
Abstract
Objective:
This study aims to comprehensively evaluated the efficacy and safety of bronchial arterial chemoembolization (BACE) in the treatment of advanced nonsmall cell lung cancer (NSCLC) through a meta-analysis of single-group rate, providing evidence-based guidance for clinical treatment.
Materials and Methods:
A systematic search was conducted in PubMed, the Cochrane Library, Embase, and Web of Science databases for relevant studies up to January 15, 2024. Inclusion criteria encompassed single-arm or multi-arm studies of nonrandomized controlled trials, observational studies, and single-arm studies in English language, focusing on NSCLC patients treated with BACE. Data extraction, quality assessment, and statistical analysis were performed following predefined protocols.
Results:
In total, 172 articles were initially retrieved, with 11 studies meeting the inclusion criteria. The included studies comprised 510 patients. Meta-analysis revealed significant heterogeneity among studies for median progression-free survival (PFS), median overall survival (OS), objective response rate, and disease control rate. The combined median PFS was 6.87 months (95% confidence interval [CI] 5.30–8.44), and the combined median OS was 13.68 months (95% CI 10.69–16.67). Subgroup analysis based on intervention measures demonstrated varying efficacy outcomes. Adverse reactions associated with BACE were generally mild, with no reports of grade 3 or higher adverse events.
Conclusion:
BACE emerges as a promising treatment modality for advanced NSCLC, exhibiting favorable efficacy and safety profiles.
Introduction
Lung cancer is the malignant tumor with the highest morbidity and mortality rates in China and worldwide. 1 –5 According to the latest epidemiological data provided by the World Health Organization, there are about 20 million new cancer cases in 2022, while 9.7 million people died from cancer. Lung cancer is the most commonly diagnosed cancer in 2022, accounting for nearly 2.5 million new cases (12.4% of all cancers globally); it remains the foremost cause of cancer mortality, accounting for an estimated 1.8 million deaths, which represents 18.7% of all cancer-related fatalities. This is followed by colorectal cancer at 9.3%, liver cancer at 7.8%, female breast cancer at 6.9%, and gastric cancer at 6.8%. 6 Nonsmall-cell lung cancer (NSCLC) accounts for 80%−85% of all primary lung cancer, 7,8 specific pathological typing is shown in Figure 1. Due to the lack of public awareness of the clinical manifestations of NSCLC, most of the patients are advanced when diagnosed, resulting in extremely low 5-year survival rates. 3,4,9 –11 Figure 2 presents the detailed mechanisms involved in the development of lung cancer.
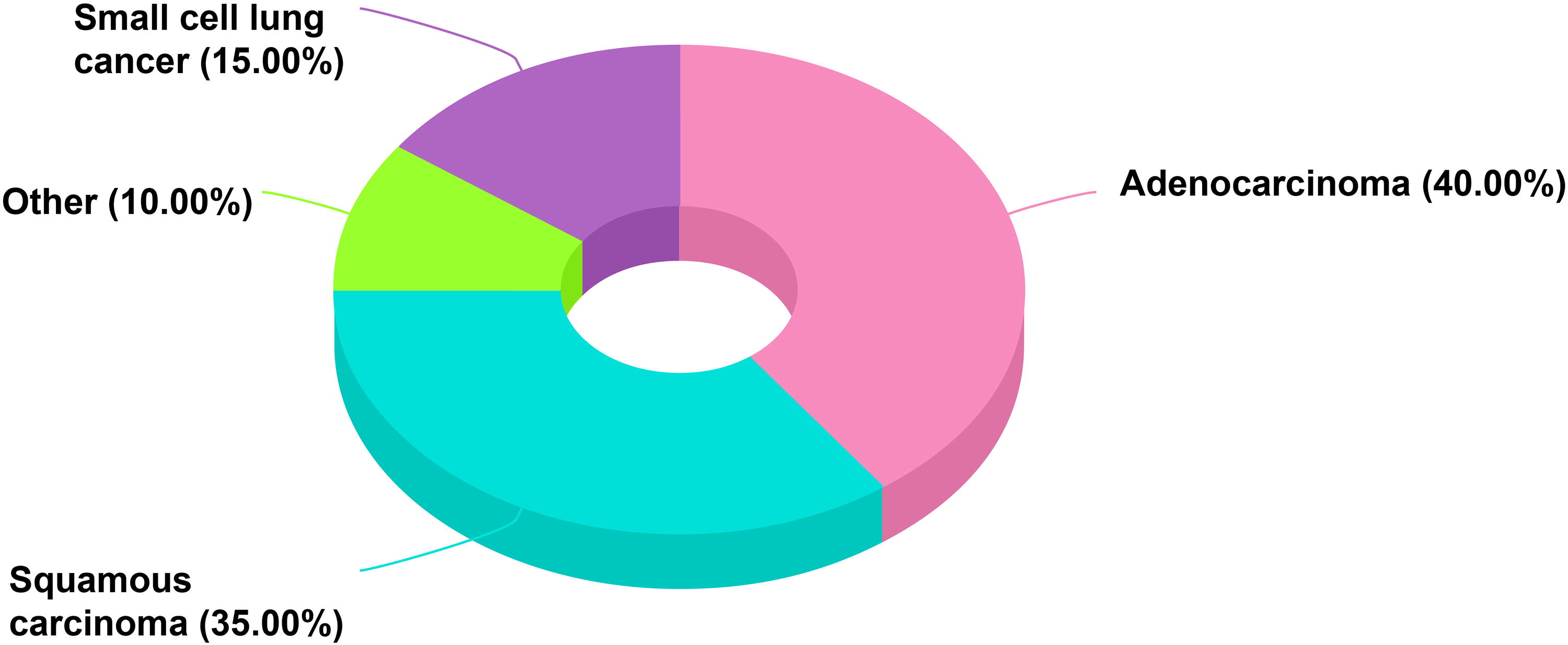
Proportions of lung cancer subtypes published by WHO in 2022.
