
Abstract
In the past decade, the implementation of immunotherapy with checkpoint inhibitors has determined a major change in the management of oncological patients. The challenges associated to the new therapeutic regimen have promoted adapted criteria for response assessment to interpret imaging findings and atypical patterns of response. Parallel to the new morphological criteria, also 18fluoro-deoxyglucose positron emission/computed tomography imaging has required novel approaches and specific guidelines on how to perform, interpret, and report the scan in patients with solid tumors under immune checkpoint inhibitors therapy. A summary of the novelties related to the new joint international European Association of Nuclear Medicine (EANM)/Society of Nuclear Medicine and Molecular Imaging (SNMMI)/Australian and New Zealand Society of Nuclear Medicine (ANZSNM) guidelines on immunotherapy is provided herein to elucidate most critical aspects in image interpretation.
Introduction
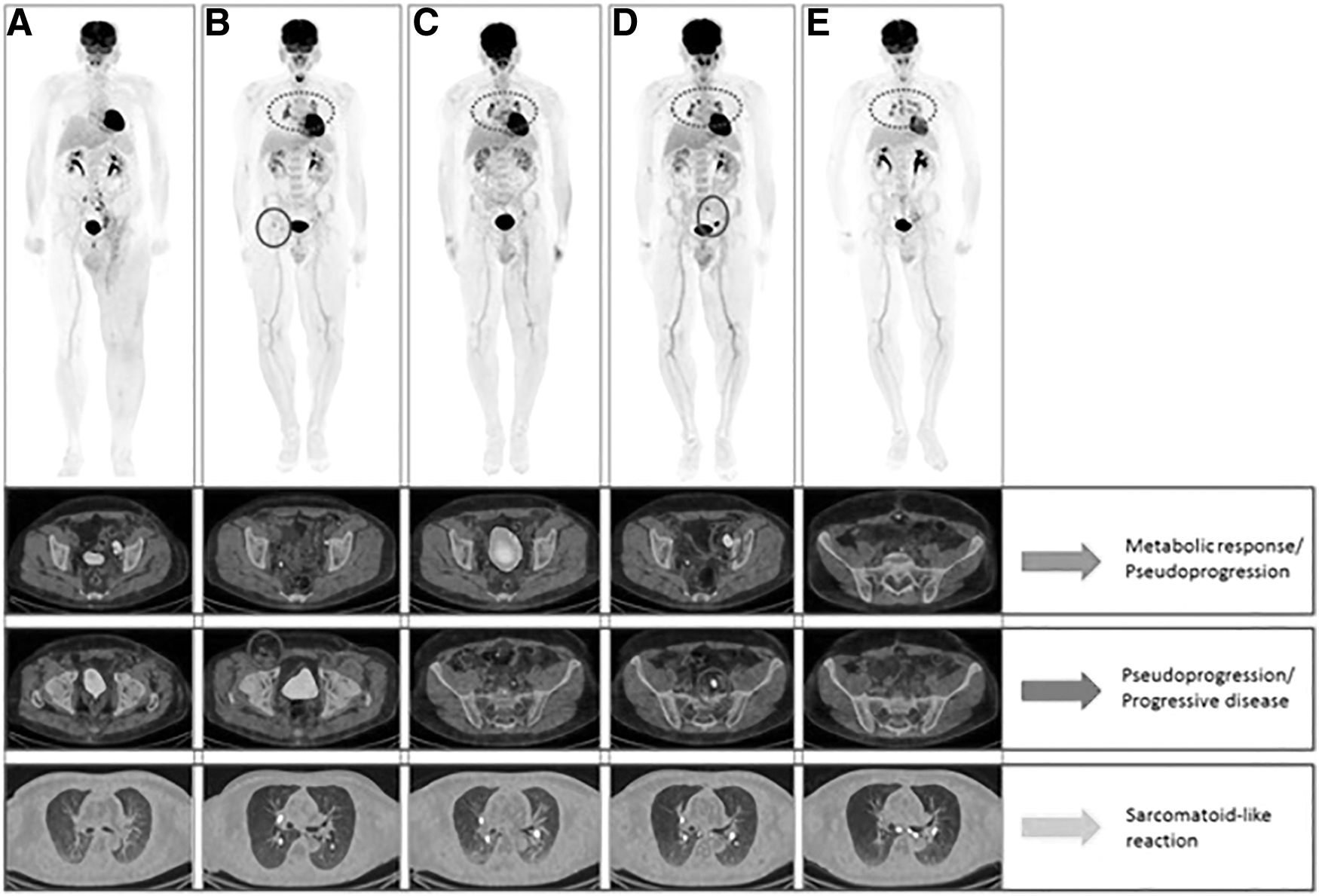
In the past decade, a large number of publications, predominantly single-centered, have investigated 18fluoro-deoxyglucose ([18F]FDG) positron emission tomography/computed tomography (PET/CT) in cancer patients undergoing treatment with immune checkpoint inhibitors. 1,2 The challenges associated to this new therapeutic regimen have promoted adapted criteria for response assessment to interpret imaging findings and atypical patterns of response (Fig. 1). Parallel to the new criteria applied for morphological imaging (i.e., modified Response Evaluation Criteria in Solid Tumors for immune-based therapeutics [iRECIST], immune-modified Response Evaluation Criteria in Solid Tumors [imRECIST]), 3,4 also [18F]FDG PET/CT imaging has required novel approaches and specific guidelines on how to perform, interpret, and report the scan in patients with solid tumors undergoing immune checkpoint inhibitors therapy.

Illustration of four specific patterns of response to immunotherapy:
Earlier this year, the “Joint EANM/SNMMI/ANZSNM practice guidelines/procedure standards on recommended use of [18F]FDG PET/CT imaging during immunomodulatory treatments in patients with solid tumors version 1.0” have been published. 1 The steering committee of the aforementioned guidelines included international experts from all over the world, aiming to shed light on the appropriate indications and recommendations on [18F]FDG PET/CT use in the era of immunotherapy, with a special focus on response assessment in solid tumors.
Based on these criteria, three different time points are reported as indicated.
