
Abstract
A 73-year-old female patient, affected by mycosis fungoides (MF), discontinued mogamulizumab, after initial clinical benefit, due to the onset of generalized erythema. Follow-up positron emission computed tomography (PET/CTs) carried out at 3 weeks and 6 months after therapy discontinuation showed, with respect to baseline PET/CT scan, a progressively increasing number of hypermetabolic enlarged lymph nodes suspected for a neoplastic involvement, but with histology indicative of an inflammatory reaction. After sequential therapy with corticosteroids and methotrexate, a complete remission was registered at 18F-fluorodeoxyglucose ([18F]FDG) PET/CT performed at 12 months after mogamulizumab interruption. The case we describe highlights the usefulness of serial examinations with [18F]FDG PET/CT in an MF patient presenting an unusual adverse reaction to mogamulizumab.
Introduction
Mogamulizumab, a humanized IgG1 monoclonal antibody targeting chemokine receptor 4 (CCR4), has been recently approved for the treatment of therapy-refractory mycosis fungoides (MF) by the Food and Drug Administration, European Medicines Agency, and Agenzia Italiana del Farmaco. In phase III MAVORIC study, patients treated with mogamulizumab exhibited higher response rate and durability with respect to those submitted to vorinostat. 1
However, mogamulizumab by removing CCR4-positive malignant cells leads to an imbalance among CCR4-positive regulatory and effector normal T cells and increases the risk of autoimmune disease. Furthermore, it has to be underlined that several adverse events (AEs) have reported during mogamulizumab therapy, such as lymphopenia, infusion reaction, fever, and cutaneous rash. 2 In this scenario, there is an unmet need of imaging biomarkers suitable for monitoring MF response to mogamulizumab.
Positron emission computed tomography (PET/CT) with 18F-fluorodeoxyglucose ([18F]FDG) is a well-established imaging modality for staging and follow-up in oncology, but its role for the imaging in MF patients during mogamulizumab immunotherapy has to be investigated yet.
Herein the authors report [18F]FDG PET/CT's findings in an MF patient showing an unusual reaction to mogamulizumab immunotherapy.
Case Presentation
Case report
In 2021, a 73-year-old female patient with a clinical history of MF refractory to topical and systemic therapies was referred to our center. In 2012, she presented alopecia areata of the scalp, diagnosed as lichen planopilaris, treated with topical steroids for 2 years with mild clinical benefit. Three years later, the patient presented an itchy erythemato-squamous circular lesion in the left arm, also poorly responsive to empirical topical steroid therapy. In 2020, due to the progressive extension of the cutaneous lesion, a biopsy was performed.
Histology showed an epidermotropic dermal infiltrate mainly constituted of small–medium CD4+ T cell, and the diagnosis of MF was formulated. Staging according to The European Organization for Research and Treatment of Cancer (EORTC) resulted in TNMB IIA. The patient was treated with Ultraviolet Light B phototherapy without benefit and only a thickening of the lesions was observed (no biopsy was performed). It was not possible to treat the patient with interferon and bexarotene because there was no possibility to prescribe them in our hospital.
In May 2021, the patient presented a progressive disease with an additional tumor lesion ≥1 cm in diameter: the staging according EORTC resulted in TNMB IIB. The patient was also studied with an [18F]FDG PET/CT scan (Fig. 1): PET/CT was performed 60 min after the intravenous administration of 3.7 MBq/kg of [18F]FDG on a digital Biograph Vision PET/CT system (Siemens Healthcare; Erlangen, Germany) with an axial FOV of 197 mm using continuous bed motion with a bed speed of 1.5 mm/s (equivalent to 90 s per bed position).

Reconstruction was conducted with a TrueX+TOF algorithm and Gauss filtered to a transaxial resolution of 2 mm at full width at half maximum. Attenuation correction was carried out using the low-dose nonenhanced CT data. PET/CT showed increased tracer incorporation in the cutaneous lesions of the left arm, with a maximum standardized uptake value (SUVmax) of 4.8 and in the ipsilateral axillary lymph nodes (SUVmax of 6.7), these last findings suspected for pathological localization. To solve differential diagnosis, an ultrasonography (US) was subsequently carried out: enlarged reactive axillary lymph nodes with no evidence of pathological alterations were found.
In June 2021, the patient started the therapy with mogamulizumab according to standard international schedule. 3 In the following weeks, clinical examination demonstrated a progressive regression of the squamous lesion in the left arm. Nevertheless, after an overall number of eight administrations of mogamulizumab therapy a generalized erythema associated with folliculitis and alopecia was registered, while laboratory examination showed low platelets' (plt) count (i.e., 75,000 plt/μL).
