
Abstract
This study assesses fibroblast activated protein inhibitor (FAPI) targeted PET/CT imaging against [18F]FDG PET/CT (FDG PET) for detecting nodal involvement in head and neck squamous cell carcinoma (HNSCC), intending to improve diagnostic precision for metastatic lymph nodes and lay the groundwork for future investigations.
Methods:
Patients diagnosed with HNSCC were retrospectively enrolled. All patients underwent [68Ga]Ga-FAPI04 PET/CT (FAPI PET) and FDG PET within 6 d. Primary tumor, lymph nodes, and tracer uptake were visually and quantitatively compared. The metastatic lymph nodes were evaluated using patient-and lesion-based analyses, with biopsy or postoperative histopathological examination as the reference.
Results:
The cohort includes 24 patients (17 men, 7 women; mean age 60 ± 11.8 years) who underwent FDG and FAPI PET for preoperative diagnostic workup or restaging due to known recurrence of HNSCC. Lesions included 24 primary tumors, 54 cervical lymph nodes, and 5 metastases. Primary tumors exhibited significant uptake on both PET modalities (median maximum standardized uptake value [SUVmax]: FDG 19.4 ± 11.6, FAPI 16.9 ± 4.6), with no statistically significant difference (p > 0.5). For lymph nodes, FAPI and FDG PET showed median SUVmax of 9.18 ± 6.77 and 9.67 ± 6.5, respectively. The patient-based analysis found FDG PET sensitivity at 88.2% and FAPI PET at 94.1%, with FAPI PET specificity significantly higher (85.7% vs. 42.8% for FDG PET). Lesion-based analysis revealed FAPI PET sensitivity and specificity at 84.2% and 93.7%, respectively, contrasting FDG PET’s at 81.5% and 25%, respectively.
Conclusion:
This study underscores the efficacy of FAPI PET in detecting primary tumors in HNSCC. Furthermore, FAPI PET shows improved specificity over FDG PET for metastatic lymph nodes advocating further investigations for integrating FAPI PET into HNSCC clinical protocols for its enhanced precision in detecting metastatic lymph nodes.
Introduction
Head and neck squamous cell carcinoma (HNSCC), the seventh most common malignancy worldwide, encompasses various tumors originating in the lip, oral cavity, hypopharynx, oropharynx, nasopharynx, or larynx. While the burden of HNSCC varies among countries, it constitutes 3% of all cancer cases and ∼1.5% of global cancer-related deaths. 1 In a significant proportion of patients, diagnosis in advanced stages is associated with short life expectancy, high death rates, and treatment-related morbidity, highlighting the need for precise and reliable imaging tools in clinical practice. 2 In this regard, [18F]FDG PET/CT (FDG PET) has demonstrated its utility in oncological imaging. However, recurrent challenges with FDG PET, particularly false positive uptake, have revealed significant limitations in HNSCC management, particularly in precisely identifying metastatic lymph nodes. This manifestation is notably accentuated in the complex anatomical landscape of the head and neck region, where physiological processes can mimic pathological uptake, thus impacting treatment strategy and patient outcomes. 3,4
The introduction of fibroblast activation proteins (FAP) overexpressed on cancer-associated fibroblasts (CAFs) and 68Ga-labeled FAP inhibitors (FAPIs) have demonstrated encouraging results 5 –7 for widespread oncological applications, including HNSCC. Low FAPI uptake in almost all normal tissues 8 and high uptake 9 across a wide range of cancer types 10 –12 have already been validated in the literature; thus, FAP-targeted imaging may be considered an alternative PET modality to overcome the inherent limitations 13 of FDG PET in the clinical management of HNSCC.
In summary, the comparative findings of FAPI and FDG PET may advance our understanding of optimal diagnostic approaches in critical aspects of HNSCC. We conducted this study to investigate the diagnostic accuracy of [68Ga]Ga-FAPI04 PET/CT (FAPI PET) and its potential advantages in overcoming the limitations of FDG with a particular emphasis on nodal involvement, which is a pivotal factor influencing therapeutic decision-making and prognosis.
Methods
Study design and patients
Among patients who underwent FAPI PET for various malignancies, 24 patients diagnosed with HNSCC were retrospectively reviewed. Patients were initially referred for FAPI PET imaging by an interdisciplinary head and neck oncology board in the presence of surgeons, radiation oncologists, nuclear medicine physicians, and radiologists to supplement FDG PET imaging if they met the following criteria: (1) patients with histopathologically proven HNSCC, (2) no prior chemoradiotherapy or surgery in the last 8 weeks, (3) patients who underwent FDG PET as a part of a preoperative diagnostic workup procedure or for restaging due to known/suspected recurrence, (4) no history of other primary malignancies, and (5) no patients under 18 years old. This retrospective study was approved by the local institutional review board (document no: 2021/111.3), and written informed consent was obtained from all patients. The primary endpoint was to determine the diagnostic accuracy of FAPI PET compared with FDG PET in detecting lymph node metastasis. The secondary objective was to determine the discrepancies between FDG and FAPI for evaluating primary tumors and distant metastasis, if any.