TIME POINT 1: Baseline Evaluation Before Treatment Start
PET/CT is regarded as mandatory in all [18F]FDG avid tumors before treatment start with immunotherapeutic regimens. The scan serves as a staging/restaging tool, depending on the line of treatment, and defines a time zero (T0) assessment useful for subsequent monitoring.
TIME POINT 2: Assessment During the Course of the Treatment
The first response assessment with [18F]FDG PET/CT is recommended 8–12 weeks after treatment start (i.e., 3–4 cycles). Given the prevailing use in this context of morphological evaluation with CT, PET/CT should be performed routinely in case of discordant findings and in nonresponding patients, to complement the information obtained from CT. Earlier or later assessment is recommended in case of clinical deterioration and/or suspicious progression on contrast-enhanced CT. 1
The guideline highlights the use of appropriate reporting of metabolic response to treatment (Fig. 2), by providing as optional the available response criteria in solid tumors (i.e., European Organisation for Research and Treatment of Cancer [EORTC] and PET Response Criteria in Solid Tumors [PERCIST]), as well as the new immunotherapy-adapted metabolic criteria (i.e., PET/CT Criteria for Early Prediction of Response to Immune Checkpoint Inhibitor Therapy [PECRIT], PET Response Evaluation Criteria for Immunotherapy [PERCIMT], immune PET Response Criteria in Solid Tumors (iPERCIST), and immunotherapy-modified PERCIST [imPERCIST]). 5 –10
Interpretation of [18F]FDG PET/CT findings in a patient with metastatic melanoma treated with nivolumab. From baseline images
TIME POINT 3: Assessment Before Immunotherapy Discontinuation or Treatment Stop
Patients receiving maintenance therapy or undergoing long-term treatment with checkpoint inhibitors would benefit from metabolic assessment of response with [18F]FDG PET/CT, particularly in partial responders or stable disease on CT. 12,13
The joint European Association of Nuclear Medicine (EANM)/Society of Nuclear Medicine and Molecular Imaging (SNMMI)/Australian and New Zealand Society of Nuclear Medicine (ANZSNM) guidelines/procedure standards support the general recommendations provided by previous EANM guidelines, 14 and SNMMI procedure standards for tumor imaging, 15 as well as the RSNA QIBA FDG/CT guidance. 16,17 In this context, given the importance of reproducible and repeatable data on [18F]FDG PET/CT imaging, international harmonizing standards, such as those based on the EANM/EARL program, 18 should be granted. This is especially true when considering semiquantitative parameters for response assessment.
