Pierre Fabre, Sanofi, and Almirall; consultant or advisory role from MSD, Pierre Fabre, and Sunpharma; and Scientific support from BMS; and travel support from Pierre Fabre, all outside the submitted study. All other authors declare no competing interests.
Funding Information
No funding was received for this article.