
Abstract
Background:
The comprehensive treatment mode of combining concurrent chemoradiotherapy (CCRT) with adjuvant chemotherapy (AC) is a commonly used mainstream model in the clinical practice of locally advanced cervical cancer (LACC). However, the necessity for AC after CCRT lacks sufficient evidence-based medical support. This study constructs a predictive model for the survival time dependence of CCRT ± AC for LACC based on the 2018 International Federation of Gynecology and Obstetrics (FIGO) staging with internal validation, the prognosis was assessed with intensity-modulated radiotherapy (IMRT) and concurrent cisplatin, and provides guidance for future stratified treatment.
Materials and Methods:
The retrospective analysis included 482 patients with LACC who CCRT from January 2016 to January 2023. Patients who used the 2009 FIGO staging were all standardized for the 2018 FIGO staging. The 482 patients with LACC were divided into a training set (n = 290) and a validation set (n = 192) at a ratio of 6:4. COX multivariate regression model and LASSO regression were used to screen for independent prognostic factors affecting progression-free survival (PFS) and overall survival (OS), and a nomogram clinical prediction model was constructed based on these factors. Evaluate the effectiveness of the model through the receiver operating characteristic curve, calibration curve, decision curve, risk heat map, and survival curves for risk stratification.
Results:
The PFS and OS independent prognostic risk factors affecting the 2018 FIGO staging of LACC during CCRT were validated to be similar to the 2009 FIGO staging prediction model reported in previous literature. In the training cohort, area under the curve (AUC) values at 1, 3, and 5 years were 0.941, 0.882, and 0.885 for PFS, and 0.946, 0.946, and 0.969 for OS, respectively. When applied to a test cohort, the model also showed accurate prediction result (AUC at 1, 3, and 5 years were 0.869, 0.891, and 0.899 for PFS, and 0.891, 0.941 and 0.878 for OS, respectively). Subgroup analysis suggests that patients with LACC, adenocarcinoma, stage IVA, pelvic lymph node metastasis, pretreatment hemoglobin ≤100 g/l and residual tumor diameter >2 cm, who received CCRT in the 2018 FIGO stage, may benefit more from adjuvant chemtherapy.
Conclusions:
Based on the 2018 FIGO staging, a nomogram prediction model for PFS and OS in patients with LACC undergoing CCRT was developed. The model, established by combining weighted clinical and pathological factors, can provide more personalized treatment predictions in clinical practice. For patients with high-risk factors such as residual tumor diameter > 2 cm after CCRT for LACC, AC may bring benefits.
Background
Cervical cancer, a prevalent malignancy among females, ranks fourth globally in terms of both incidence and mortality rates. 1 China alone contributes significantly to this global burden, reporting 111,000 new cervical cancer cases annually, with an incidence rate of 6.25%, accounting for one-third of the global incidence. 2
According to the 2018 FIGO staging, stages IB3, IIA2, and IIB-IVA are classified as locally advanced cervical cancer (LACC). The standard treatment mode for LACC is radical radiotherapy combined with concurrent chemotherapy (CCRT), but approximately 30%–40% of LACC patients experience recurrence. 3 The 5-year progression-free survival (PFS) rate is 58%, 4,5 indicating that a significant number of patients remain uncured. Hence, there persists a need for further refinement and enhancement of the existing treatment approach to ameliorate outcomes and survival prospects for those with progressing disease. For LACC, adjuvant chemotherapy (AC) after CCRT emerges as an alternative treatment option, 6 –9 although its role remains controversial. 10,11 A phase III open randomized controlled study has demonstrated that supplemental chemotherapy following CCRT can significantly improve the 3-year PFS and 3-year overall survival (OS) rates compared to utilizing only CCRT. 6 In addition, a study conducted by Guler Yavas and colleagues from Japan revealed that AC can also simultaneously reduce instances of local recurrence and distant metastasis rates, without escalating severe restrictive toxic reactions. 7 However, The South American phase III randomized controlled trials employed a dual-drug combination regimen during CCRT, which to some extent, escalated toxicity levels, lowered treatment completion rates, and negatively impacted patient quality of life. 6 It is crucial to note that most supportive results for AC are derived from retrospective studies with small sample sizes. Nevertheless, recent analyses from the OUTBACK Trial 10 and Mata in 202211 suggest that AC may not contribute to the survival benefit of patients with LACC. Developing a prognostic model and conducting a stratified analysis can enable physicians to accurately assess patient risks, identify optimal treatment cohorts, facilitate personalized care, and enhance disease monitoring and management. Consequently, identifying high-risk populations within the same stage demographic and customizing follow-up treatments through CCRT for these high-risk cohorts may present a promising clinical strategy. At present, there are many clinical prognostic models for LACC undergoing CCRT, but most of these models are based on the 2009 FIGO staging 12 –14 and lack rigorous external or internal validation, 13 –15 which limits their utility in clinical settings.
The study retrospectively analyzed prognostic factors for LACC patients treated with CCRT, following or not AC basing on the 2018 FIGO staging. The authors constructed a clinical nomogram prognostic model and performed subgroup stratified analysis of relevant prognostic factors to explore the optimal approach for comprehensive LACC treatment, focusing on identifying potential beneficiaries of AC treatment in LACC. In addition, according to incorporate 2018 FIGO staging, they refined prognostic models and offer a more updated and reliable foundation.
