
Abstract
Background:
Delivery of radiotherapeutic dose to recurrent head and neck cancer (HNC) is primarily limited by locoregional toxicity in conventional radiotherapy. As such, HNC patients stand to benefit from the conformal targeting of primary and remnant disease achievable with radiopharmaceutical therapies. In this study, the authors investigated the tumor targeting capacity of 131I-CLR1404 (iopofosine I-131) in various HNC xenograft mouse models and the impact of partial volume correction (PVC) on theranostic dosimetry based on 124I-CLR1404 (CLR 124) positron emission tomography (PET)/computed tomography (CT) imaging.
Methods:
Mice bearing flank tumor xenograft models of HNC (six murine cell line and six human patient derived) were intravenously administered 6.5–9.1 MBq of CLR 124 and imaged five times over the course of 6 d using microPET/CT. In vivo tumor uptake of CLR 124 was assessed and PVC for 124I was applied using a novel preclinical phantom. Using subject-specific theranostic dosimetry estimations for iopofosine I-131 based on CLR 124 imaging, a discrete radiation dose escalation study (2, 4, 6, and 8 Gy) was performed to evaluate tumor growth response to iopofosine I-131 relative to a single fraction of external beam radiation therapy (6 Gy).
Results:
PET imaging demonstrated consistent tumor selective uptake and retention of CLR 124 across all HNC xenograft models. Peak uptake of 4.4% ± 0.8% and 4.2% ± 0.4% was observed in squamous cell carcinoma-22B and UW-13, respectively. PVC application increased uptake measures by 47%–188% and reduced absolute differences between in vivo and ex vivo uptake measurements from 3.3% to 1.0 percent injected activity per gram. Tumor dosimetry averaged over all HNC models was 0.85 ± 0.27 Gy/MBq (1.58 ± 0.46 Gy/MBq with PVC). Therapeutic iopofosine I-131 studies demonstrated a variable, but linear relationship between iopofosine I-131 radiation dose and tumor growth delay (p < 0.05).
Conclusions:
Iopofosine I-131 demonstrated tumoricidal capacity in preclinical HNC tumor models and the theranostic pairing with CLR 124 presents a promising new treatment approach for personalizing administration of iopofosine I-131.
Introduction
Approximately 50% of patients with head and neck cancer (HNC) manifest recurrence following initial treatment, with the majority of these recurrences being loco-regional (mouth, throat, or neck). 1 Although some of these patients remain potentially curable with further local treatment approaches (surgery, radiation, and chemoradiation), retreatment is technically challenging and accompanied by a significant risk of damage to normal tissues. Surgery is often limited by tumor adherence to critical structures (base of skull, neurovascular structures), whereas external beam radiation therapy (XRT) is often limited by normal tissue tolerance (spinal cord, bone, and cartilage). Although frequently warranted in the attempt to provide disease control, HNC retreatment can induce profound adverse effects on patient health-related quality of life (QOL). 2,3 Therefore, improved treatment approaches for patients with locoregional HNC recurrence are needed.
One promising approach to treat locoregional HNC recurrence is to deliver a targeted radiopharmaceutical agent as an adjuvant to XRT, thereby potentially limiting additional dose to surrounding normal tissues. This would allow for a decrease in the total dose applied through external beam radiation, thereby reducing side-effects, while maintaining or potentially increasing tumor control. Such an approach is of particular significance in HNC because surgery and radiation often compromise normal salivary and swallow function with a powerful adverse impact on patient QOL. 4,5 A promising agent that can be used in the adjuvant setting to treat HNC is iopofosine I-131 (previously referred to as CLR 131), which is an iodinated alkyl phosphocholine (APC) analog with broad cancer-targeting abilities. 6
APC analogs are internalized preferentially by cancer cells through lipid rafts, which are specialized plasma membrane microdomains that spatially organize critical signaling molecules. Malignant cells possess lipid rafts at concentrations 6–10 × higher than normal cells, which is considered a major reason for the almost universal tumor selectivity of these agents regardless of histopathological origin. 7,8 The theranostic properties of CLR1404 can be exploited for tumor imaging by labeling with 124I (CLR 124) and treatment by labeling with 131I (iopofosine I-131). In combination with conventional modalities of cancer treatment, such as XRT, this strategy affords a unique approach to improve therapeutic outcome.
Clinical trials of iopofosine I-131 in a spectrum of hematological cancers (NCT02952508) and pediatric solid tumors (NCT03478462) are ongoing. Preliminary reports in patients with recurrent multiple myeloma are promising with an overall response rate of 40% and over 3 months of progression-free survival. 9,10 Transient cytopenia remains a dose-limiting toxicity in patients treated with high doses of iopofosine I-131, but with moderate dose levels continuing to be effective. 11 While preclinical studies have demonstrated selective uptake and retention of CLR1404 in over 50 tumor models, including several HNCs, there remains a need to further characterize the tumor dosimetry of CLR in HNC models within the context of XRT. 6 Accurate dosimetry in mice is necessary to extrapolate the potential efficacy of a combined approach to humans.