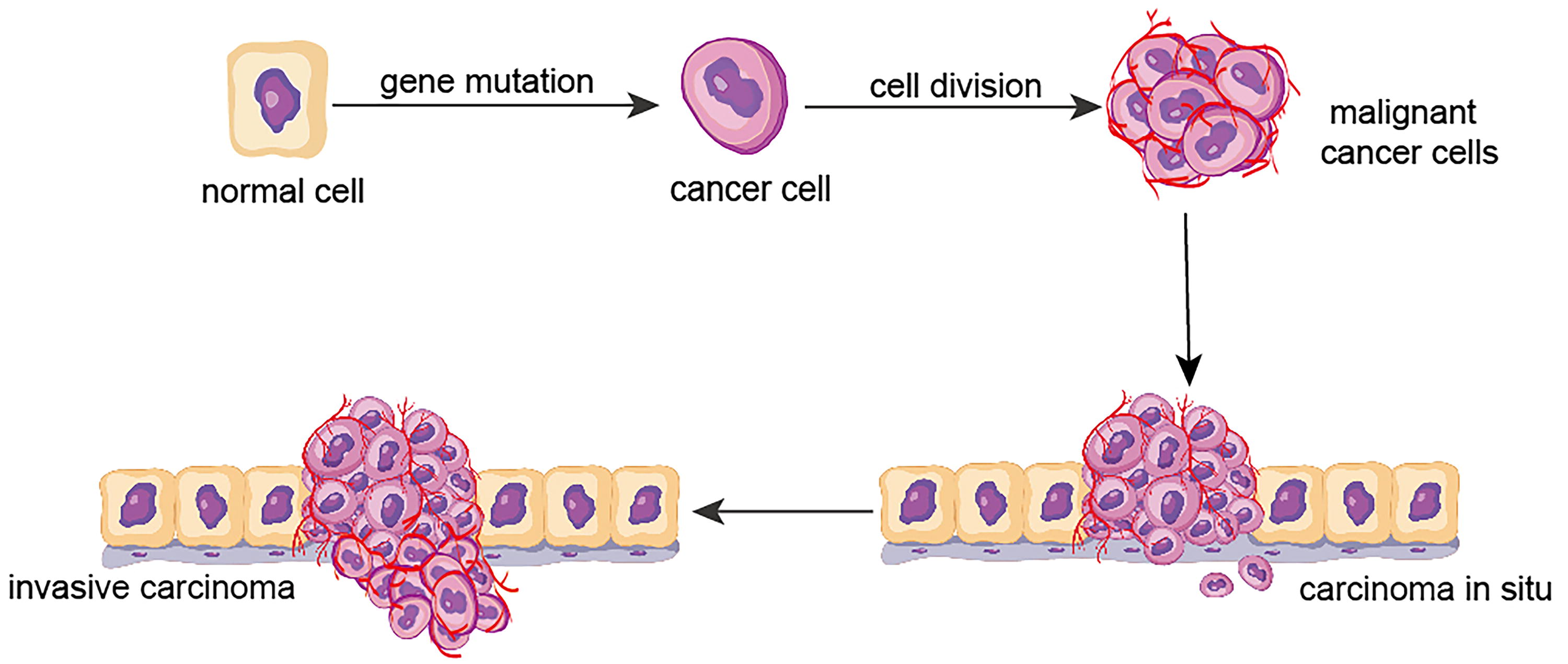
The development of lung cancer.