Methods
Research subjects
The authors conducted a retrograde analysis of the clinical data pertaining to LACC patients treated at the Fourth Affiliated Hospital of Guangxi Medical University from January 2016 to January 2023, ensuring comprehensive follow-up data. The inclusion and exclusion criteria are as follows:
Inclusion and exclusion criteria
Inclusion criteria encompassed patients diagnosed with cervical cancer through pathology. Clinical stages considered were IB2, IIA2, and IIB-IVA (2009FIGO stage), all adjusted to the 2018 FIGO stage. Furthermore,the authors included patients who had not undergone radiotherapy, chemotherapy or surgery previously. Patients were excluded if they had contraindications to radiotherapy and chemotherapy, were accompanied by primary malignant tumors in other organs, or presented with systemic infections, coagulation abnormalities, or autoimmune diseases. In addition, individuals with mental or neurological disorders that could interfere with subsequent follow-up were excluded. Those lost to follow-up due to personal reasons or with incomplete clinical data were also excluded. Ultimately, this study comprised a total of 482 patients.
Radiotherapy
Radiotherapy was applied to patients by external beam therapy (EBRT) and high-dose rate brachytherapy, maintaining consistent irradiation techniques and target areas across all groups.
External irradiation target area and dose
EBRT was administered using intensity-modulated radiation therapy (IMRT); gross tumor volume (GTV) encompassed imaging diagnosis of pelvic and para-aortic lymph node metastases. Clinical target volume (CTV) included the uterus, cervix, partial vagina (determined by the lower edge of the tumor for vaginal boundary), pelvic lymph node drainage area (the iliac common, inner and outer areas, obturator area, and sacral anterior area), and parasitic lymph node drainage area (upper boundary T10, lower edge-renal vessel level, determined by the location of abdominal aortic metastatic lymph nodes). The delineation of the lymphatic drainage area followed the 2008 Radiation Therapy Oncology Group (RTOG) expert consensus for cervical cancer radiotherapy. The prescription doses are as follows: 50.4 Gy/28f, biological equivalent dose in 2 Gy fractions (EQD2), for PCTV 49.56 Gy, and 61.60 Gy/28f for PGTVnd (EQD2 62.63 Gy, α/β = 10) (Table 1) EBRT dose plan design and treatment requirements: 6 MV X-ray, reverse intensity modulation plan design, with fixed field or volume modulation technology. The plan adhered to 100% CTV and 95% PTV coverage. During treatment, cone beam computed tomography was performed 1–2 times weekly, and IMRT was administrated five times a week over a period of 5–6 weeks. The treatment duration extended over 5–6 weeks, occurring daily from Monday to Friday. The limit of endangered organs refers to the relevant regulations of the RTOG. Limit of dose to organs at risk: Rectal V50Gy ≤ 50%; bladder V50Gy ≤ 50%; femoral head V50Gy ≤ 5%; spinal cord Dmax ≤ 45 Gy; small intestine V50Gy ≤ 10–15%; renal V20Gy ≤ 25%; and liver V30Gy ≤ 30%.
Radiation Dose and Plan Implementation for CCRT+ACT and CCRT
ACT, AC (adjuvant chemotherapy) + Treatment.
Intracavitary brachytherapy
Patients received two-dimensional (2D) intracavitary brachytherapy (ICBT) treatment before 2019 or three-dimensional (3D) combined intracavitary and interstitial brachytherapy contoured following International Commission on Radiation Units and Measurements Report 89 (ICRU89) guidelines. The total dose delivered was 36 Gy, divided into six fractions of 6 Gy each. The mean EQD2 at point A was 42.52 Gy for 2D BT in CCRT +AC group, and 42.42 Gy for 2D BT in CCRT group alone. The mean EQD2 at the high-risk CTV (HRCTV) D90 was 50.00 Gy for 3D BT in CCRT + AC group, and 50.44 Gy in CCRT group alone (Table 1). During the third week of radiotherapy, ICBT was introduced depending on each patient's response. No external radiotherapy was administered on the day of ICBT.
Chemotherapy
All patients were treated with concurrent cisplatin, 40 mg/m2 every 7 days for one cycle, with or without cisplatin-based AC. This regimen commenced on the first day of radiotherapy and continued until the completion of radiotherapy. Patients who achieved a complete response (CR) on pelvic MR imaging after CCRT with intention-to-treatment (ITT) of AC, Analysis was by intention to treat at the end of treatment cycle. Those who achieved a partial remission (PR) or no change (NC) were offered AC, unless they declined further treatment. AC commenced approximately 2–3 weeks postradiotherapy, with the schedule contingent on the patient’s recovery. Treatment could be temporarily halted in response to acute side-effects or if the patient was unable to comply. When the patient regained fitness, the treatment was resumed. In cases of severe side-effects, the treatment was suspended until the side-effects subsided, subsequently resuming with potential dose adjustments.
AC: Patients received paclitaxel at a dosage of 150 mg/m2 on day 1, and cisplatin at a dosage of 75 mg/m2 on day 1. Alternatively, carbolated area under the curve (AUC) = 5 on day 1 for the same number of cycles. Adequate hydration was provided before and after chemotherapy, with supplementary symptomatic treatments such as antiallergic, hormonal, diuretic, antiemetic, and liver and stomach protection.
Follow-up
The authors recorded the commencement and conclusion of radiotherapy, noted the fractionation dose, inquired about subjective symptoms, assessed treatment compliance, and monitored for radiotherapy complications during follow-up. The follow-up protocol included gynecological examination, blood routine, and tumor marker detection, along with imaging studies (upper and lower abdominal computed tomography [CT]/magnetic resonance imaging [MRI], pelvic MR, chest CT if necessary, and bone electrochemotherapy) to evaluate short-term and long-term efficacy. Case biopsy could be performed if necessary for disease progression. Follow-up intervals were scheduled at the end of radiotherapy, and then at 1 month, 3 months, and 5 years after treatment. The residual status of cervical tumors was determined by pelvic MRI results (tumor diameter: >2 cm; ≤2 cm) obtained during the initial re-examination at the end of follow-up treatment. Subsequently, follow-up visits were scheduled once every 3 months from the first to the third year, once every 6 months after 3 years, and once every year after 5 years. In case of any abnormality during this period, individuals were advised to seek immediate medical attention.