Our group has used positron emission tomography (PET)/computed tomography (CT) imaging of CLR 124 and Monte Carlo radiation transport methods to characterize the biodistribution and estimate organ and tumor absorbed doses (ADs) in mice from iopofosine I-131, thus providing useful information in the early stages of drug development and clinical translation. 12 –14 Corrections for partial volume effects (PVEs) in PET/CT images can also improve the accuracy of dosimetry studies. PVEs lead to an underestimate of tumor uptake in PET/CT images, particularly in small tumor lesions, which lead to an underestimate of tumor ADs. The authors and others have shown that “hot sphere” phantoms can be used to produce recovery coefficient (RC) correction models leading to more accurate tumor dose estimates in preclinical dosimetry studies. 15,16
In this work, the authors evaluated the tumor-selective uptake of CLR 124 in murine and patient-derived xenograft (PDX) models of several HNCs. They introduced a novel 3D printed “hot spheres” phantom to produce a, RC correction model on a cohort of mice bearing HNC xenografts. The RCs derived from the phantom were applied to CLR 124 PET/CT images of HNC xenografts and compared to biodistribution data from the same tumor-bearing mice. Monte Carlo dosimetry was performed on both corrected and uncorrected image datasets to demonstrate the dosimetric impact of accounting for PVEs.
Materials and Methods
Radiopharmaceuticals
Methods for synthesis of CLR1404 and radiolabeling with 124I or 131I have been described previously. 6,17 Briefly, radio-iodination of CLR1404 was accomplished through isotope-exchange reaction with sodium iodide. Radiochemical purity of CLR 124 and iopofosine I-131 exceeded 96% with radiochemical yields consistently above 70%. Cellectar Biosciences (Florham Park, NJ) provided clinical grade iopofosine I-131 as well as unconjugated CLR1404 for preparation of CLR 124 by Dr. Weichert. 18 124I was obtained from IBA Molecular North America. All radiopharmaceuticals were prepared under good manufacturing practice guidelines.
Human HNC models
In vivo uptake of CLR 124 and theranostic iopofosine I-131 dosimetry was studied in six human HNC cell lines (squamous cell carcinoma [SCC]-2, SCC-6, SCC-22B, SCC-47, SCC-1483, and Tu-138) and six HNC PDX (UW-1, UW-13, UW-22, UW-25, UW-36, and UW-64). Cell lines SCC-1, SCC-6, and SCC-47 were obtained from MilliporeSigma (Burlington, MA), whereas SCC-2, SCC-1483, and Tu-138 were provided by Dr. Henning Bier through Dr. Thomas Carey (Technical University Munich), the Marnett Group (Vanderbilt University), and Dr. Jennifer Grandis (University of Pittsburgh), respectively. All HNC cell lines were cultured as previously described. 19 The authenticity of each cell line was verified within 6 months of cell use by short-tandem repeat profiling (University of Wisconsin-Madison Pathology Core Lab).
PDX models can provide an advantage over established cancer cell lines in predicting patient response to targeted drugs because they more accurately reflect the biological characteristics of human cancers. Briefly, tumor tissue was collected at the time of surgery or staging biopsy from consenting patients (IRB#2016-0934) and transferred to the laboratory in ice-cold culture media containing DMEM. The sample was then minced into <1 mm3 pieces under sterile conditions and mixed in a 1:1 ratio with Matrigel and implanted into 4–6-week-old NOD-SCID gamma mice (NSG, Jackson Laboratories). Subsequent passages are made into either NSG or athymic nude mice in a similar manner. PDX models used in this work were developed and characterized as previously described. 20,21 Two of six PDX models (UW-1 and UW-36) have been validated as human papillomavirus (HPV)+ by p16 staining, a status previously demonstrated to enhance radiation sensitivity. 22
Mice and xenograft tumor models
All animal studies were conducted under National Institutes of Health (NIH) guidelines and Institutional Animal Care and Use Committee-approved protocols. Human tumor xenografts were established in 4–6-week-old female athymic nude mice (Envigo Bioproducts) on the right and/or left hind flank. For cell line-derived tumors, a 200 μL cell suspension containing 1–2 million tumor cells was injected subcutaneously. For the PDX models, tumor tissue was harvested from NSG mice bearing the PDX of interest and implanted into athymic nude mice. Tumor growth was monitored twice per week using digital caliper measurements of the long (L) and short (W) axis of tumors and volume determined using the ellipsoid volume formula
PET imaging and biodistribution of CLR 124
Mice bearing flank tumor xenografts (n = 2–6 per tumor model, n = 48 total) were administered 6.5 or 9.1 MBq of CLR 124 by lateral tail vein injection. Sequential CT and PET scans were acquired in an Inveon micro-PET/CT scanner (Siemens Preclinical Systems, Knoxville, TN) at 1, 24, 48, 72, and 144 h after injection. Before each scan, mice were anesthetized with isoflurane (4% induction and 2% maintenance) and placed in a prone position on the heated scanner bed. CT scans (80 kVp; 1000 mAs; 275 ms; 220 angles) were reconstructed by filtered back projection using the system software with a Shepp-Logan filter to a 0.2 × 0.2 × 0.2 mm3 resolution.