Additional information for image interpretation and reporting are provided through a detailed checklist (Table 1), which should serve as guidance for [18F]FDG PET/CT imaging during immunotherapy with checkpoint inhibitors. Special attention is given with this regard to the signs of the immune activation, that is, spleen-to-liver ratio, and the occurrence of the immune-related adverse events (irAEs), which should be promptly reported, whereas more severe toxicities should be directly communicated to the referring physician or to the appropriate health care provider.
Recommended Checklist for the Assessment of Patients with Solid Tumors Undergoing Immunotherapy with Checkpoint Inhibitors
Modified from Lopci et al
1
under a Creative Commons Attribution 4.0 International License (
[18F]FDG, 18fluoro-deoxyglucose; EORTC, European Organisation for Research and Treatment of Cancer; PECRIT, PET/CT Criteria for Early Prediction of Response to Immune Checkpoint Inhibitor Therapy; PERCIMT, PET Response Evaluation Criteria for Immunotherapy; iPERCIST, immune PET Response Criteria in Solid Tumors; imPERCIST, immunotherapy-modified PERCIST; PERCIST, PET Response Criteria in Solid Tumors; PET/CT, positron emission tomography/computed tomography.
While representing up-to-date recommendations on [18F]FDG PET/CT use during immunomodulatory treatments, these guidelines are not carved in stone. Response assessment and patient management during immunotherapy remains a dynamic research field, which continuously provides new evidence and applications. Therefore, the aforementioned guidelines should serve as a starting point to clarify the role of PET/CT in this clinical scenario, which has to be furthermore validated. Particularly with respect to the use of the new radiopharmaceuticals developed for immune-PET imaging.
As for many other clinical indications in nuclear medicine, a multidisciplinary approach is important to optimally manage unexpected events and imaging challenges. In view of the complexity of new therapies and often unique patterns of response or irAEs on [18F]FDG PET/CT, it is vital that prospective clinical research and trials are conducted to establish evidence for appropriate use that can be utilized by nuclear medicine specialists and clinicians treating and managing these patients.
Footnotes
Acknowledgments
The authors would like to thank all original contributors of the joint EANM/SNMMI/ANZSNM guidelines 1 for their precious collaboration: Nicolas Aide, Rodney J. Hicks, Antonia Dimitrakopoulou-Strauss, Laurent Dercle, Amir Iravani, Romain D. Seban, Christos Sachpekidis, Olivier Humbert, Olivier Gheysens, Andor W.J.M. Glaudemans, Wolfgang Weber, Richard Wahl, Andrew M. Scott, and Neeta Pandit-Taskar.
Disclosure Statement
E.L. reports receiving grants from Fondazione AIRC (Associazione Italiana per la Ricerca sul Cancro) and from the Italian Ministry of Health, and faculty remuneration from ESMIT (European School of Multimodality Imaging and Therapy) and MI&T congressi. A.C. reports previous fellowships from Fondazione AIRC. L.F. declares no conflict of interest.
Funding Information
No funding was received for this article.