Statistical methods
Statistical analysis was conducted using R language (Version 4.3) statistics software. Count data and intergroup ratios were analyzed through the Chi-square test, whereas quantitative data were assessed using the t-test. Survival analysis employed the Kaplan–Meier method, and intergroup survival rate comparison was executed using the log-rank test. Prognostic factors influencing patient survival were examined through a multivariate COX regression model. The least absolute shrinkage and selection operator (LASSO) method was employed for screening and determining potential risk factors affecting prognosis. Subsequently, a nomogram clinical prediction model was constructed. The predictive performance was evaluated using a receiver operating characteristic (ROC) curve, and model accuracy and clinical applicability were assessed through calibration curves and decision curve analysis. A risk heat map and risk grouping were utilized to generate survival curves, validating the model’s effectiveness. The datasets were divided into CCRT + AC and CCRT groups based on whether AC was administered after CCRT. A forest plot was used for stratified analysis of relevant prognostic factors between the two groups, with p < 0.05 indicating a statistically significant difference. The primary observational indicators for the clinical prediction model are PFS and OS. PFS is calculated from the date of diagnosis to the date of progression or the last follow-up, whereas OS is defined as the time elapsed from treatment initiation to death or the last follow-up.
Results
Patient characteristics
In this analysis of 482 patients with LACC who underwent CCRT, less than 5% of patients (n = 22) did not complete the full course of the originally scheduled radiotherapy, which included EBRT and BT, due to toxic side-effects and personal reasons. However, the administered dose for these patients still exceeded 90% of the originally planned dose. The authors identified prognostic factors and evaluated the efficacy of AC. The median follow-up duration was 42 months (range, 8–86 months). The patient cohort was randomly divided into a training set (n = 290) and a validation set (n = 192) at a 6:4 ratio using SPSS software for model development and validation. There was no statistically significant difference in clinical and pathological data between the two patient groups (p > 0.05) (Table 2).
Basal Clinicopathologic Characteristics in Training and Validation Cohort
ACT, AC (adjuvant chemotherapy) + Treatment.
Prognostic factors