List mode PET scans consisting of 40 million coincidence events per mouse (energy window; 350–650 keV) were reconstructed using a two-dimensional ordered subset expectation maximization (OSEM2D) algorithm with 16 subsets and 4 iterations to a 0.8 × 0.8 × 0.8 mm3 resolution. The resulting PET and CT image volumes were coregistered and corrections for attenuation, normalization, dead-time, and scatter were applied using the system software. Region of interest (ROI) analysis and quantification was performed with contours drawn on the anatomic CT image volumes.
Quantitative in vivo uptake is expressed as percent injected activity per gram (%IA/g), assuming unit density of tissue and correcting for radioactive decay of 124I. Following the final 144-h time point, a subset of mice was sacrificed, and tumor tissue was collected to corroborate the accuracy of in vivo measurements. Tumors were wet-weighed and activity was counted in a Wizard 2 automated γ-counter (Perking Elmer, MA) to calculate the %IA/g ex vivo.
Partial volume correction phantom
The authors assessed the impact of PVE on 124I PET-based tumor uptake and dosimetry in this work with a 3D printed partial volume correction (PVC) phantom (Phantech, Madison, WI). The phantom contains a single-channel series of nine spherical voids ranging from 3.7 to 24.8 mm in diameter. The phantom was filled with 124I solution comparable to in vivo CLR 124 observations and scanned with micro-PET/CT using the same imaging parameters. Recovery of 124I activity concentration (AC) in each sphere was assessed through ROI analysis of the fused PET/CT image volumes. Contours of each spherical void were produced using the CT volume for reference and ROI volumes matched to the known volume of the corresponding spheres. RC was calculated using Equation 1.
The relationship between RC and sphere diameter was then fit to a sigmoidal function to allow for calculation of RC at any sphere diameter corresponding to measured tumor volume delineated in imaging studies.
Correcting for PVE in a defined tumor volume at a single point in time is straightforward. Propagating PVC through to tumor dosimetry, a product of the temporal integration of the spatially varying dose distribution, requires consideration of the entire time-activity curve. The area under the time activity curve of iopofosine I-131 (AUC) incorporating PVC is given by Eq. (2), where RC is a function of the tumor volume over the course of the imaging series. The AD for a given tumor can then be corrected by the ratio of corrected and uncorrected AUC (Eq. 3). Assuming a constant tumor volume over the course of an imaging study, this correction factor is reduced to
Theranostic dosimetry in tumors
Dosimetry for iopofosine I-131 in this study was assessed by in vivo CLR 124 imaging using an in-house internal dosimetry platform as previously described. 12 –14 PET and CT image volumes at each time point were coregistered and resampled to an intermediate voxel resolution (0.4 × 0.4 × 0.4 mm3) using a Mitchell-Netravali resampling filter. Iopofosine I-131 activity distributions were generated from CLR 124 PET images, correcting for differences in radioactive decay rates of 124I and 131I.
AD rate distributions for iopofosine I-131 were generated at each time point using Geant4 (version 9.6) Monte Carlo simulations using the CT and PET volumes to represent the geometry and 131I activity source distributions, respectively. Approximately 15 million 131I decays were simulated in mice at each time point (over 5,000 decays per source voxel) to achieve mean relative error in tumor ROIs of <2%. The mean AD rate in tumor ROIs was determined at each time point and the integral AD was calculated using a trapezoidal fit between imaging time points and assuming physical decay from the final time point. The assumption of prolonged retention of iopofosine I-131 beyond the 144-h imaging time point is supported by observations from previous preclinical and clinical studies. 14,23,24
Radiopharmaceutical therapy with iopofosine I-131
Tumor growth delay was assessed in SCC-2 and Tu-138 xenograft mouse models (n = 6–8) following the administration of iopofosine I-131 radiopharmaceutical therapy (RPT) tailored to achieve tumor dose levels of 2, 4, 6, and 8 Gy. Theranostic dosimetry studies of CLR 124 in representative tumor-bearing mice informed the prescription of iopofosine I-131 to SCC-2 (0.78 Gy/MBq) and Tu-138 (1.16 Gy/MBq) tumors.
Mice bearing SCC-2 xenografts received 2.6, 5.1, 7.7, or 10.2 MBq, while mice bearing Tu-138 xenografts received 1.8, 3.6, 5.4, or 7.2 MBq of iopofosine I-131. Mice receiving cold CLR1404 were used as control. An additional group of mice in each cohort was treated with 6 Gy of tumor-targeted XRT using an X-RAD 320 irradiator (Precision X-Ray, Inc., North Branford, CT). RPT experiments were carried out once tumors achieved a volume of ∼400 mm3. Tumor volume was assessed using caliper measurements twice weekly for 4 weeks following treatment.
Clonogenic assays were performed for SCC-2 and Tu-138 cell lines to characterize in vitro response to radiation. Cells were seeded to 6-well plates at specified quantities (n = 3) and irradiated by 0, 2, 4, 6, or 8 Gy using the X-RAD 320 irradiator. After 10–14 d of incubation, cells were fixed and stained with 5% crystal violet in methanol and counted. Clonogenic survival was fit to a linear-quadratic model using nonlinear least squares to quantify characteristic radiobiological factors. 25
Statistical analysis
To assess the reproducibility and accuracy of PVC in vivo uptake with respect to ex vivo measurements, four metrics were estimated. To assess raw correlation between the measurements, Pearson's correlation coefficient was estimated. Second, intraclass correlation coefficients (ICCs) were estimated from linear mixed models. In this context, ICC is the estimated ratio of between-animal variance over the total variability observed (sum of between-animal and between-modality variance), a larger ICC (closer to one) represents smaller error between the in vivo and ex vivo measurements.