To discriminate between disease progression and generalized adverse reaction to mogamulizumab, an incisional biopsy of the left flank was performed and histological examination resulted positive for spongiotic dermatitis. Furthermore, peripheral blood smear was negative for neoplastic cells. A diagnosis of mogamulizumab-AE was postulated, and therapy was promptly discontinued.
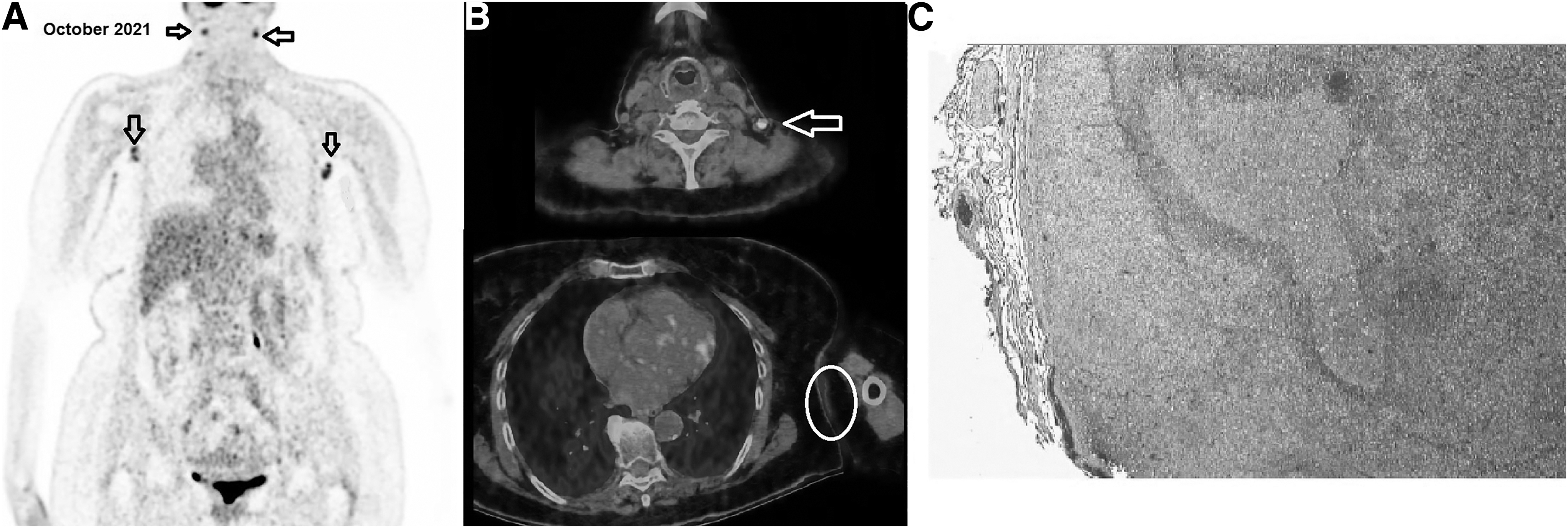
A further PET/CT scan, carried out in October 2021 at 3 weeks after mogamulizumab discontinuation, demonstrated, despite skin lesion's response, meaningfully increased [18F]FDG incorporation into neck, axillary, and inguinal lymph nodes, with an overall pattern interpreted as progressive metabolic disease according to PET Response Evaluation Criteria for Immunotherapy (PERCIMT) (Fig. 2). Therefore, a PET-guided biopsy of a left neck node was performed, and histology depicted the lymph node with an expanded paracortical area, as for reactive phenomena (Fig. 2C). Therefore, the patient started corticosteroid therapy with prednisone (50 mg/day) and was submitted to periodic monitoring through clinical and laboratory examinations.
Three months later, the patient presented an almost complete resolution of the generalized erythema and alopecia, although a moderate enlargement of axillary lymph nodes was detected. The regions' US examination described reactive isolated hyperplastic nodes, characterized by preserved morphology with the largest node measuring 29 mm in maximum diameter.
Six months after mogamulizumab discontinuation, the patient underwent a follow-up [18F]FDG PET/CT (Fig. 3A) that revealed an increased number of hypermetabolic enlarged lymph nodes with bilateral localizations to neck, supraclavicular, axillary, iliac (i.e., common, internal, and external), and inguinal nodes (SUVmax 9.7), as shown in Figure 3A and B. A further PET-guided biopsy of the target node in the right nuchal region was carried out and histology further excluded progression.