Univariate and multivariate analyses identified five independent prognostic factors that significantly influence PFS and OS in patients: Histopathology, 2018 FIGO staging, LNM, pretreatment hemoglobin levels, and residual tumor diameter after treatment. These factors were incorporated into a nomogram prediction model, demonstrating high accuracy in forecasting patient outcomes (refer to Table 3 and Table 4). LASSO pathway maps, which utilized Inlambda and LASSO regression cross-validation with a 1-standard error (s.e.) and minimum value criteria respectively for PFS and OS, show the same prognostic factor s with Univariate and multivariate analysis (using Cox regression model) (as shown in Fig. 1).

Unvariate and Multivariate Analysis of Factors in PFS
ACT, AC (adjuvant chemotherapy) + Treatment.
Unvariate and Multivariate Analysis of Factors in OS
ACT, AC (adjuvant chemotherapy) + Treatment.
A nomogram was constructed, combining the significant prognostic factors identified by both COX and LASSO models to estimate PFS and OS. The nomogram assigns points to each factor, with a total score range of 0–20 for PFS and 0–28 for OS. The corresponding survival rates on the 1-year, 3-year, and 5-year survival axes indicate that higher total scores are associated with lower survival rates (refer to Fig. 2).

Nomogram prediction model
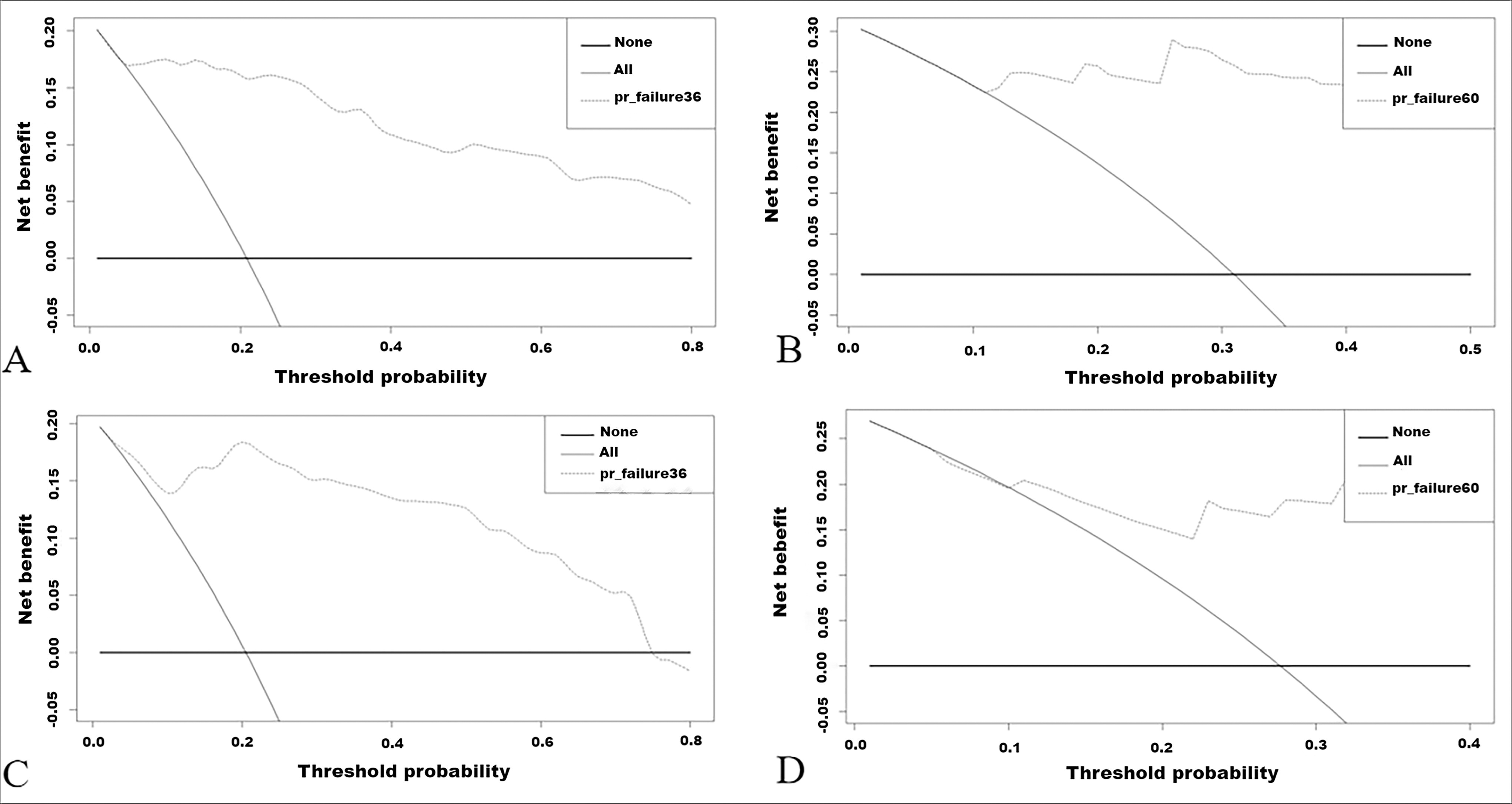
The model showed strong predictive power for PFS and OS, with PFS C-index results of 0.855 and OS C-index results of 0.839. In the training cohort, AUC at 1, 3, and 5 yrs was 0.941, 0.882, and 0.885 for PFS, and 0.946, 0.946, and 0.969 for OS, respectively. When applied to a test cohort, the model also showed accurate prediction result (AUC at 1, 3, and 5 years was 0.869, 0.891, and 0.899 for PFS, and 0.891, 0.941 and 0.878 for OS, respectively). (Fig. 3). The model’s calibration and practicality were confirmed by consistent calibration and validation curves (Figs. 4–7). Risk heat maps and survival curves further demonstrated the model’s ability to effectively differentiate between high-risk and low-risk groups (Figs. 8–11).

The receiver operating characteristic curve of the score chart for the prediction of PFS and OS at 1 year, 3 years, and 5 years of follow-up is shown in training and validation cohort. (
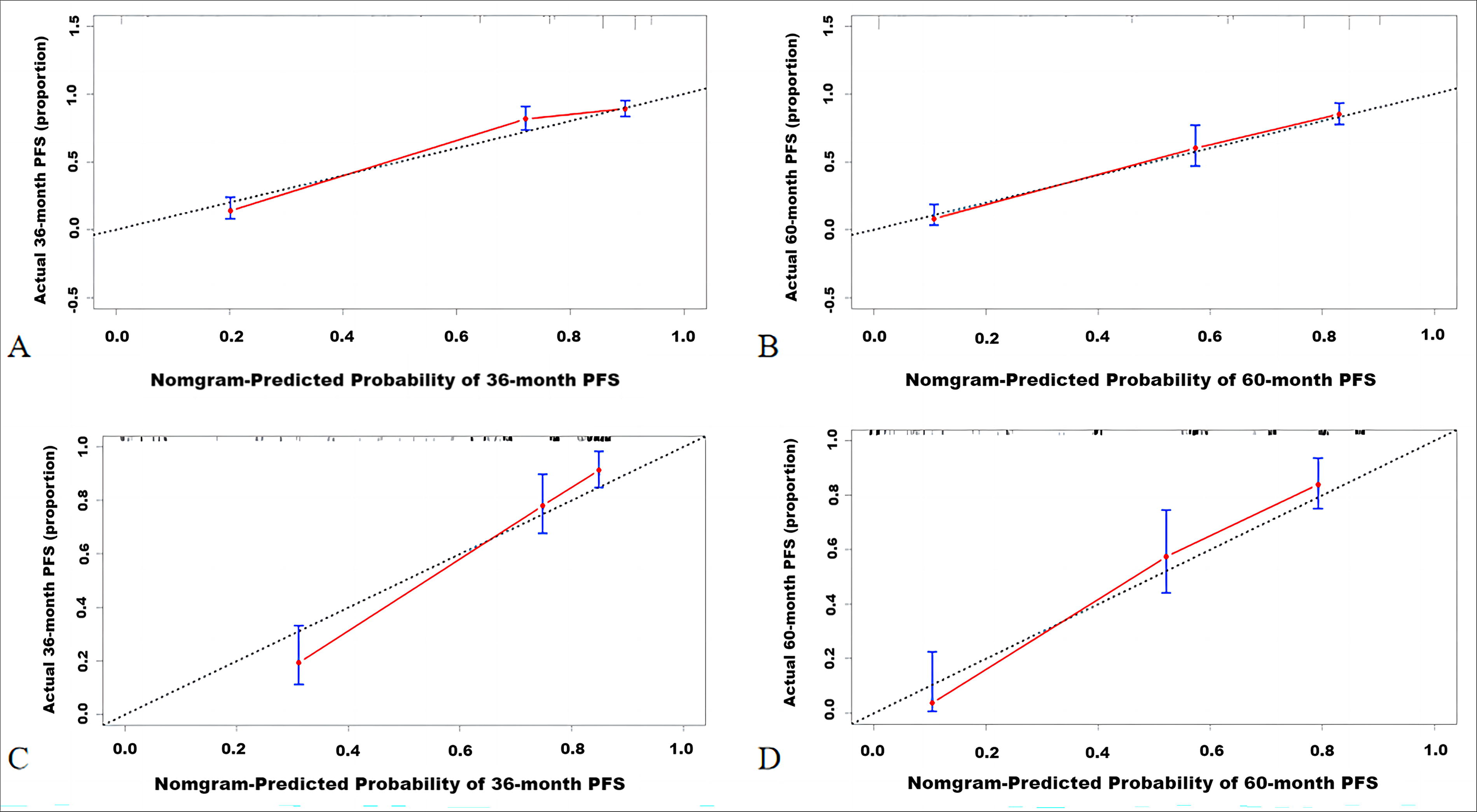
Calibration curve of PFS at 3 years and 5 years of follow-up is shown in training and validation cohort. (

Calibration curve of PFS at 3-year and 5-year follow-up is shown in training and validation cohort.