To quantify how close the in vivo and ex vivo measurements were (on the units of observation), a repeatability coefficient was calculated. By construction, this value represents the value at which the authors would expect pairwise differences (in vivo measurement—ex vivo measurement) to fall under, with 95% probability. A smaller repeatability coefficient is desired. Finally, to determine if there was evidence of systemic bias between the in vivo and ex vivo measurements, paired t-tests were calculated. A smaller p-value provides evidence against the null hypothesis that the mean pairwise difference is zero.
To assess the variance in time-to-tumor-tripling (TT) between the dosage groups, a Cox proportional hazards model was fit to both the SCC2 and TU-138 data. Estimated hazard ratios (HR) and associated 95% confidence intervals can be seen in Figure 4. A likelihood ratio p-value was calculated from a linear trend test to assess if there was evidence of a linear decrease in the HR as dosage increased.
To model the clonogenic survival data, a linear-quadratic protracted radiation model was fit to the surviving fraction (SF) data using nonlinear least squares. The estimated predictive error was calculated using a second-order Taylor expansion. 26
Results
Recovery of 124I in microPET/CT
A PVC phantom was used to assess and validate the preclinical microPET/CT scanner ability to perform quantitative imaging of 124I in spherical target volumes of varying size (Fig. 1). With a solution AC of 298 kBq/mL, the phantom was imaged with microPET/CT acquiring 120 million coincident events per scan. PET images were then reconstructed with the same parameters used for mice studies. ROIs drawn on the corresponding CT image volume for each of the nine spheres were used to assess recovery, with the mean difference between the volume of reference ROIs and known sphere sizes being 0.6% ± 4.6%. Recovery of 124I is shown plotted against sphere diameter in Figure 1C. The largest sphere at 25 mm in diameter exhibited the highest recovery at 0.823. Recovery of 124I began to drop appreciably in spheres at or below 9.8 mm in diameter.
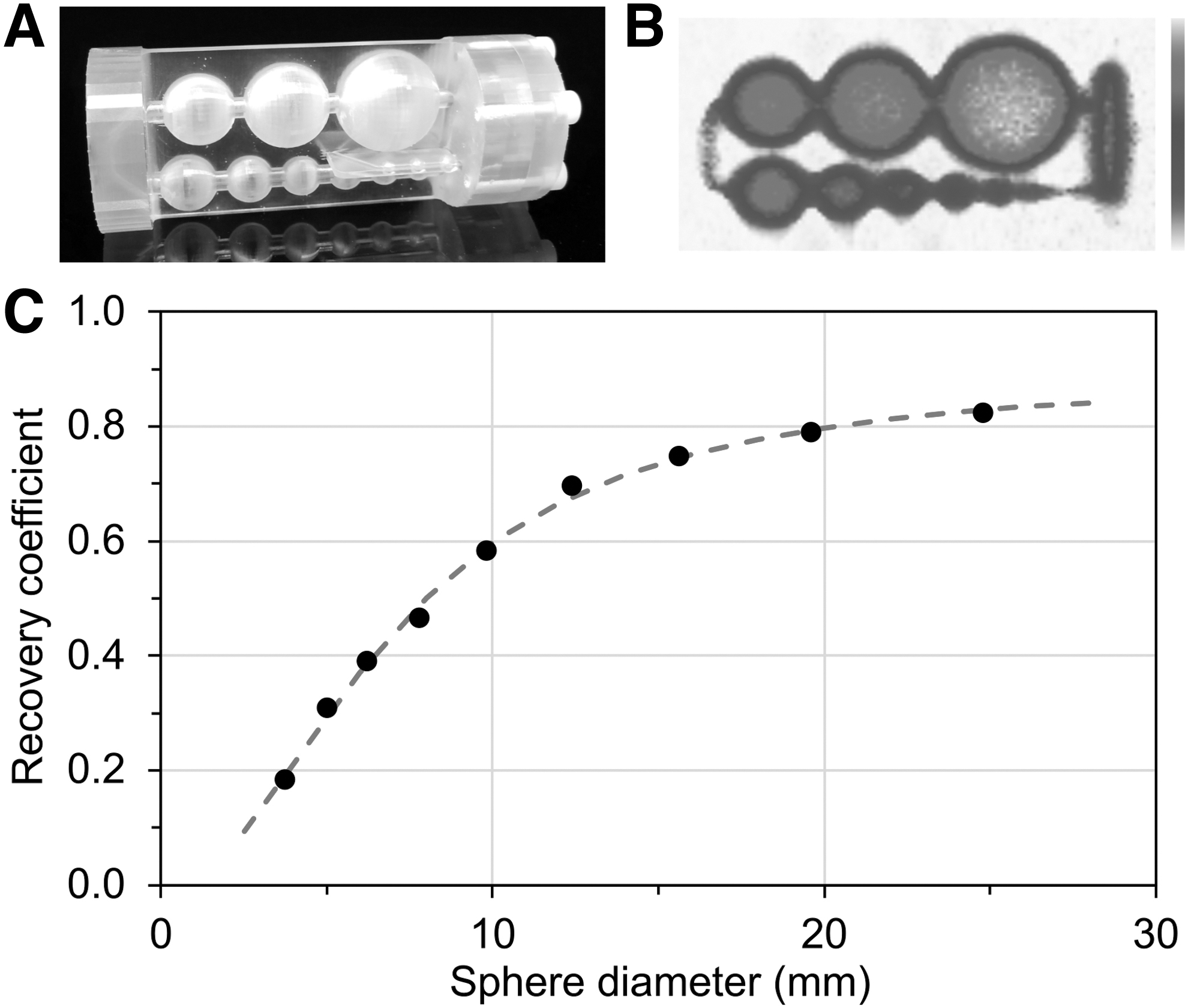
PVC phantom analysis for 124I in microPET/CT imaging.