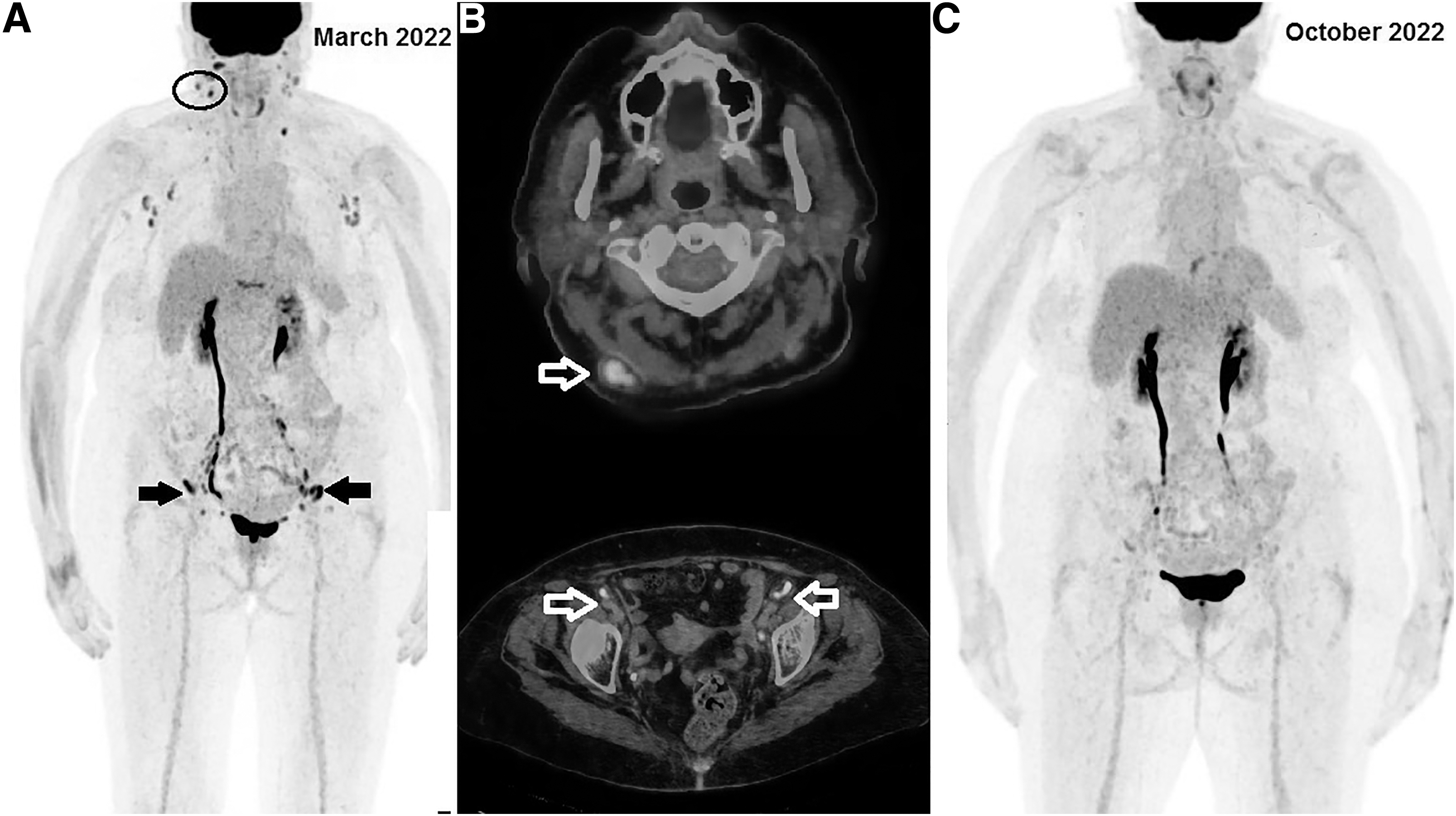
Subsequently she was submitted to methotrexate 15 mg once weekly from April to September 2022. At last follow-up (October 2022), she had no clinical evidence of disease and underwent the fourth PET/CT scan that demonstrated complete regression of all the previously documented hypermetabolic nodes (Fig. 3C).