Decision curve analysis of PFS at 3-year and 5-year follow-up is shown in training and validation cohort.
Calibration curve of PFS at 3-year and 5-year follow-up is shown in training and validation cohort.

Risk heat map for PFS in training cohort. PFS, progression-free survival.
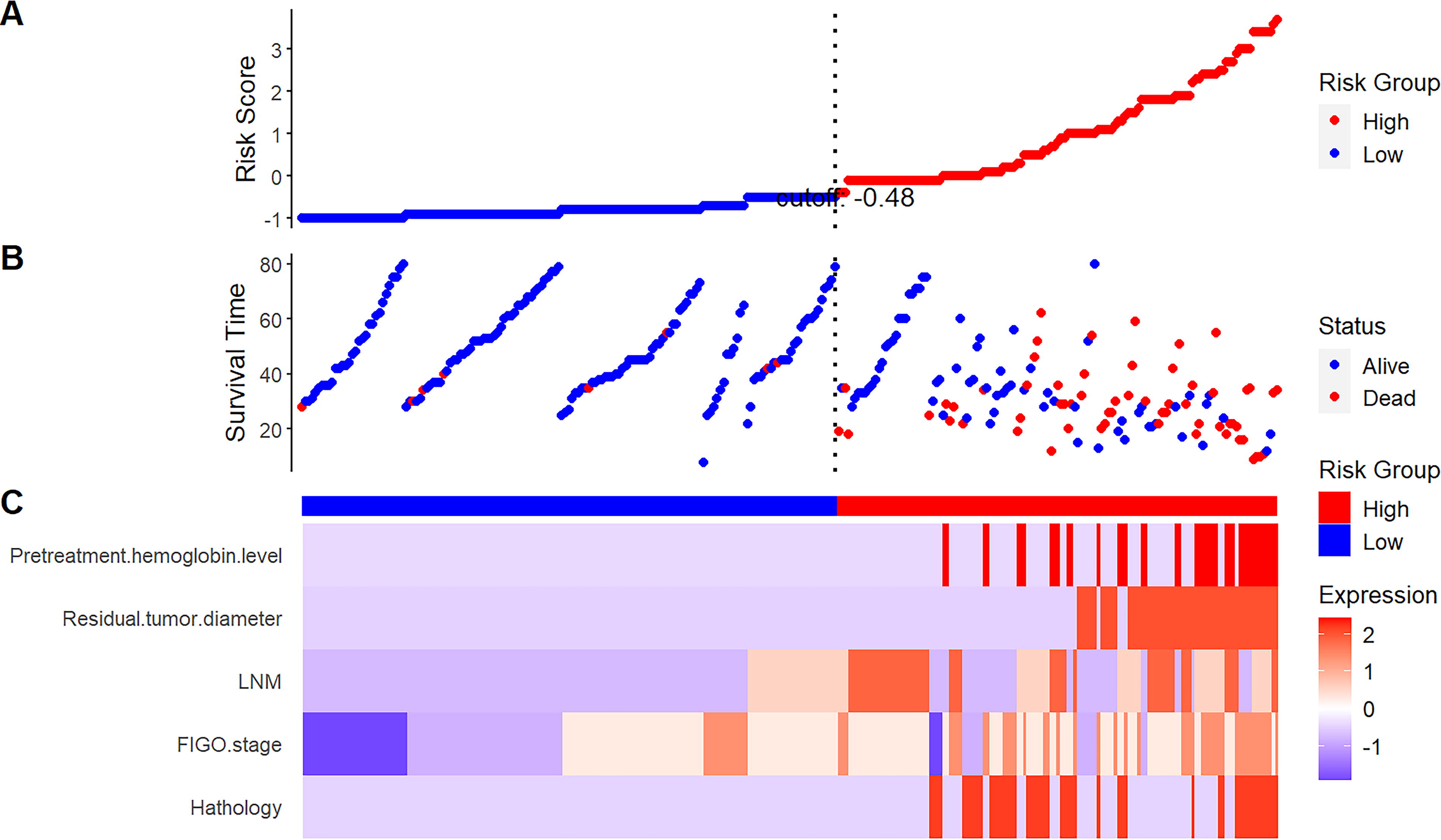
Risk heat map for OS in training cohort. OS, overall survival.