The preferred approach for addressing lung cancer involves an anatomical lobectomy, coupled with a dissection of both mediastinal and hilar lymph nodes, 12,13 but since 70% of lung cancer patients are at progressive stage when diagnosed, the surgical resection rate is less than half. 4,10 For those patients who are ineligible for surgery, alternative treatment options must be explored. Currently, the first-line treatment for advanced inoperable NSCLC is mainly platinum-based two-agent chemotherapy combined with radiotherapy and targeted therapy, 14 –19 but patients with NSCLC are often insensitive to systematic chemotherapy and radiotherapy. In addition, adverse reactions such as cancer recurrence, chemotherapy resistance, hematological toxicities, and neuropsychiatric toxicities often lead to patient refusal or intolerance, resulting in generally poor prognoses for the majority of patients. 14,20,21 Hence, it is essential to prioritize effective and less toxic treatments to improve the long-term prognosis for patients with advanced NSCLC. The treatment of locally advanced patients with NSCLC who have failed first-line concurrent chemoradiotherapy is challenging, and searching for effective methods to control localized cancer foci in the lungs is one of the research hotspots in advanced tumor research.
In recent years, interventional therapy has the advantages of minimally invasive, satisfactory efficacy, fewer adverse reactions, quicker postoperative recovery, and saving treatment cost, and has been widely used in the treatment of lung cancer, which significantly increases the survival rate of patients and improves their quality of life. Among them, bronchial arterial chemoembolization (BACE) has become a research hotspot in the field of lung cancer. 22,23 It can not only block the blood supply arteries of the tumor but also directly deliver chemotherapy drugs to the tumor site and release them slowly, thereby prolonging the drug action time, increasing the local drug concentration in the tumor, reducing the blood drug concentration and toxicity throughout the body, and promoting tumor ischemic and necrosis. 24 Although BACE has demonstrated some efficacy and safety in the treatment of advanced inoperable NSCLC, the available studies are limited by small sample sizes and a lack of backing from large-scale randomized controlled trials (RCTs). The meta-analysis of single-group rates is a methodological approach that aggregates dichotomous data from uncontrolled cross-sectional studies, which can be clinically used to analyze clinical studies lacking large samples. Based on this, this study used meta-analysis of single-group rate to comprehensively evaluate the efficacy and safety of BACE in the treatment of advanced NSCLC, aiming to furnish a more robust evidence-based foundation for clinical decision-making.
Materials and Method
Selection criteria
Definition of study types
This study included single-arm or multi-arm studies of non-RCT, observational studies (including case-control studies and cohort studies) with single-arm or multi-arm studies, and single-arm studies. The language of the literature was limited to English.
Clarification of study subjects
Patients included in this study must meet the diagnostic criteria for NSCLC (confirmed histopathological subtype through percutaneous needle aspiration biopsy, surgery, or bronchoscopy), regardless of age, gender, race, and region, to ensure the universality and applicability of the study results.
Definition of intervention measures
All patients were treated with bronchial artery chemoembolization alone or in combination with 125I seed implantation, microwave ablation (MWA), targeted therapy, or immunotherapy. Specific embolization materials included drug-eluting microspheres, polyvinyl alcohol particles, gelatin sponge particles, and eight spheres microspheres to provide a comprehensive evaluation of the therapeutic efficacy of various embolization materials.
Determination of outcome indicators
The primary outcome indicators of this study included two items: median overall survival (median OS) and median progression-free survival (median PFS). Among them, OS was delineated as the interval extending from the initiation of treatment to the point of the patient’s death, while PFS referred to the duration from the beginning of treatment to either disease progression or death. The secondary outcome indicators of this study included two items: objective response rate (ORR) and disease control rate (DCR). According to the modified Response Evaluation Criteria in Solid Tumors, the treatment response was classified as complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). Among them, ORR was defined as CR+PR and DCR was defined as CR+PR+SD. The selection of these indicators aimed to comprehensively evaluate the effectiveness and safety of the treatment.
Development of exclusion criteria
To ensure the accuracy and reliability of the study, the following exclusion criteria were set: literature not related to the topic, non-English language literature, withdrawn literature, repetitively published literature, reviews, case reports, literature with unavailability of full text, literature with a sample size of fewer than 10 individuals, and literature with unavailable data.
Construction of literature search strategy
This study conducted a computer-based search of four major databases: PubMed, the Cochrane Library, Embase, and Web of Science. During the search process, the subject terms and free words were first determined through querying MESH, and Boolean logic operators were employed for the systematic arrangement and combination of search terms to ensure both comprehensiveness and precision in the search process. The English search terms included “Carcinoma, Non-Small-Cell Lung,” “nonsmall cell lung cancer,” “Chemoembolization, Therapeutic,” “chemoembolization,” “transarterial chemoembolization,” etc. The timeframe for the search was set to January 15, 2024 from the time of construction of each database. The detailed search formula is shown in Supplementary Material 1.