CLR 124 targets HNC cells in vivo
Longitudinal PET/CT imaging studies over the course of 6 d demonstrated the capacity of CLR 124 to target HNC and established an in vivo model for iopofosine I-131 tumor dosimetry (Fig. 2). Maximum intensity projections of PET images in representative mice show selective uptake and retention of CLR 124 in human xenograft HNC models and limited uptake in normal tissues (Fig. 2A). The biodistribution of CLR 124 in normal tissues (Supplementary Fig. S1) indicated hepatobiliary clearance of the agent driven by elevated heart (blood pool) activity, as previously reported. 14,27,28 ROI analysis of tumor uptake at 1, 24, 48, 72, and 144 h after injection showed peak uptake of CLR 124 was achieved by 48–72 h with durable retention through 144 h. The cohorts exhibiting highest uptake were SCC-22B (4.37 ± 0.81%IA/g at 144 h) and UW-13 (4.23 ± 0.41%IA/g at 144 h).

PET/CT imaging and ROI analysis of flank tumor-bearing mice following intravenous administration of CLR 124.
However, uptake in the remaining PDX models (Fig. 2C, Supplementary Fig. S2B) was notably lower than that observed in cell line-derived xenografts (Fig. 2B, Supplementary Fig. S2A), with UW-36 tumors showing little to no appreciable uptake of CLR 124 (max of 1.98 ± 0.23%IA/g at 48 h). Accounting for PVC, the 144-h uptake for cell line-derived xenograft and PDX models was 5.67 ± 1.62%IA/g and 4.19 ± 1.60%IA/g, respectively. The average tumor volume at the time of imaging was 381 ± 253 mm3 with PDX tumors experiencing slower growth (80 ± 93 mm3) over the course of 6 d than that observed in cell line-derived xenografts (108 ± 149 mm3).
Ex vivo biodistribution studies were performed in a subset of mice (SCC-6, SCC-22B, Tu-138, UW-1, UW-13, and UW-64) immediately following the final imaging time point to verify in vivo tumor uptake. Uptake measurements by ex vivo biodistribution confirmed relative trends observed in vivo with the highest uptake again observed in the SCC-22B (8.01 ± 1.55%IA/g) and UW-13 (9.71 ± 1.06%IA/g) cohorts.
Accuracy of in vivo uptake improves with PVC
For a subset of mice used in CLR 124 imaging and dosimetry studies (n = 24), tumor tissue was excised following the final imaging time point (144 h) and an additional ex vivo biodistribution measure of uptake was acquired. PVC using phantom measured RC was applied to in vivo uptake based on the mean segmented tumor volume observed over the course of the imaging study. Tumor volumes in mice ranged between 4.8 and 11.6 mm in diameter, assuming spherical geometry. The accuracy of in vivo uptake improved significantly (Fig. 3A) following PVC with the absolute difference between in vivo and ex vivo measurements being reduced from 3.50%IA/g to 0.99%IA/g. While the paired t-test p-value (p < 0.0001) suggests evidence of a systematic bias between the initial in vivo and ex vivo measurements, following PVC, the p-value increased (p > 0.05), indicating a lack of evidence for systematic bias once PVC is applied.

Impact of PVC on in vivo uptake measures relative to ex vivo.
The intraclass correlation between in vivo and ex vivo uptake increased from 0.24 to 0.77 after PVC, and the repeatability coefficient decreased from 0.05 to 0.03 following PVC. The three metrics above provide evidence of increased reproducibility and repeatability of the PVC. The magnitude of ex vivo uptake was, on average, 48% ± 14% higher compared with PET-based measures (Fig. 3B) with the largest difference in uptake (66.8% and 67.4%) observed in the smallest tumor volumes (74 and 99 mm3, respectively). This volume-dependent variability in in vivo uptake was reduced following PVC. Inadequate resection of one SCC-6 tumor resulted in artificially low ex vivo uptake and has been excluded from this analysis. Figures and analysis, including this data point, are shown in Supplementary Figure S3.
Theranostic CLR 124/iopofosine I-131 tumor dosimetry
Longitudinal PET/CT imaging studies of CLR 124 in mice (n = 2–6) were used to estimate tumor dosimetry for a single fraction of iopofosine I-131 in each xenograft tumor model. Estimates of cumulative AD prescriptions (Gy/MBq) of iopofosine I-131 RPT are shown in Table 1. Tumor models that demonstrated the highest uptake of CLR 124, SCC-22B, and UW-13 also exhibited the highest iopofosine I-131 prescription doses (1.31 ± 0.27 and 1.24 ± 0.08 Gy/MBq, respectively). Given the improved quantification of in vivo uptake with PVC, the authors further applied RC factors to the in vivo dosimetry results using Equation 3.