[68Ga]Ga-FAPI04 synthesis
The synthesis of [68Ga]Ga-FAPI04 was performed using a fully automated, GMP-compliant SCINTOMICS GRP® module with disposable single-use cassette kits (ABX), FAPI-04 (Huayi Isotopes Co, China), and a 68Ge/68Ga-generator (iThemba Labs, South Africa). The 68Ga solution eluted from the generator with 0.6 M hydrogen chloride was prepurified using a cation exchange cartridge and eluted with 5 M sodium chloride. The 68Ga was then added to 25 µg FAPI in HEPES buffer and heated for 20 min at 90°C. The reaction mixture was transferred to a preconditioned SepPak C18 cartridge, washed with water, eluted with ethanol/water (50/50) and filtered through a 0.22 µm sterile filter. The final product was diluted with phosphate buffer solution to a total volume of 15 mL, achieving a radiochemical purity of over 98% as determined by high-performance liquid chromatography and thin-layer chromatography.
PET/CT imaging and evaluation
Images were acquired 50–70 min after intravenous injection of [18F]FDG (2.5 MBq/kg ±10%) and 40–50 min after [68Ga]Ga-FAPI04 (injected activity range 187–259 MBq) on separate days (2–6 d), using a Discovery IQ PET/CT scanner (GE Healthcare) and reconstructed using the Bayesian penalized likelihood reconstruction algorithm (Q.Clear) with a penalization factor (beta) of 300. All acquired data were transferred to the Advantage Workstation (version 4.7, GE Healthcare) for visual evaluation. Two board-certified nuclear medicine physicians, blinded to all clinical and imaging data, evaluated FDG and FAPI PET scans in consensus. A positive lesion was defined as an increased activity within the primary tumor, regional lymph node, or distant metastasis greater than the surrounding background. The primary tumor, the number and locations of all lymph nodes, and metastatic lesions were documented. A region of interest was drawn manually along the borders of the primary tumors on the CT counterpart of PET images, and the maximum standardized uptake value (SUVmax) was measured accordingly. On the contrary, a circular ROI was drawn around the lymph nodes and metastatic lesions. All calculations were performed using the dedicated software of the manufacturer (GE Healthcare, AW 4.7).
Statistical analysis
Continuous variables were described by median and range, and qualitative variables were described by the frequency of their modalities where appropriate. All statistical analyses were performed using IBM SPSS Statistics (Version 21.0). Histopathological results, obtained through biopsy or surgery, served as the reference standard for calculating the diagnostic performance of imaging studies in detecting primary tumors and metastatic lymph nodes. Due to an insufficient number of patients with distant metastasis, no statistical tests were conducted for metastatic lesions.
Results
Patient characteristics
The study cohort included 24 patients, 17 men and 7 women, aged between 34 and 79 (mean age of 60 ± 11.8 years). All lesions, totaling 24 primary tumors, 54 cervical lymph nodes, and 5 metastases, were documented. All primary lesions underwent histopathological confirmation through biopsy or postoperative histopathological examination. In five patients who underwent lymph node dissection, the presence of metastatic lymph nodes was confirmed through histopathological examination performed after surgery. On the contrary, in 19 inoperable patients, all lymph nodes demonstrating radiotracer uptake underwent biopsy. Histopathological examination confirmed the presence of metastatic or reactive lymph nodes, thereby determining their true or false positive status. In patients with no pathological radiotracer uptake in the cervical lymph nodes on the PET scans, true negativity of the lymph nodes was determined primarily on clinical follow-up, radiological imaging, and biopsy when necessary or a combination of these methods. Distant metastasis in three patients was also confirmed through clinical follow-up and radiological imaging. All confirmations, whether through biopsy, postoperative examination, clinical follow-up, or radiological imaging, were meticulously conducted by a multidisciplinary board. The demographic and tumor characteristics of patients are summarized in Table 1.
Patient Characteristics
SUVmax, maximum standardized uptake value; FAPI, fibroblast activated protein inhibitor.