Process of literature screening and data extraction
Two researchers independently carried out the tasks of literature screening and data extraction, subsequently verifying their work through a cross-checking process. In case of any disagreement, a third researcher would be introduced for judgment. The extracted data mainly included key information such as the first author and year of publication, study type, number of patients, disease stage, pathological type, intervention measures, outcome measures, etc. When outcome measures and their 95% confidence intervals (CIs) were not stated within included studies, Kaplan–Meier curves were digitized using the Engauge Digitizer to extract relevant PFS and OS.
Quality evaluation of included literature
To ensure the scientific and rigorous nature of the study, this research used the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool to assess the quality of non-RCTs, observational studies, and other literatures. This tool contains seven evaluation dimensions, including: bias due to confounding, bias in selection of participants into the study, bias due to departures from intended interventions, bias arising from deviations from intended interventions, bias due to missing data, bias in outcome measurement, and bias in the selection of reported results.
Statistical analysis methods
In this study, using Stata MP 17.0, meta-analysis of single-group rate was conducted on both continuous variables and binary variables. The median PFS and median OS were continuous variables, and ORR, DCR, and grade ≥3 adverse events were dichotomous variables. Finally, drawings were made using Adobe Illustrator.
Meta-analysis is primarily used for quantitative pooling analysis of homogeneous data to explore differences among the included independent research data. To achieve this, heterogeneity testing is required for the included research data, including qualitative description using the Q statistic and quantitative description using the I 2 statistic, to judge the magnitude of heterogeneity among studies. When I 2 is less than 50% and p > 0.1 in the Q test, it suggests that the results of the independent studies are in good agreement, meaning that they have low heterogeneity, and we can use the fixed-effects model for integration analysis when appropriate; otherwise, we employ the random-effects model to conduct the integration analysis.
The results of the meta-analysis of single-group rate are descriptive and do not have a distinction between “positive” or “negative.” In previous meta-analysis of single-group rate, the I 2 statistic is often >90%, and the Q statistic is often <0.1. Therefore, regardless of the magnitude of the test statistics, the random-effects model will be used for the analysis in this study, and a forest plot will be used to describe the combined analysis results.