Subject-Specific Tumor Dosimetry for Iopofosine I-131 in Tumor-Bearing Mice
AD, absorbed dose; PVC, partial volume corrections; SCC, squamous cell carcinoma.
Following PVC, iopofosine I-131 prescription doses for tumors increased by 64%–125% (mean, 87% ± 17%). Overall trends observed across tumor models remained consistent following PVC. On average, the corrected tumor dose for cell line-derived xenograft models, 1.75 ± 0.44 Gy/MBq, was 24% higher than that observed in PDX models, 1.40 ± 0.46 Gy/MBq.
Tumor growth inhibition increases with iopofosine I-131 AD
A comprehensive study was performed to probe the response of HNC tumors to escalating levels of iopofosine I-131 radiation dose relative to that of conventional XRT. Iopofosine I-131 was prescribed at 2, 4, 6, and 8 Gy using non-PVC theranostic dosimetry results. The radiation dose delivered based on PVC dosimetry was 3.3, 6.6, 9.8, and 13.1 Gy for SCC-2 or 3.4, 7.0, 10.4, and 13.9 Gy for Tu-138, which maintains discrete and comparable dose levels. Figure 4 provides a summary of tumor dose–response in SCC-2 and Tu-138.
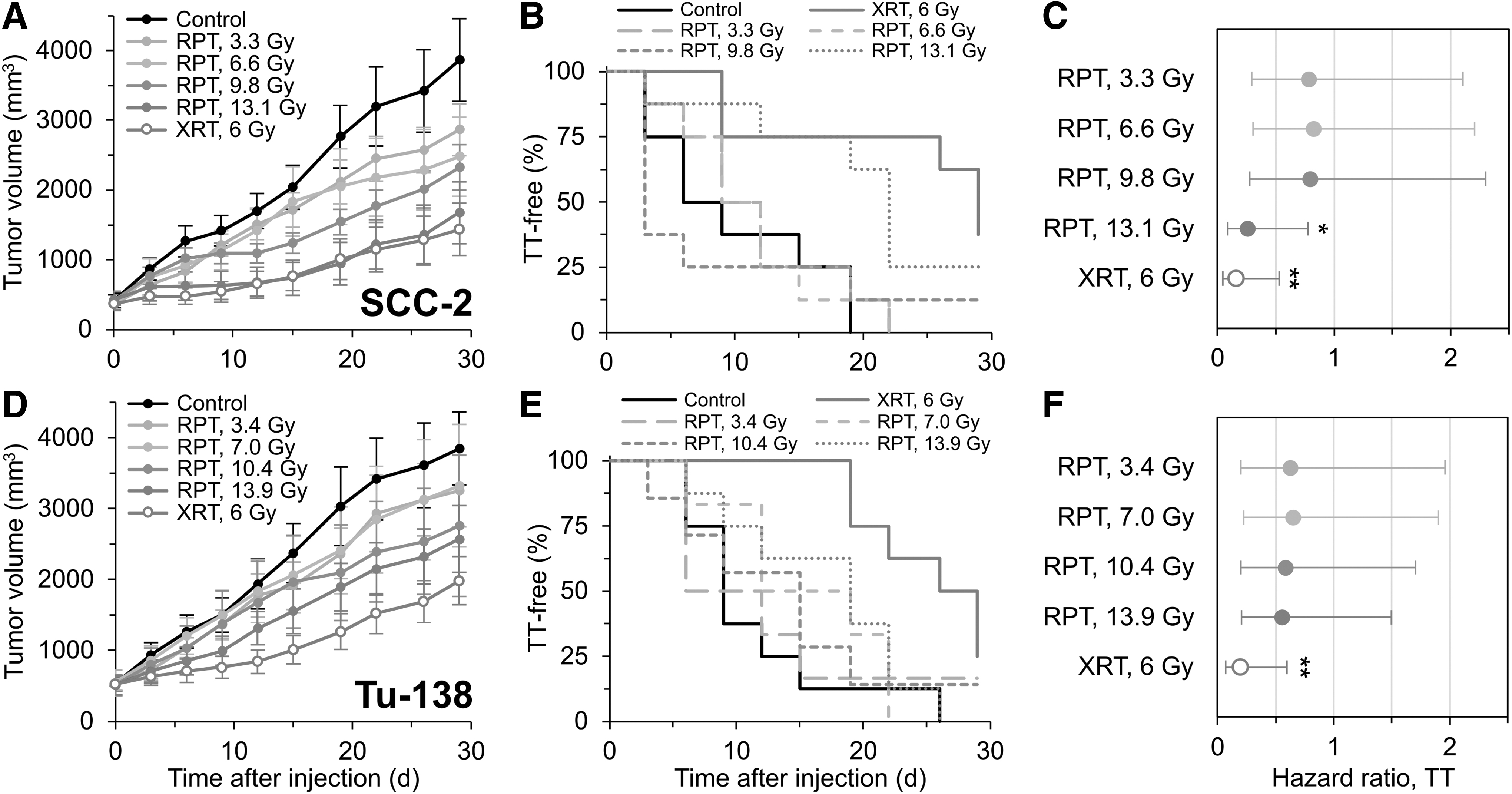
Dose escalation and tumor response to iopofosine I-131 in SCC-2
Overall, significant growth delay is observed in SCC-2 tumor models with mean tumor growth for the 8 Gy iopofosine I-131 cohort following closely with 6 Gy XRT (Fig. 4A). To assess the variance in growth across the treatment groups, a time-to-event analysis, where the event was defined as TT, was performed using a Cox proportional hazards regression model. From this model, it was found that the 6 Gy XRT cohort exhibited the largest deviation from control in both SCC-2 and Tu-138 (Fig. 4B, E). The response of each cohort varied relative to control over the course of observation, although this variation failed to reach statistical significance, given the high level of within-group heterogeneity observed.