Discussion
Nuclear medicine offers the unique opportunity of investigating pathological processes at a cellular and molecular level through radiopharmaceuticals emitting energy suitable for imaging through SPECT or PET technology. 4,5
[18F]FDG represents the most commonly employed tracer in oncology, since tumor cells use glycolysis as a preferential source for producing energy necessary for growth and proliferation. Nevertheless, it lacks specificity since activated inflammatory cells also overexpress glucose transporters and, therefore, internalize [18F]FDG, which can be used, in fact, as a biomarker both of oncological and inflammatory conditions.
Scientific data on [18F]FDG PET/CT for staging and monitoring MF during therapies are extremely limited. In this regard, Tsai et al. employed [18F]FDG PET/CT for staging 13 patients affected by MF and Sézary syndrome at high risk of nodal involvement: the authors reported that PET/CT showed a higher sensitivity than CT alone for nodal involvement detection, with a correlation among tracer's uptake (SUV) and histological grading. 6 In a retrospective study on a large cohort, Feeney et al. found that among 122 patients 55 had cutaneous involvement, whereas 95 had hypermetabolic lymphadenopathy, and 54 had FDG-avid extranodal disease. 7
In this respect, it is worth mentioning the recently published Italian consensus-based position article on cutaneous T cell lymphomas: [18F]FDG PET/CT is recommended as imaging modality for patients' staging, since it was found to show a sensitivity of 82% and 80% for the detection of cutaneous and extracutaneous disease, respectively. Furthermore, in case of nodal involvement, [18F]FDG PET/CT resulted useful for identifying the most appropriate peripheral node to be biopsied on the basis of SUV value. 8
It has to be underlined that the use of [18F]FDG PET/CT in early-stage MF is still up for debate, since cutaneous lesions might show low or absent FDG-avidity. However, an accurate evaluation of cutaneous extension and the eventually involved lymph nodes is of crucial importance for MF patients' prognostic stratification. In the case we report, we decided to carry out a PET/CT scan after a multidisciplinary discussion, taking into account the results of the PROCLIPI international Study showing that PET/CT detected pathological nodal involvement in 18% of early-stage MF subjects, some of whom not exhibiting enlarged nodes at physical examination. 9 In addition, we assumed that a baseline [18F]FDG PET/CT scan would have been of value to assess the response to mogamulizumab therapy.
To the best of our knowledge, our report is the first one highlighting the usefulness of serial [18F]FDG PET/CT scans for the imaging of a sustained inflammatory reaction to mogamulizumab in an MF patient. In a recently published systematic review analyzing 14 published studies, in patients undergoing mogamulizumab monotherapy the most common all-grade AEs were lymphopenia, infusion reaction, fever, rash and chills, whereas the most common grade ≥3 AEs were lymphopenia, neutropenia, and rash. 2 To date, in literature there are no cases describing histopathological changes affecting the lymph nodes after treatment.
Some authors have documented the histopathological modifications of the paracortical cell subpopulations in the dermopathic lymph nodes associated with MF. 10 We have hypothesized that, in our patient, the use of CCR4-targeted immunotherapy might have determined an imbalance between regulatory and effector T cells leading to an inflammatory cascade, subsequently blocked by corticosteroids and methotrexate. However, it has to be highlighted that we cannot exclude that the use of methotrexate might have determined a complete remission of an eventually residual disease.
Owing to the atypical presentation of the AE described in our patient, interpretation of PET/CT scans was challenging, since progressive nodal involvement was suspected; however, it has to be underlined that functional imaging resulted useful not only to disclose patient's reaction to drug but also for its monitoring after therapy discontinuation. Of note, there is no consensus on what criteria should be applied for PET interpretation during immunosuppressive regimens. This issue should represent a topic of future investigations.
In conclusion, [18F]FDG PET/CT might represent a useful tool for the imaging of MF patient during immunotherapy, but its applications could be hampered by the lack of specificity. In this perspective, it has been recently synthesized a radiopharmaceutical specifically targeting chemokine receptor CXCR4, namely 68Ga-pentixafor, 11 which has been applied with promising results in preliminary clinical studies on patients with MF, and might have a role for patients' stratification and follow-up during CCR4-directed therapies.
Footnotes
Authors' Contributions
L.F. and I.P. drafted the article; C.P. administered the therapy and followed up the patient; L.F. and O.B. carried out PET/CT scans and analyzed images; S.A., F.F., and V.P. performed histological examination; M.C. provided hematological consultancy; M.C. and O.S. critically revised the article for important intellectual content. All the authors have approved the final version of this article
Ethical Approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from the patient.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.