In this study, funnel plots and Egger’s test were employed to assess result bias. Symmetry in the funnel plot or a p-value > 0.05 in Egger’s test indicated a low likelihood of publication bias. In addition, the sensitivity analysis method in this study was the one-by-one exclusion method. It is based on the principle of excluding any one study in turn, and the remaining studies were re-evaluated through meta-analysis to determine if the outcomes of the original meta-analysis were substantially shaped by the impact of specific studies. When the 95% CI after excluding any one study did not include 1 or 0, it represented low sensitivity and robust results. Conversely, it represents high sensitivity and unreliable results.
Results
Overview of literature screening and included studies
After initial screening, we retrieved a total of 172 relevant articles. Through careful reading of titles, abstracts, and full-text contents, 11 articles were ultimately selected for inclusion in this study, covering the treatment outcomes of a total of 510 patients. 23,25 –34 The detailed literature screening process is illustrated in Figure 3, while Table 1 provides a comprehensive listing of the basic information for the included studies.
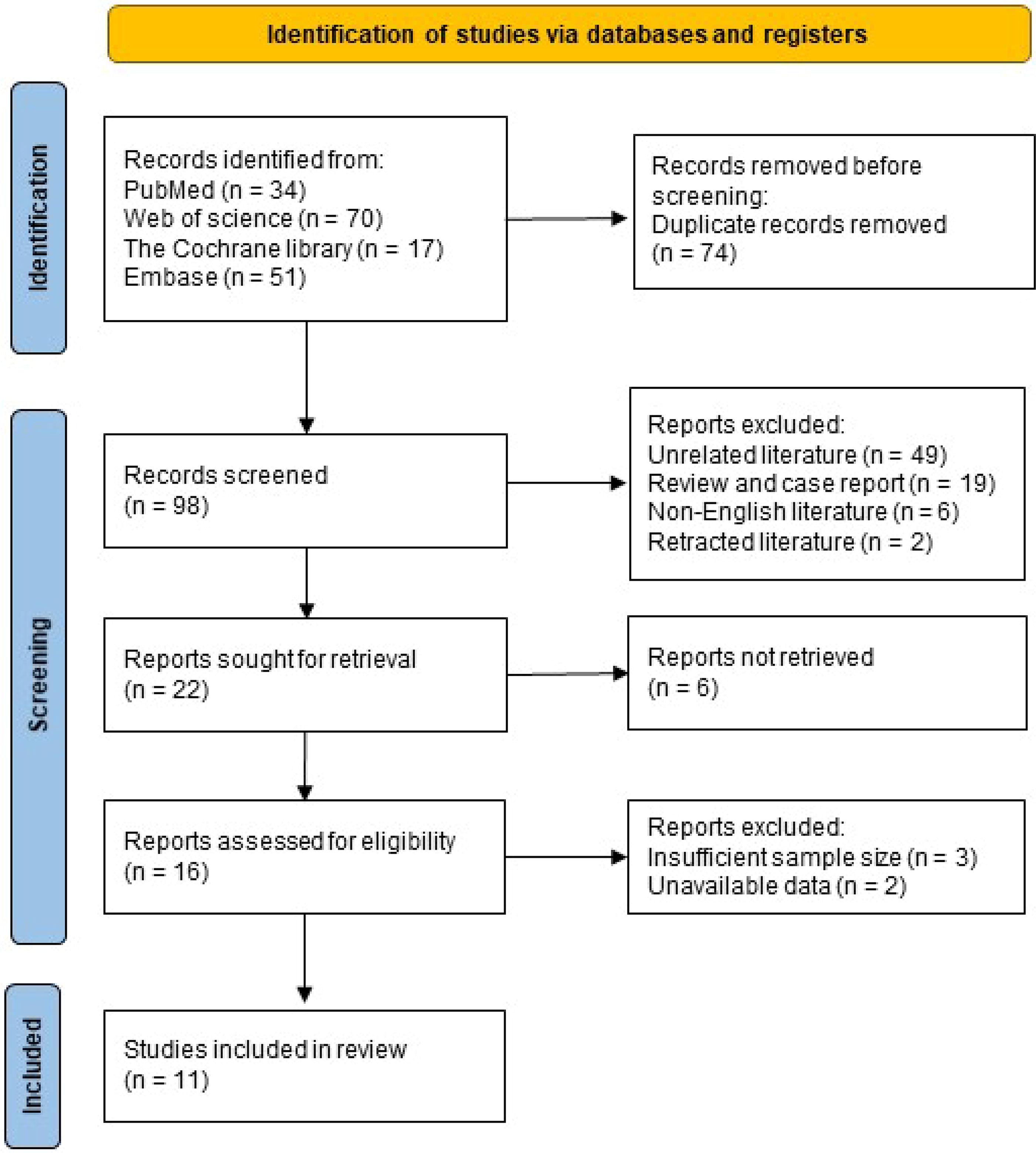
Flow diagram showing inclusion and exclusions of the studies.
Baseline Characteristics of 11 Studies (Patient and Study Characteristics)
125I, 125I seed implantation; DEB-BACE, drug eluting beads-bronchial arterial chemoembolization; ECOG, Eastern Cooperation Oncology Group; MWA, microwave ablation; PD-1, programmed cell death protein 1 blockade; PVA-BACE, gelatin sponge particles-bronchial arterial chemoembolization; SCC, squamous cell lung cancer.
Results of research quality assessment
Rigorous quality assessments were conducted on the included literature. Among them, the overall risk of bias was low for three single-arm studies and seven non-RCT studies, while the overall risk of bias was moderate for one single-arm study. This demonstrates the reliability and scientific validity of these studies, indicating a high level of research quality. The specific evaluation results are detailed in Table 2.
The Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I)
Comprehensive results of meta-analysis
Analysis of median PFS
Eight studies reported in detail the median PFS. 23,25,27,28,30 –32,34 During the statistical analysis, we detected a significant level of heterogeneity across the studies (p < 0.000, I 2 = 95.8%). Consequently, a random-effects model was utilized to perform the meta-analysis. The findings revealed that the pooled median PFS was 6.87 months (median OS = 6.87, 95% CI [5.30, 8.44]). Further subgroup analysis was performed according to various intervention strategies. The results revealed that patients treated exclusively with DEB-BACE had a median PFS of 4.75 months (median PFS = 4.75, 95% CI [2.68, 6.81]); for patients treated with BACE using other embolization materials, the median PFS was 5.97 months (median PFS = 5.97, 95% CI [2.90, 9.04]); and for patients treated with BACE combined with other treatment therapies, the median PFS was 9.36 months (median PFS = 9.36, 95% CI [7.81, 10.91]). Detailed subgroup analysis data are shown in Figure 4.