Primary lesions
The primary tumors in all patients exhibited significant uptake on both PET modalities. The median SUVmax for the primary tumors on FDG PET was 19.4 ± 11.6, whereas the median SUVmax on FAPI PET was 16.9 ± 4.6. There was no statistically significant difference between FDG and FAPI PET measurements (p > 0.5).
Lymph nodes
In patient-based analysis, the lymph nodes’ median FAPI and FDG SUVmax were 9.18 ± 6.77 and 9.67 ± 6.5, respectively. Out of 24 patients, 17 were diagnosed with lymph node metastases. FDG PET failed to detect metastases in two cases, while FAPI PET missed one. As a result, FDG PET yielded 15 true positives and 2 false negatives, whereas FAPI PET yielded 16 true positives and 1 false negative. Conversely, FAPI PET demonstrated false positive lymph node uptake in one patient, while FDG PET exhibited false positive results in four out of the seven patients without lymph node metastases. Consequently, FAPI PET resulted in six and FDG PET three true negatives. Overall, the sensitivity of FDG PET and FAPI PET in detecting lymph node metastasis on a patient basis was comparable (88.2% vs. 94.1%, respectively); however, the specificity of FAPI PET (85.7%) was significantly higher than FDG PET (42.8%).
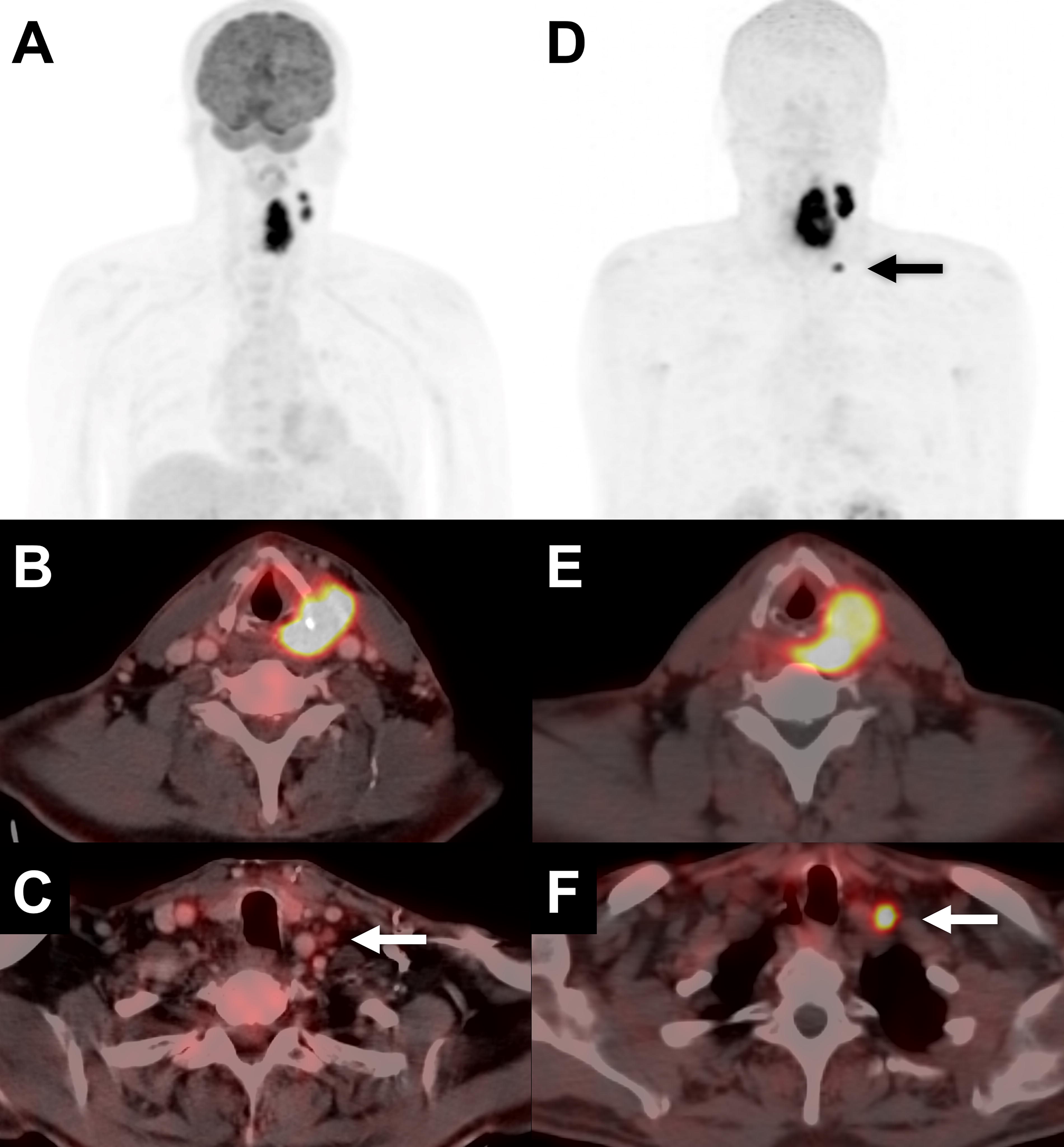
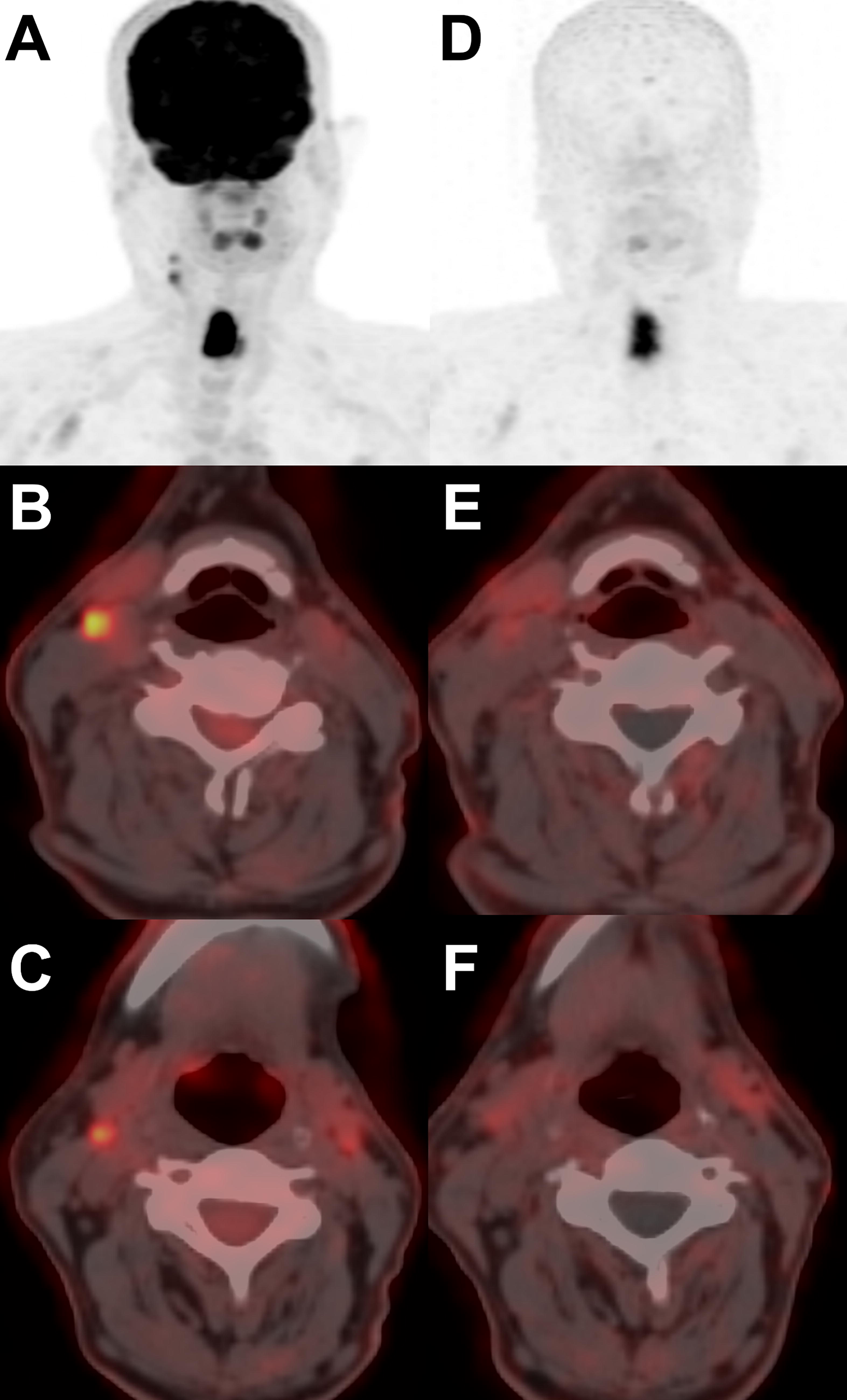
We also conducted a per-lesion analysis in a subset of five patients who underwent lymph node dissection, wherein all lymph nodes were confirmed through histopathological examination. In the lesion-based analysis, histopathological examination identified metastases in 38 (70.4%) of the 54 cervical lymph nodes. FAPI PET detected uptake in 32 lymph nodes, while FDG PET identified uptake in 31 lymph nodes, with agreement on 30 lesions. As a result, metastases in five lymph nodes were exclusively identified through postoperative histopathological examination, and two metastatic lymph nodes were detected by either FDG (Fig. 1) or FAPI (Fig. 2) PET alone. Histopathological examination proved reactive features in 16 lymph nodes; one was FAPI-positive (Fig. 3) and 12 were FDG-positive (Fig. 4). The lesion-based sensitivity and specificity of FDG PET were 81.5% and 25%, while respective values for FAPI PET were 84.2% and 93.7%. The performance of PET modalities is summarized in Table 2.