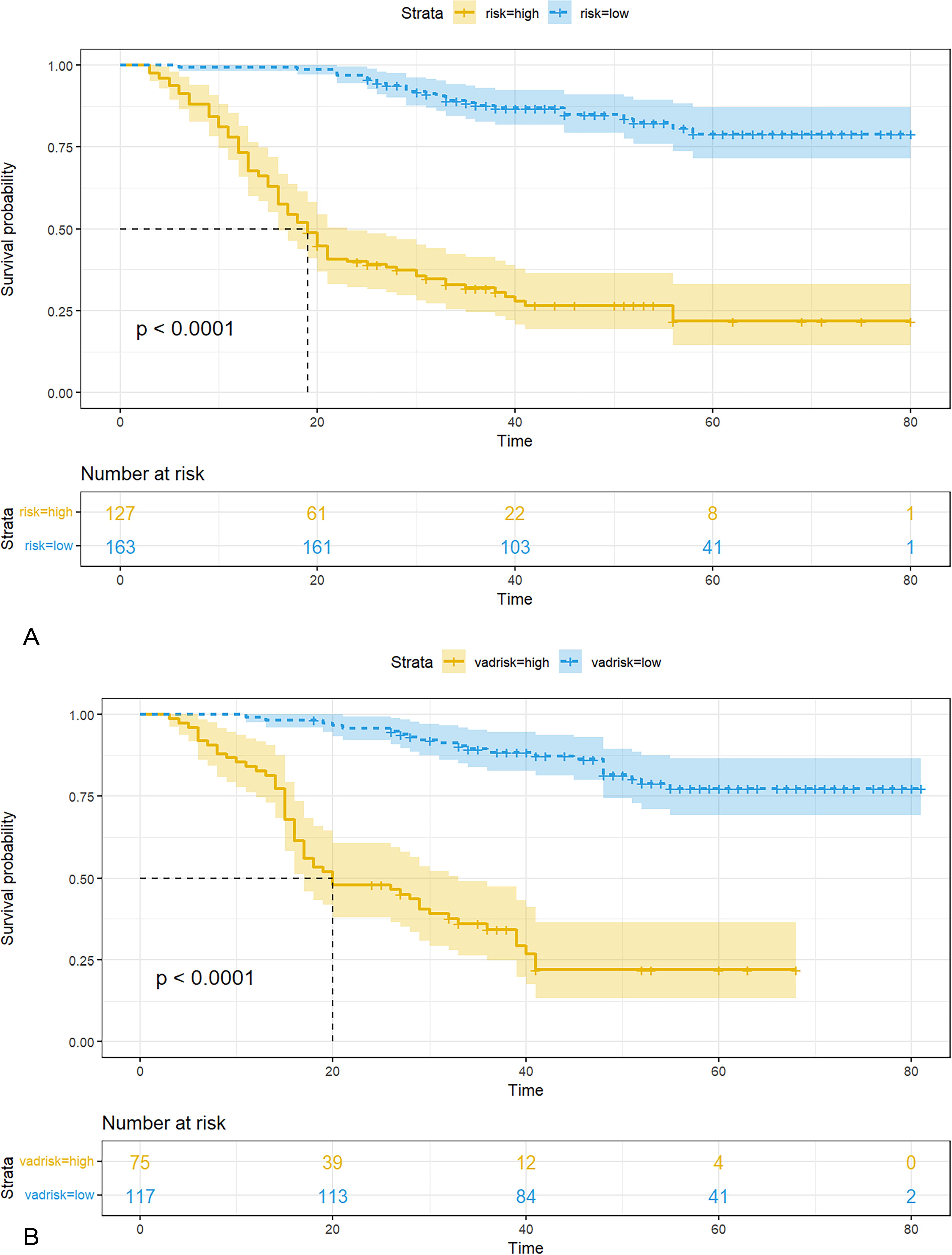
Draw a survival curve based on the median risk score of the prediction model divided into high- and low-risk groups for PFS in training and validation cohort. (
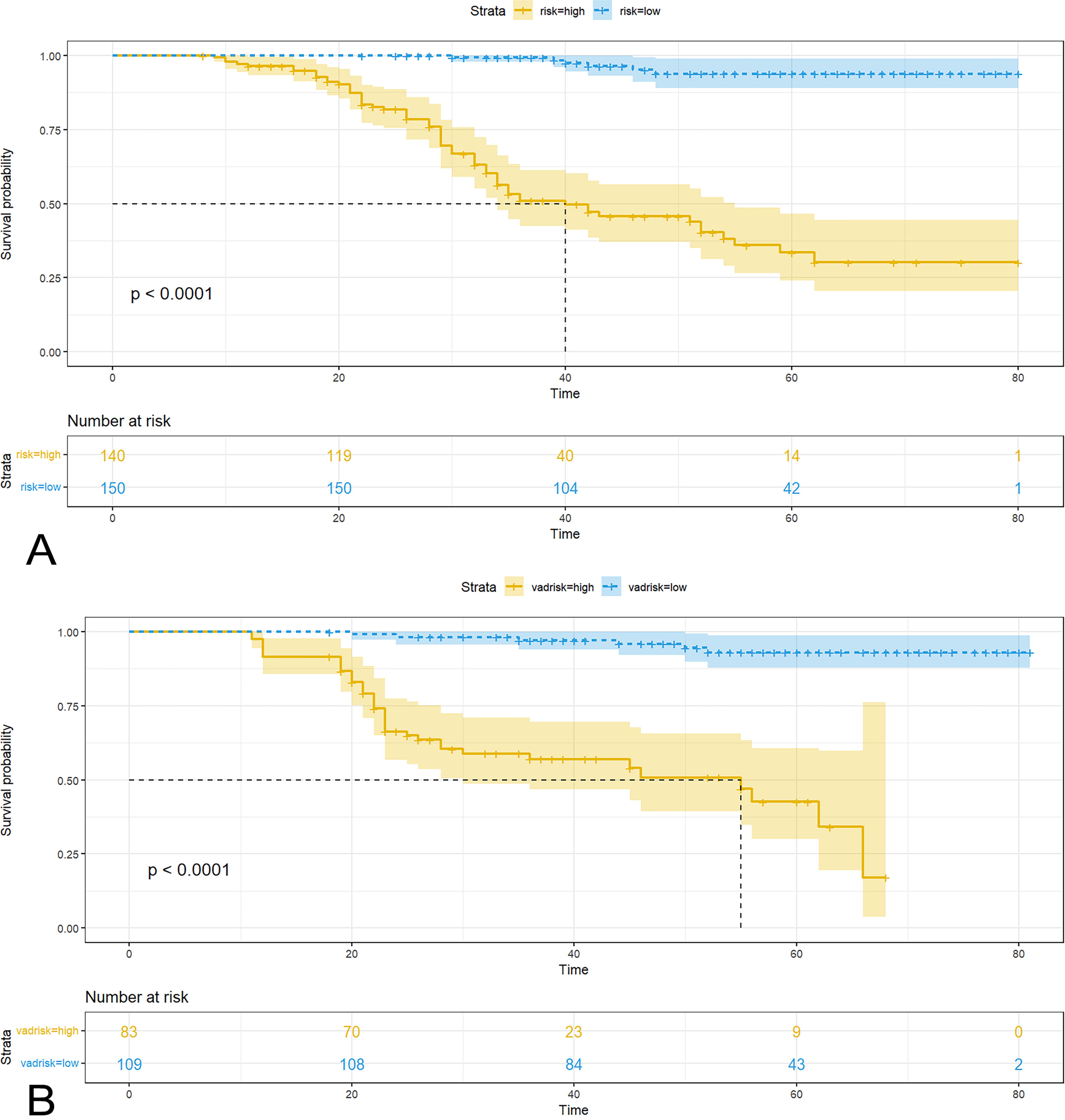
Draw a survival curve based on the median risk score of the prediction model divided into high- and low-risk groups for PFS in training and validation cohort.
AC
In the subgroup analysis, presented through a forest plot, patients with adenocarcinoma, stage IVA, pelvic lymph node metastasis (p-LNM), pretreatment hemoglobin of 100 g/l or lower, and a residual tumor diameter of larger than 2 cm significantly benefited from AC, showing improved PFS and OS (Figs. 12 and 13). Among the 227 patients who received AC, 42 patients had residual tumors >2 cm after CCRT, which may be a potentially poor prognostic factor associated with AC.

Subgroup analysis for CCRT + AC and CCRT in PFS. CCRT, concurrent chemoradiotherapy; AC, adjuvant chemotherapy; PFS, progression-free survival.

Subgroup analysis for CCRT + AC and CCRT in OS. CCRT, concurrent chemoradiotherapy; AC, adjuvant chemotherapy; OS, overall survival.
Discussion
LACC is characterized by high-risk factors, exhibits strong heterogeneity, and has a propensity for challenging local lesion control, recurrence, and metastasis. Determining the optimal treatment regimen for LACC is a subject of ongoing debate, highlighting the need for research into effective treatment models. 16,17
In this study, the authors conducted a comprehensive 7-year follow-up of LACC patients, following the 2018 FIGO staging criteria. All patients received CCRT and high-dose-rate brachytherapy; some also received AC. Using multivariate analysis with COX and LASSO regression, they identified five significant prognostic factors: pretreatment hemoglobin levels, LNM, FIGO stage, residual tumor diameter, and histological type. These factors were integrated into a nomogram prediction model, designed to estimate disease-specific mortality risks at various follow-up intervals for patients treated with definitive chemoradiotherapy, with or without AC. The dataset was randomly divided into training and validation sets, with the model showing high accuracy and an excellent goodness-of-fit. Patients were divided into low-risk and high-risk groups based on the model’s median predicted risk value, and survival curves from both sets revealed clear stratification. Internal validation confirmed the model’s robust predictive performance, underscoring its potential utility in informing clinical treatment decisions.