In Figure 4, there is a slight linear relationship between radiation dose and TT-free survival for SCC-2 (p < 0.02) with respect to estimated HR (Fig. 4C), but no statistically significant correlation observed for Tu-138, despite the data trending toward lower HR with increasing dose. For both models, the 6 Gy XRT cohort exhibited statistically significant response (p < 0.005). However, only the 8 Gy group for SCC-2 showed significant response to iopofosine I-131 (p < 0.02). In all iopofosine I-131 treatment groups, an HR of <1 was observed. Following administration of iopofosine I-131, mice exhibited transient weight loss at the highest dose cohorts, but no sign of severe adverse effects on health status.
Clonogenic assays of SCC-2 and Tu-138 showed markedly different in vitro response to XRT with SCC-2 cells responding more severely than Tu-138 for the same radiation dose (Supplementary Fig. S4). The α/β parameters derived from the linear-quadratic model were 1.99 Gy for SCC-2 and 2.58 Gy for Tu-138, both indicative of late responding tissues. In clinical terms, a lower α/β ratio indicates a higher biological effective dose for a given fractionation scheme with conventional XRT.
Discussion
Reirradiation of recurrent and unresectable HNC has proven to be an effective, yet challenging, treatment approach in the clinic. Advances in conformal XRT have improved disease control and survival, but high risk of significant locoregional toxicity remains dose limiting. In recent years, there has been a growing interest in the use of RPT agents, with toxicity concerns oriented toward red marrow and clearance organs, in combination with conventional therapies. 29 However, despite HNC emerging early on as a promising target, 19 the capacity for CLR1404 to broadly target HNC and deliver effective radiation dose has not been thoroughly studied. In this study, the authors have investigated the tumor targeting capacity of CLR 124 and iopofosine I-131 against HNC, in vivo, and explored the incorporation of PVC in theranostic dosimetry to allow for more accurate assessment dose delivered by iopofosine I-131 RPT.
PET/CT imaging of CLR 124 in flank tumor-bearing mice showed selective uptake and retention in a broad spectrum of both cell line and PDX HNC models. The biodistribution of CLR 124 in normal tissues, as reported in Supplementary Figure S1, demonstrated hepatobiliary clearance of CLR 124 and prolonged retention in blood aligns with observations from prior preclinical investigations of CLR 124. 14,27,28 Notably, PDX models exhibited 26% lower uptake compared with cell line-derived models, on average, despite UW-13 demonstrating the second highest uptake of all tumor models. The source of this discrepancy is multifaceted. Cosper et al explain that tumor stromal microenvironment and confluence of human and mouse tissue affect tumor vascularization and physiology in such a way that makes drug delivery challenging in these PDX models. 20
The authors' observation of slower tumor growth in PDX models is indicative of this. However, robust uptake in UW-13 challenges this notion and suggests that affinity for CLR1404 may vary depending on individual cancer strain morphology independent of the nominal in vivo behavior of PDX models. Variability in morphology and targeting across cancer cell lines of a common disease site is expected and was a key factor in the use of 12 different HNC tumor models for this work. 30 These observations suggest that pretherapy confirmation of uptake would be beneficial in screening patients for iopofosine I-131 RPT. It is also worth noting that the two HPV+ models, UW-1 and UW-36, exhibited the lowest uptake. Although far from conclusive, these results indicate that the impact of HPV status on CLR1404 targeting of HNC cancer should be further investigated.
The challenge of imaging 124I with quantitative accuracy has long been an issue in nuclear medicine and is becoming increasingly important to address with the resurgence of theranostics. 31,32 In this work, considerable PVEs were observed in quantitative in vivo uptake measurements of CLR 124 such that the concentration of 124I activity was systematically underreported and that this bias grew increasingly large for small tumors. Employing a novel preclinical hot-sphere phantom, the authors found that the application of RC factors, as a function of measured spherical tumor volume, significantly improved the accuracy of in vivo quantification of CLR 124.
These results match up well with the observations of Knowles et al, 33 who investigated 124I-A11 in prostate cancer and similarly assessed the accuracy of in vivo uptake measures with PVC using ex vivo biodistribution data acquired immediately following imaging. Notably, Knowles et al utilized background subtraction before application of PVC using an ROI encompassing nonspecific tissue near the tumor. While this approach helps account for the assumption of a cold background that RC values are measured in, this tumor to background ratio changes with time after injection. This makes background subtraction more difficult to apply to cumulative measures such as AD, which is the primary focus of this work.