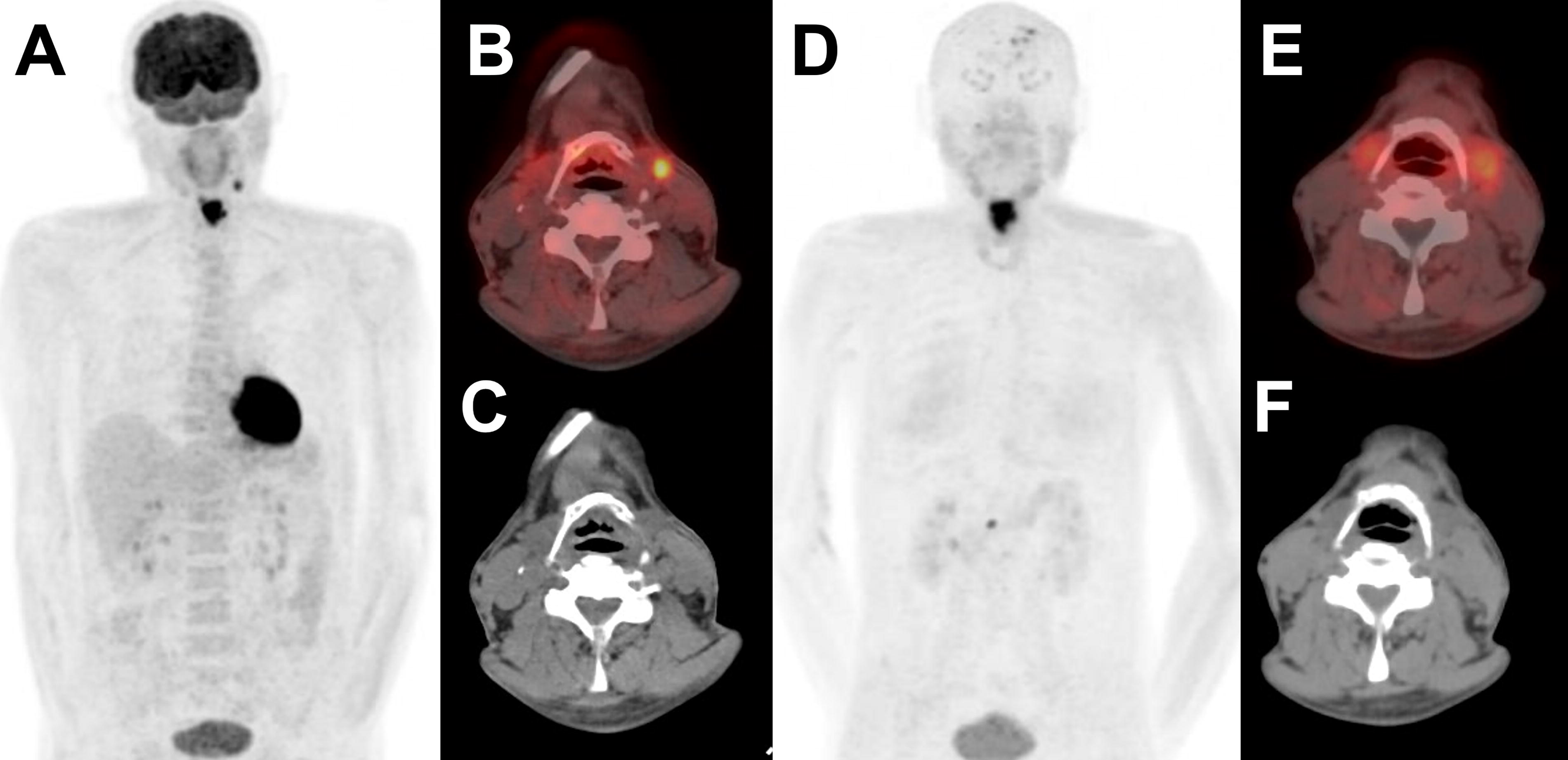
The hypermetabolic lymph node identified [18F]FDG PET/CT MIP
[18F]FDG PET/CT showed significant uptake in the multiple metastatic lymph nodes at the superior deep cervical
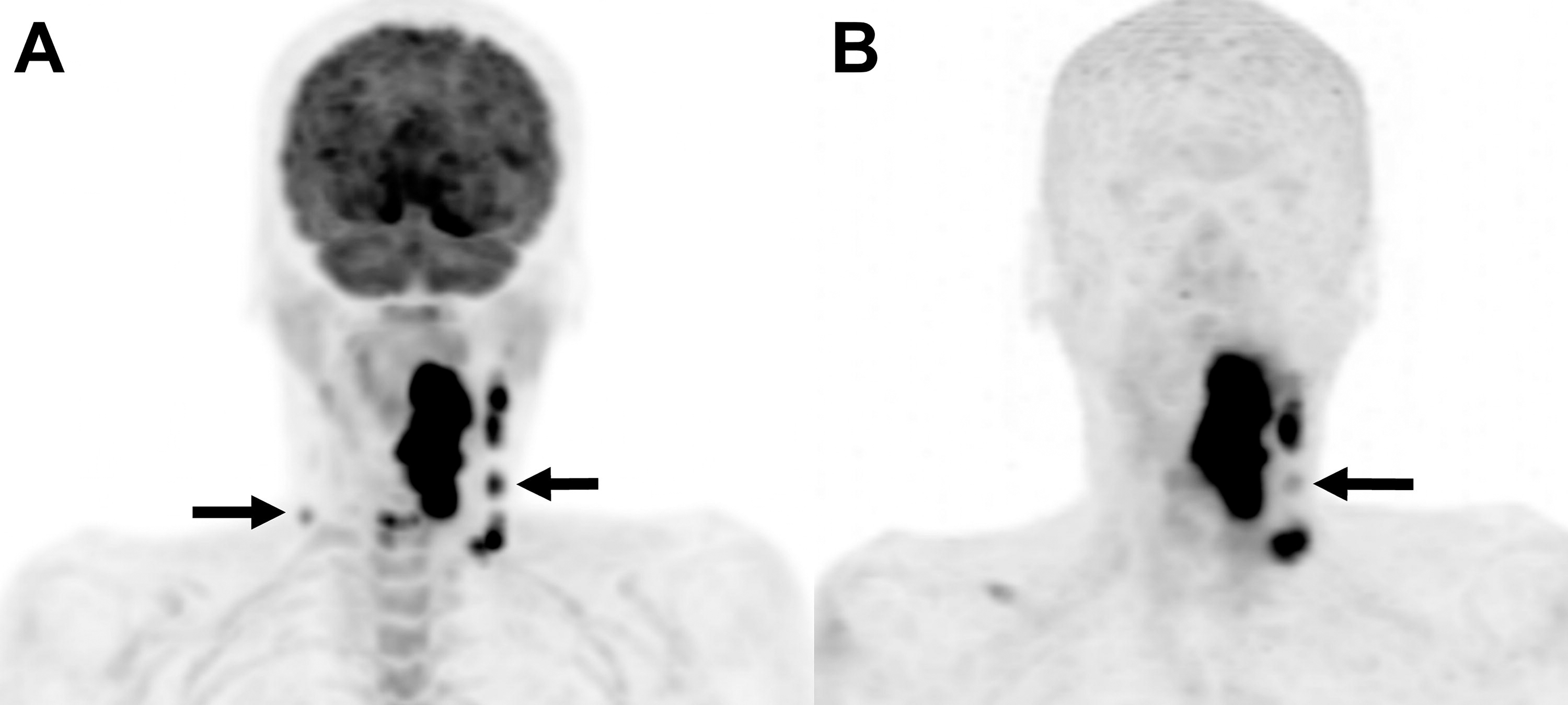
This figure contrasts [18F]FDG PET/CT and [68Ga]Ga-FAPI04 PET/CT images, detecting the primary tumor and metastatic lymph nodes. While [18F]FDG PET/CT identifies multiple nodes with two false positives (arrows), [68Ga]Ga-FAPI04 PET/CT shows fewer false positives (arrow), with one node displaying notably lower uptake.