There are many factors that affect the prognosis of LACC patients. Previous studies 12,15,18,19 have highlighted the substantial influence of clinical staging on the survival prognosis of LACC patients. This study also indicates that the survival rate of LACC gradually decreases with the advancing stage, establishing it as an independent prognostic factor affecting survival. In cervical cancer research, LNM has been identified as a key prognostic factor influencing the survival outcomes of LACC patients. The commonly used FIGO staging system in 2009 did not consider regional lymph node status, implying that LNM did not alter the patient’s staging. After the 2018 FIGO staging revision, regardless of the primary lesion status, LNM was included in the newly added IIIC stage. Therefore, constructing the LACC prognosis model based on the revised 2018 FIGO staging is essential.
LNM serves as the primary metastatic pathway of cervical cancer, a fact supported by numerous literature studies. 12,14,15,18,19 These studies consistently affirm the close association between LNM and the survival prognosis of LACC patients, aligning with the findings of this study. In this study, the authors found that the size of tumor residue after CCRT was an independent prognostic factor affecting survival. According to literature reports, 20,21 approximately 30%−65% of patients exhibit residual imaging after receiving CCRT. Kim et al. 22 demonstrated that 71% of patients with residual tumors ≤2 cm after treatment did not exhibit disease progression during follow-up, whereas only 11% of patients with residual tumors >2 cm showed no disease progression. This suggests that a tumor residue exceeding 2 cm entails a higher risk of disease progression. While previous literature 14,23,24 primarily considered the diameter of the primary tumor as a crucial factor affecting prognosis, different studies reported varying thresholds for the tumor diameter size impacting efficacy and prognosis. 12,14,23,24 Although larger tumors are often associated with hypoxia and anemia, leading to potentially worse treatment responses, the impact on therapeutic efficacy results from the interaction of multiple factors. Ultimately, it projects the tumor’s inherent sensitivity to radiotherapy and chemotherapy, manifesting as the size of residual tumor post-treatment. Consequently, this study suggests that residual tumor diameter is a more fitting prognostic indicator compared to pretreatment tumor diameter.