Given the improved quantification of CLR 124 uptake the authors observed with PVC, RC-based corrections were carried through to the CLR 124 PET-based theranostic tumor dosimetry for iopofosine I-131. They found that when PVC was performed, the radiation dose delivered to tumors per injected activity increased by 64%–125%. Notably, the radiation dose delivered to tumors by iopofosine I-131 RPT varied substantially between HNC models (0.89–2.25 Gy/MBq), emphasizing the importance of personalized tumor dosimetry iopofosine I-131 RPT.
However, the authors also found that tumor dose-guided delivery of iopofosine I-131 RPT achieves significantly different tumor response between models. It has largely been accepted that a Gy of XRT is not biologically equivalent to a Gy of RPT, but the work presented in this study further demonstrates that the tumoricidal capacity of a Gy of iopofosine I-131 RPT can vary between HNC cell lines as well. They determined that for SCC-2 tumors, 13.1 Gy from iopofosine I-131 will produce a similar response to 6 Gy of XRT, which is not true for Tu-138 tumors, where a Gy of iopofosine I-131 achieves less relative effectiveness than XRT.
While target receptor saturation is a concern for some molecularly targeted agents, APC analogs such as CLR1404 show little to no saturability effect on tumor uptake. 34 As such, variability in tumor response to iopofosine I-131 is expected to be due to differences in uptake and radiobiological characteristics of each model. In this study, a slightly higher α/β value for SCC-2 (1.99 Gy) compared to Tu-138 (2.58 Gy) indicates that a higher biologically effective dose delivered to SCC-2 may explain difference in response. This provides further evidence that, when it comes to dosimetry, radiobiological factors need to be accounted for to fully understand and leverage the prognostic power of radiation dosimetry. 35
There are a few notable limitations of this work. While the application of RC-based PVC for in vivo CLR 124 uptake was validated with direct ex vivo biodistribution measurements, the correction holds only for region-level metrics such as mean AD. The approach assumes uniform uptake within the target volume. This is often not the case in larger tumors with spatially heterogeneous or concentrated manifestation of hypoxia. Furthermore, using region-based PVC to arrive at more accurate mean dose metrics curtails much of the valuable information that can be gleaned from the personalized voxel-level dosimetry approach employed in this work. Given the importance of voxel-level dosimetry in clinically relevant radiobiological factors, the translational potential of this PVC approach is limited to small lesions. Another limitation of this work lies in the variability in tumor size in preclinical imaging and therapy studies.
The incorporation of volume-based PVC reduced the impact of this variability on uptake and dosimetry analysis. For therapy studies, however, a considerable range in initial tumor volumes (72–1360 mm3) introduced uncertainty to this response analysis. In the statistical analysis, this manifested as a high degree of within-group heterogeneity in the longitudinal growth models, which proved challenging for the many internal optimization algorithms used in the fitting of hierarchical statistical models. However, this variability in tumor size is often observed in preclinical studies and efforts to reduce this would require preparation of a prohibitively large number of mice per experiment.
Conclusions
The work presented herein establishes that CLR 124 and iopofosine I-131 demonstrate tumor-specific uptake and durable retention in a broad spectrum of HNC xenograft models. PVEs significantly impact quantitative PET imaging of CLR 124 in tumors and the methodology validated in this study for incorporating PVC in dosimetry should be considered in future theranostic applications of CLR 124 and iopofosine I-131. The tumor dosimetry-driven response studies presented here suggest that iopofosine I-131 has the capacity to deliver increasingly tumoricidal doses to HNC tumors and that careful consideration of radiobiological factors should be made when considered in the context of conventional XRT. Given that both iopofosine I-131 and XRT alone show evidence of tumor response in HNC, combination XRT-RPT should be further explored to assess whether apparently additive or synergistic effects may be realized, allowing for dose modifications that would reduce the local or systemic toxicity of either treatment.
Footnotes
Acknowledgments
The authors would like to thank the University of Wisconsin Small Animal Imaging and Radiotherapy Facility and The Ride (Madison, WI) for supporting this work.
Authors' Contributions
I.R.M.: formal analysis; investigation; software; visualization; and writing—original draft. C.L.: formal analysis; investigation; resources; and writing—review and editing. J.G.: data curation; methodology; validation; and writing—review and editing. J.J.: data curation and resources. C.L.: formal analysis; software; visualization; and writing—review and editing. D.P.A.: validation. R.H.: resources. J.P.W.: resources and supervision. P.M.H.: conceptualization; funding acquisition; methodology; project administration; supervision; and writing—review and editing. B.P.B.: funding acquisition; methodology; supervision; and writing—review and editing.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Disclosure Statement
J.P.W. was cofounder of Cellectar Biosciences and J.J. is a cofounder of Phantech.
Funding Information
The authors would like to acknowledge the Cancer Center Support Grant National Cancer Institute (NCI) P30 CA014520. Research reported in this publication was supported by the NCI of the NIH under award no. T32CA009206 and the Specialized Program of Research Excellence (SPORE) program, through the NIH National Institute for Dental and Craniofacial Research and NCI grant P50DE026787.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.