[18F]FDG PET/CT demonstrates significant metabolic activity in two lymph nodes on MIP
Diagnostic Accuracy of [18F]FDG PET/CT and [68Ga]Ga-FAPI04 PET/CT in Detecting Nodal Metastasis
Distant metastasis
Three patients were presented with distant metastasis. All metastatic lesions were determined through clinical and radiological follow-up. The mean SUVmax of three metastatic lung lesions of two patients was 5.35 ± 1.4 on FAPI PET and 7.95 ± 0.3 on FDG PET. One patient was presented with a metastatic bone lesion with an SUVmax of 3.4 on FAPI and 5.59 on FDG PET. In addition, one FDG- and FAPI-positive metastatic liver lesion was detected in one patient.
Discussion
Nodal staging in HNSCC is crucial due to its pivotal role in prognosis, treatment planning, and therapeutic decision-making. Several studies have reported sensitivity of FDG PET/CT ranging from 70% to 90% in nodal staging of HNSCC. However, it fails to provide a comprehensive diagnostic assessment due to the complex anatomy of the neck region. It is well established that FDG fails as a specific marker for malignancy given its propensity for uptake in normal or actively inflamed tissues, thus posing challenges in scan interpretation.
These limitations have prompted the need for more specific PET tracers, which can help distinguish between tumor activity and inflammation. In this regard, clinical investigations have focused on radiopharmaceuticals such as [18F]fluorothymidine ([18F]FLT), [18F]fluoroethyl-
In this study, we compared the diagnostic efficacy of FAPI PET/CT and FDG PET/CT in a cohort of 24 patients with HNSCC. Our results showed that both modalities demonstrated high tracer uptake in all the primary lesions with a median SUVmax of 19.4 ± 11.6 and 16.9 ± 4.6 for FAPI PET/CT and FDG PET/CT, respectively. Although a higher value with FAPI PET was measured, there was no statistically significant difference (p > 0.5). In a cohort of 15 nasopharynx carcinoma, Quin et al. 14 also reported a 100% detection rate. In contrast, FDG uptake was higher than FAPI PET in their study but similarly, they were comparable with no statistically significant difference. Chen et al. 15 in a cohort of 36 oral SCC also demonstrated high SUVmax values on both modalities with no statistically significant difference observed. With the high detection rates observed within the specific cohort of patients already identified as positive, it is imperative to recognize the potential presence of patient selection bias as a notable limitation. The principal objective of this study did not center on assessing the diagnostic efficacy of FAPI PET in identifying primary tumors, a facet already well-documented in existing literature. 16 However, recent findings by Gu et al. 17 underscore the promising utility of FAPI PET, particularly in discerning primary tumors among FDG-negative head and neck cancers with unknown primary, thereby highlighting its potential superiority over FDG PET in this clinical context. Furthermore, within our cohort, FAPI PET showcased a remarkable tumor-to-background ratio in the primary tumors during visual interpretation than that of FDG PET, a finding consistently supported by several studies. 16 In this regard, FAPI PET holds promise offering enhanced delineation of head and neck tumors addressing the limitations of FDG PET in image-guided radiotherapy. The potential of FAPI PET in this context has recently been demonstrated by Syed et al., 18 warranting further research.
Maintaining a cautious approach when interpreting FDG PET/CT results in the context of head and neck cancers is crucial. The paramount consideration lies in the recognition of false positivity as a critical pitfall that can potentially lead to unnecessary interventions, such as biopsies or surgeries. The high incidence of inflammation and reactive hyperplasia is a well-established aspect contributing to false positive FDG uptake in lymph nodes. 19 Reactive histological features were observed in 16 lymph nodes with only one of them testing positive for FAPI while FDG was positive for 12 of these lymph nodes. Consequently, fewer false positive lymph nodes with FAPI PET resulted in a higher specificity in both patient- and lesion-based analyses. In patient-based analysis, we measured the sensitivity and specificity of FAPI PET and FDG PET as 94.1% versus 88.2% and 85.7% versus 42.8%, respectively. Our findings align with those of Chen et al. 15 who reported similar results based on histopathological confirmation: 94.74% versus 100% for sensitivity and 100% versus 29.41% for specificity. Furthermore, in the study by Qin et al. 14 , although FDG PET demonstrated higher uptake than FAPI PET (11.94 vs. 8.81) FAPI PET detected 100 and FDG PET detected 48 lymph nodes. However, their study lacked histopathological verification. Transitioning to the lesion-based analysis, we observed nuanced differences in detection rates. In five patients who underwent lymph node dissection, a lesion-based analysis was performed for 54 lymph nodes, of which 38 were histopathologically confirmed metastases. The detection rates of FAPI PET and FDG PET were 84.2% and 81.5%, respectively. In a study by Zhao et al., 20 a lesion-based analysis of 121 metastatic lymph nodes in nasopharyngeal carcinoma showed a higher detection rate favoring FAPI PET. The difference was notably significant (95% vs. 72%, p < 0.001) compared with our findings, which did not demonstrate a statistically significant difference. Furthermore, the SUVmax of lymph nodes was significantly higher in FAPI PET (11.12 vs. 6.53; p < 0.001) in their study, in contrast to our cohort, which did not demonstrate a statistically significant difference (p > 0.5) as determined by the median SUVmax for FAPI PET and FDG PET (9.18 and 9.67, respectively). Our results are consistent with prior research findings for diagnostic efficacy, highlighting the potential of FAPI PET to enhance specificity. In line with these findings, FAPI uptake was observed in a single reactive lymph node, which improved specificity in our cohort. Nevertheless, it is also crucial to recognize false positive findings or instances of nonmalignant FAPI uptake, a phenomenon well-documented in existing literature. 21 Accordingly, the false positive uptake in a single lymph node may be attributed to the nonspecific fibrosis induced by inflammation as previously described. 22 Hence, inflammation emerges as a primary factor in explaining nonmalignancy on FAPI PET/CT.