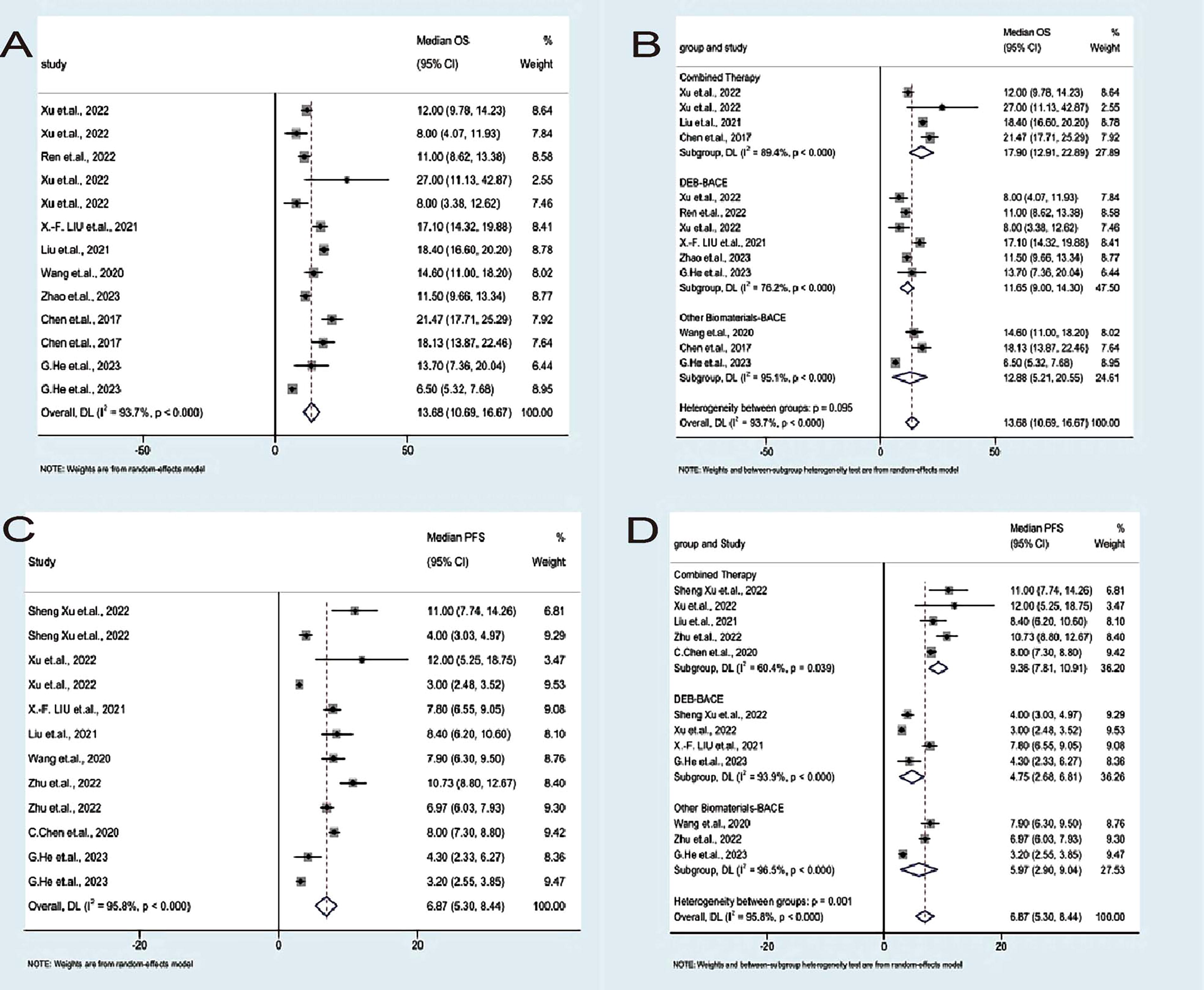
Analysis of median OS
Nine studies reported in detail the median OS. 23,26 –33 In the statistical analysis, we detected a significant level of heterogeneity across the studies (p < 0.000, I 2 = 93.7%). Thus, a random-effects model was utilized to perform the meta-analysis. The findings revealed that the pooled median OS was 13.68 months (median OS = 13.68, 95% CI [10.69, 16.67]). Further subgroup analysis was performed according to various intervention strategies. The results revealed that patients treated exclusively with DEB-BACE had a median OS of 11.65 months (median OS = 11.65, 95% CI [9.00, 14.30]); for patients treated with BACE using other embolization materials, the median OS was 12.88 months (median OS = 12.88, 95% CI [5.21, 20.55]); and for patients treated with BACE combined with other treatment therapies, the median OS was 17.90 months (median OS = 17.90, 95% CI [12.91, 22.89]). Detailed subgroup analysis data are shown in Figure 4.
Analysis of objective response rate
Ten of these studies were detailed in reporting ORR, 23,25 –29,31 –34 and we similarly observed statistical heterogeneity (p = 0.000, I 2 = 89.227%). Therefore, a random-effects model was utilized to perform the meta-analysis. The subgroup analysis indicated that the ORR for January was 0.386 (ORR = 0.386, 95% CI [0.207, 0.581]), the ORR in February was 0.586 (ORR = 0.586, 95% CI [0.355, 0.800]), and the ORR in March was 0.334 (ORR = 0.334, the 95% CI [0.111, 0.602]); the patient’s June ORR was 0.458 (ORR = 0.458, 95% CI [0.295, 0.625]). Detailed subgroup analysis data are shown in Figure 5.