The 2012 China CRA survey showed that tumor-associated anemia exceeded 60%. 25 Anemia can induce tissue hypoxia, alter the gene expression of tumor cells, cause changes in the proteome and genome, 26,27 enhance the invasiveness of tumors, and contribute to tumor progression. Hypoxia also promotes tumor neovascularization and induces the expression of various coagulation-promoting factors, rendering tumor cells more prone to infiltration and metastasis. 28 Hypoxia not only promotes tumor progression and metastasis but also increases the tumor’s resistance to radiotherapy and chemotherapy, thereby reducing treatment efficacy and affecting prognosis. 29,30 In addition, hypoxia can influence the oxygenation status of tumor cells, thereby affecting the sensitivity of radiation therapy. 31 A study by Liu et al. 15 suggests that pretreatment hemoglobin levels serve as independent prognostic factors, aligning with the results of this study. Barkati et al. 32 found that patients with lower pretreatment hemoglobin levels exhibited a higher recurrence rate and lower OS and disease-free survival compared to patients with higher hemoglobin levels. Haensgen et al. 33 demonstrated that a pretreatment hemoglobin of 11 g/dL was correlated with better overall 3-year survival. In terms of pathological factors, patients with adenocarcinoma display poor radiotherapy sensitivity, low treatment response, and a higher risk of local recurrence and distant metastasis due to tumor biology, resulting in a poorer prognosis compared to patients with squamous cell carcinoma. 34,35
This study categorized participants into two groups, CCRT + AC and CCRT, based on the utilization of AC after CCRT. Subgroup stratified analysis of factors related to survival prognosis was conducted using a forest plot. The findings indicate that patients with residual tumors >2 cm after treatment, accompanied by P-LNM and adenocarcinoma pathology, as well as those with pretreatment hemoglobin levels below 100 g/l, demonstrated significantly better prognosis in terms of both PFS and OS when receiving AC compared to those who did not. In the IVA stage, patients with poorer prognosis due to rectum or bladder involvement showed an improvement trend in PFS, with statistically significant improvements observed in OS. LACC patients with these high-risk factors remain at an increased risk of disease progression even after receiving CCRT. AC, as opposed to treatment observation alone, may confer survival benefits to these patients. At present, there is no standardized treatment plan for residual lesions in the cervix after CCRT. Although pelvic dissection may introduce more complications without improving OS (69% at 2-year OS), 31% of patients still experience recurrence after pelvic palliative surgery. 36 The purpose of AC is to eliminate micrometastatic lesions within and outside the radiation field after CCRT, reduce the risk of distant metastasis, further promote residual tumor regression, and potentially benefit the survival of high-risk populations with adverse prognostic factors mentioned above.
Based on the authors’ research findings, specific comparisons with the OUTBACK study can be drawn. Notably, this study demonstrated a high completion rate of over 95% for radical radiotherapy, which significantly differs from the OUTBACK study where the completion of CCRT was affected in 23% of patients due to increased toxicity. 10 This highlights better patient compliance in this study, potentially contributing to more reliable final results. Moreover, this study’s subgroup analysis reveals a distinct benefit of AC in high-risk groups, including patients diagnosed with adenocarcinoma, pelvic LNM, and anemic conditions, as well as those with noticeable residual lesions after radiotherapy and IVA staging. This contradicts the OUTBACK study’s suggestion that unselected AC might not be suitable for all LACC cases. On the contrary, the authors’ findings indicate that selected patient groups do seem to derive significant benefits from AC. This suggests a need for a more stratified approach when considering AC for LACC, especially in high-risk patients. It is worth noting that the majority of patients enrolled in the OUTBACK study were of stage I and IIB, whereas this research focused solely on LACC. Therefore, it becomes essential to consider these differences and the potential underestimation of AC’s value when interpreting the comparative results of both studies. Notably, the positive outcomes from South American phase III randomized controlled studies using gemcitabine combined with cisplatin in CCRT and AC further signify the ongoing exploration in assessing the value of AC for LACC.
In summary, this study constructed a prognostic model using the 2018 FIGO staging system to predict OS and PFS in LACC patients treated with CCRT, with or without AC. The model, which includes a nomogram for personalized predictions, showed good predictive accuracy in internal validation. It suggests that AC may benefit high-risk patients, such as those with residual tumors larger than 2 cm post-treatment. In addition, LNM, including the number and size of involved nodes, is a significant survival predictor. However, due to the retrospective nature of this study, which limits the ability to capture detailed lymph node information, the authors encourage future prospective studies for a more thorough analysis. While this model was internally validated, its generalizability requires further confirmation through external validation. The findings highlight the need for more research to determine the optimal use of AC.
Footnotes
Authors’ Contributions
L.H. and M.W. designed the study, provided administrative, technical, or material support, obtained funding, acquired data, and performed statistical analyses. S.L., X.W., and C.F. contributed to the follow-up, data collection, and analyses. S.C. revised the manuscript, supervised the study, and provided important intellectual content. S.C. provided administrative, technical, or material support. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Guangxi Major Scientific Research & Technology Development Plan (2021AB12004).
Availability of Data and Materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approval by the Ethics Committee of the Forth Affiliated Hospital of Guangxi Medical University. Written informed consent was obtained from each patient.