We observed a strong agreement between FAPI PET and FDG PET in identifying metastatic lymph nodes, yet there were instances where metastatic lesions were undetected by both modalities. FAPI PET overlooked six lymph nodes and FDG PET missed seven. False negativity may be attributed to several factors, such as the small size of the lesion or inherent constraints of PET scanners, such as the partial volume effect. We believe the small size of metastatic lymph nodes in our cohort likely contributed to these findings. As determined by histopathological examination, there were millimetric metastatic lymph nodes. In this regard, the retrospective nature of our study is a significant limitation due to lack of a prospective surgical approach, thus a size comparison between false negative and true positive lymph nodes could not be performed. However, we observed metastatic lymph nodes with high metabolic activity despite their small size, which may be indicative of aggressive lesions, as both FAP expression and high glucose metabolism are recognized as poor prognostic markers. Therefore, biological variations within lesions including tumor heterogeneity, low FAP expression in the tumor or surrounding stroma, or low glucose metabolism in certain lesions can impact detection sensitivity. In addition, the presence of necrosis within lymph nodes can reduce FDG uptake, further contributing to false negatives, nevertheless, such observations were not noted in our study.
Higher FAPI uptake than FDG was observed in three metastatic lung lesions (mean SUVmax: 7.95 vs. 5.35) and one metastatic liver lesion (SUVmax:16.07 vs. 5.35). On the contrary, Zhao et al. 20 found that FAPI PET was superior to FDG PET in detecting 41 distant metastases. However, our results do not offer adequate statistical evidence due to the limited number of lesions. Nevertheless, both PET modalities exhibited similar performance in detecting metastases. Gu et al. 17 also reported similar performance for FAPI PET and FDG PET in the detection of metastases; however, in their study SUVmax values were comparable. Qin et al. 14 reported three metastases detected exclusively by FAPI PET in a single patient. These lesions were located at the skull base, where brain activity could potentially have interfered with the activity on FDG PET. Alternatively, these reports indicate high FAP expression in metastatic lesions and considering the previously reported safety of FAP-targeted radionuclide treatments, 23 FAPI PET has the potential to strengthen treatment decisions in the realm of FAP-targeted theranostics.
Several limitations should be disclosed. First of all, the small sample size of 24 patients may constrain the generalizability of the results to larger populations. Nonetheless, FAPI PET holds particular value due to the limited data available in the existing literature. We believe it contributes valuable insights into the diagnostic efficacy of FAPI PET in HNSCC within this particular context. The retrospective design also introduces biases that, coupled with the small sample size, limit the ability to draw statistical conclusions. Future prospective studies with larger cohorts are essential to validate these initial findings and provide a more comprehensive understanding of FAPI PET in the management of HNSCC.
Conclusion
This study demonstrates the remarkable efficacy of FAPI PET in detecting primary tumors and metastatic lymph nodes in HNSCC, showing results equivalent to FDG PET. The reduced incidence of false positives and the consequent enhanced specificity of FAPI PET in detecting lymph nodes exceed those of FDG PET, warranting further investigation into its potential clinical benefits.
Footnotes
Authors’ Contributions
S.K. and E.G.I.: Led the study’s design and data interpretation. C.Ş. and B.B.: Contributed clinical expertise and patient follow up. D.H.-Ş. and Z.G.Ö.: Conducted the literature review and drafted sections of the manuscript. F.B.: Managed the technical aspects of radiopharmaceutical preparation and quality control while Y.Ş.: Refined the manuscript during revisions.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.