Analysis of DCR
Ten of these studies reported DCRs in detail, 23,25 –29,31 –34 and we also observed statistical heterogeneity (p = 0.000, I 2 = 92.695%). Therefore, a random-effects model was utilized to perform the meta-analysis. The subgroup analysis indicated that the January DCR for patients was 0.902 (DCR = 0.902, 95% CI [0.706, 1.000]), the February DCR for patients was 0.886 (DCR = 0.886, 95% CI [0.732, 0.983]), and the March DCR for patients was 0.769 (DCR = 0.769, the 95% CI [0. 563, 0.926]); and the June DCR for patients was 0.732 (ORR = 0.732, 95% CI [0.575, 0.866]). Detailed subgroup analysis data are shown in Figure 5.
Analysis of incidence of adverse reactions
All included studies provided detailed accounts of the occurrence of adverse reactions. 23,25 –34 Among them, only three articles mentioned adverse reactions exceeding grade 3, and these adverse reactions were all due to the use of apatinib or immune checkpoint inhibitors. As for BACE, the most common adverse reactions included nausea, vomiting, pain, fever, abnormal liver function, and bone marrow suppression. It is worth mentioning that no reports of grade 3 or higher adverse reactions caused by BACE were found in all studies.
Results of sensitivity analysis
To assess the stability of the meta-analysis results, we performed a sensitivity analysis using median PFS and median OS as indicators. After excluding the literature one by one, the obtained results were not significantly affected, which indicated that our findings were highly stable. The detailed results of the sensitivity analysis are presented in Figure 6.

Discussion on publication bias
To explore the potential publication bias in this study, we conducted a publication bias analysis using median PFS and median OS as indicators. The results showed that the funnel plot was asymmetrical, which usually suggests the existence of heterogeneity in the studies. However, further Egger test results revealed the p-values of 0.641 for median PFS and 0.366 for median OS, both exceeding 0.05. This suggests a low likelihood of publication bias in the study. The specific results of the publication bias analysis are detailed in Figure 6.
Discussion
As of 2022, lung cancer will remain the leading malignant tumor in China in terms of morbidity and mortality. 10,35 Due to the atypical symptoms of early-stage lung cancer, most patients are already in advanced stages upon diagnosis, and the success rate of radical surgery is low. 11 The conventional treatment for advanced lung cancer is combined radiotherapy; however, most patients have poor prognosis due to tumor recurrence, chemotherapy resistance, bone marrow suppression, and other adverse effects. 14 In recent years, BACE has become a popular choice for the treatment of advanced lung cancer, especially for patients with advanced NSCLC who have relapsed, refractory, or refused chemotherapy after standard treatment. 29,36 –41
The mechanism of BACE is that it utilizes bolus microspheres to slowly and steadily release chemotherapeutic drugs, ensuring that high drug concentrations are maintained inside the tumor, typically 2–6 times higher than those administered intravenously. 42,43 In addition, these drugs are able to re-enter the tumor through the blood circulation to administer secondary chemotherapy. 25 At the same time, given that the main blood supply artery for lung cancer is the bronchial artery, 44,45 embolic microspheres, after embolizing this artery, can slow down the blood flow and reduce the inflow of chemotherapeutic drugs into the circulation and nontarget tissues, thus prolonging the residence time and duration of action of the drugs in the vascular bed of the tumor, 46 further inhibiting the transmembrane ion pumps and enhancing the uptake of chemotherapeutic drugs by tumors, 47 thus enhancing the chemotherapeutic effect of chemotherapy while embolizing the arteries of the tumor’s blood supply. 42,46 –48
The study by Bie et al. showed that the application of drug-loaded microspheres for the treatment of NSCLC demonstrated some efficacy with median PFS of 8.0 months and median OS of 16.5 months. 36 This study showed that BACE treatment for patients with advanced NSCLC had a significant prolongation of median OS and median PFS. Further subgroup analysis revealed that the median OS and median PFS of BACE combination therapy were significantly longer compared with BACE monotherapy, which may be attributed to the following factors: on the one hand, the embolization of the tumor blood supply artery by BACE may cause local ischemia and hypoxia of the tumor, but it may also promote the formation of new blood vessels in the peripheral tissues of the tumor, which may lead to the recurrence of the tumor; on the other hand, the targeted therapy combination selectively binds to the ATP site on intracellular vascular endothelial growth factor receptor-2, which subsequently inhibits tumor neovascularization. 49 And then, MWA or 125I seed implantation can directly inactivate most of the tumor tissues, 31 and BACE continuously releases loaded chemotherapeutic drugs through microspheres and embolizes the tumor-supplying arteries to reduce collateral circulation and enhance the synergistic anticancer effect on residual tumor tissues.
In a previous study, He et al. conducted a comparison of the efficacy and safety of DEB-BACE versus PVA-BACE in treating patients with advanced squamous lung cancer who had failed systemic therapy demonstrated that DEB-BACE significantly extended OS and PFS without increasing the incidence of adverse effects compared to PVA-BACE. 27 However, in the present study, DEB-BACE’s median OS and median PFS were slightly shorter than those of other embolic materials, which is inconsistent with the results of the above studies. Possible reasons include: (1) the present study was a meta-analysis of single-group rate, and there were differences in baseline data such as tumor stage, tumor size, age, and Eastern Cooperation Oncology Group score of patients included in different studies; (2) the limited number of controlled studies on various embolization materials means that the results of the subsequent subgroup analyses may lack accuracy; (3) most of the literature included had an insufficient follow-up period, and a large number of patients were still at the end of the follow-up period survived, which may have had an impact on the results of the subgroup analyses. No serious adverse reactions related to BACE occurred in all included studies, demonstrating the safety of this treatment method.
In addition, a study pointed out that in the case of combined hemoptysis in patients with intermediate and advanced lung cancer, especially in central squamous lung cancer, the risk of sudden fatal hemoptysis is much higher than that of other lung cancer types due to its tendency to form cavities. 50,51 For lung cancer patients with hemoptysis, BACE can not only effectively stop hemoptysis but can also significantly enhance the antitumor effect so as to achieve etiological treatment. 52 The study further indicated that BACE showed better efficacy in treating squamous lung cancer than other types of lung adenocarcinoma. 30 Xu and Lin showed that BACE treatment of patients with standard treatment-refractory/ineligible NSCLC significantly prolonged patients’ median OS without increasing the incidence of adverse events. 53,54 Therefore, BACE has undoubtedly become a reliable choice for all types of lung cancer treatment, and its reusable nature allows it to be flexibly combined with other therapeutic means to jointly achieve better therapeutic effects. However, despite the promising application of BACE in the treatment of lung cancer, there is still no conclusion about the selection of its optimal embolic material. The solution to this problem requires more in-depth and detailed studies to further explore and validate.
Limitations of this study: (1) There is still a lack of clinically relevant RCTs, and most of the included studies were non-RCTs, single-arm trials, with a large degree of interstudy heterogeneity, and the heterogeneity did not decrease significantly after subgroup analysis based on the interventions, and it is important to consider that the heterogeneity may arise from the differences in sample size, age of the included patients, disease stage, previous treatment, etc.; (2) the sample sizes of the included studies were restricted, and the overall quality of the evidence was somewhat lacking. Variations in sample size, patient age, disease stage, and prior treatments across studies necessitate cautious interpretation and generalization of the findings; (3) the results of the meta-analysis of the single-group rate were descriptive results, not results of the difference in the comparisons, and the significance of the sensitivity analyses and the publication bias analysis have limited significance; (4) due to the short follow-up time of the included studies, the presence of patients still alive at the end of the follow-up period complicates the accurate assessment of the long-term effects of this treatment approach. Therefore, there is currently uncertainty regarding the long-term benefits of BACE for lung cancer, which may lead to an underestimation of its actual effectiveness. Longer follow-up and further detailed studies are essential to fully grasp the efficacy of BACE in treating lung cancer; (5) not all studies covered all endpoints of interest, and such omissions could be a potential source of bias and thus mislead the results of our analyses. To minimize the impact of this problem, we took active steps to maximize endpoint data collection for each study. This included a deep dive into existing data and attempts to reproduce Kaplan–Meier curves by means of digital reconstruction. In this way, we aim to gain a more complete picture of the endpoints in each study, which will allow us to more accurately assess treatment efficacy and reduce bias due to missing data. Therefore, the conclusions obtained in this study need to be further verified by more high-quality and large-sample clinical studies.
Conclusion
In conclusion, BACE, as a localized treatment, has demonstrated excellent results in the field of lung cancer treatment. Its remarkable therapeutic effect is not only reflected in the effective control of tumor but also in the prolongation of patients’ survival and significant improvement of their quality of life. At the same time, BACE also shows good safety, effectively reduces complications and adverse events during the treatment process, and brings a safer and more reliable treatment option for patients. Therefore, BACE is undoubtedly a superior treatment for patients with NSCLC and is expected to bring better prognosis and quality of life to more patients.
Future Prospects
The future of BACE in lung cancer treatment is promising but requires further exploration. Advancements in both technique and material selection will be critical to optimizing outcomes. Future research should focus on larger, RCTs to overcome current limitations, such as small sample sizes and study heterogeneity, and to confirm the long-term efficacy and safety of BACE. Comparative studies on different embolic materials and their combinations with other therapeutic approaches could offer deeper insights into achieving optimal clinical results. Extending follow-up periods will be vital for accurately assessing the sustained benefits of BACE and refining patient selection criteria. By addressing these research gaps, we can better tailor BACE to individual needs, ultimately enhancing survival rates and quality of life for lung cancer patients.
Footnotes
Authors’ Contributions
Conception and design of study: T.W.; Drafting of article: J.W. and Y.X.
Data Availability
All data produced or analyzed in this study are contained within the published article, with referenced sources listed in the References section.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was received for this article.