
Abstract
Purpose:
Differentiating purely viral from bacterial etiologies continues to be a challenging yet key step in the management of community-acquired pneumonia (CAP), further highlighted since the COVID-19 pandemic. This study aims to evaluate the utility of 99mTc-ubiquicidin (UBI) in the differentiation of bacterial from nonbacterial pneumonia.
Methods:
A total of 30 patients with CAP were allocated into groups A, bacterial (n = 15), and B, viral pneumonia (n = 15). All patients underwent 99mTc-UBI scan with planar and
Results:
UBI scan was positive in 43.3% (n = 13) of patients, with sensitivity, specificity, and accuracy of 86.7%, 100%, and 93.3%, respectively, and close correlation with chest CT scan and PCR results (p-value = 0.000). Planar images were generally not helpful. Receiver operating characteristic curve analysis indicated similar diagnostic performance for 30-min and 3-h SPECT images by implementing T/B thresholds of 1.2 and 1.33, respectively.
Conclusions:
99mTc-UBI SPECT is a promising modality for differentiating purely viral from bacterial or superimposed bacterial pneumonia and provides reliable evidence either to mandate or withhold administration of antibiotics in patients with CAP.
Introduction
Pneumonia is one of the most common causes for hospitalization worldwide, with an annual recording of 450 million cases according to the WHO and responsible for an annual death of about 4 million patients. Community-acquired pneumonia (CAP) affects about 200 million people per year, equally affecting children as well as adults on the global scale, a number presumed to underestimate its true incidence rate as only cases leading to hospitalization are documented. These numbers clearly rise during times of pandemic, such as the recent COVID-19 pandemic. Pneumonia may be caused by sterile inflammation or be of a viral, bacterial, or fungal origin. Molecular diagnostic tests, especially PCR, have further highlighted the role of viruses in pneumonia. 1 –3 Viruses are the putative causative agents of pneumonia in about one-third of adults 3 and more than half of pediatric patients. 4 Bacteria may be the primary cause of pneumonia, exist as a coinfection, or be superimposed on viral pneumonia. Differentiation of purely viral from bacterial ± viral pneumonia drastically affects the management as bacterial pneumonia mandates administration of complex antibiotic regimens. 3,5 In practice, differentiation is primarily based on the physician’s clinical judgment, which takes into account a variety of factors, including the presence of viral epidemics in the community, the patient’s age, symptoms, the speed of onset, results from paraclinical tests such as biomarkers and radiographical changes, and ultimately, the patient’s response to treatment. 3
It has become increasingly clear that none of the commonly performed diagnostic tests has sufficient accuracy on its own to distinguish bacterial from purely viral pneumonia. For instance, PCR has been reported to have merely 60%–71% sensitivity for diagnosing COVID-19 infection compared with chest computed tomography (CT) scans. In addition, it cannot rule out a simultaneous bacterial infection. 6 Procalcitonin (PCT) (with a 0.5 ng/mL cutoff) has been reported to have a sensitivity of 68% and a specificity of 60% for diagnosing bacterial pneumonia in children. 7 Chest CT scan has high sensitivity for diagnosing pneumonia. However, the overlap between the presentation in typical viral, COVID-19, and bacterial pneumonia—especially in the early stages of the disease—significantly limits its specificity. 8 –10 CT scans have been reported to have relatively low specificity (45%–67%) for diagnosing COVID-19 pneumonia, 11,12 with one study reporting specificity as low as 25%. 6 The incidence of superimposed bacterial pneumonia ranges is reported 1% and 7% for patients with influenza pneumonia during the nonpandemic and 2009 pandemic years, respectively. 13,14 During the COVID-19 pandemic, superimposed bacterial pneumonia was detected in 16% of patients. However, the frequency of empirical antibiotic therapy was disproportionately high, performed in 60%–100% of patients with COVID-19 pneumonia, further emphasizing the need reliable diagnostic modalities. 13,14 Till present date, no consensus has been reached on a clinical algorithm to clearly distinguish the cause of pneumonia, neither on whether patients with obvious viral CAP require empirical antibiotic treatments. 3
Ubiquicidin (UBI) is a cationic, synthetic, antimicrobial peptide fragment that binds preferentially with the anionic microbial cell membrane at the site of infection. 15 Technetium-99m ubiquicidin (99mTc-UBI) is bacteria-specific imaging modality successfully implemented in various studies to differentiate bacterial from nonbacterial infections during the past 2 decades, mainly focusing on differentiating bacterial osteomyelitis in diabetic foot or patients with orthopedic devices, 16 –21 recent endeavors have focused on implementing UBI as a PET tracer. 22 –25
To the authors’ knowledge, utility of 99mTc-UBI in differentiating bacterial from nonbacterial pneumonia has not yet been studied. This study aims to evaluate the potential role and accuracy of 99mTc-UBI scintigraphy in differentiating bacterial from nonbacterial CAP with the ultimate goal of improving patient management and reduction of nonbeneficial empirical antibiotic treatments.
Materials and Methods
Patient selection and allocation
This study was approved by the Clinical Research Ethics Committee of the Medical School of Shahid Beheshti Medical University (IR.SBMU.MSP.REC.1403.206). All procedures involving human participants were carried out in accordance with the Declaration of Helsinki as revised in 2013. All patients were interviewed by a nuclear medicine physician and were thoroughly informed about the methods and objectives of this study. Eligible patients were included only after having their oral and written informed consent documented.
This prospective single-center study comprised 35 eligible patients with CAP who were admitted to the Shohada-e Tajrish medical center during 2022–2023. Five patients had to be excluded from the study due to early discharge before completing paraclinical tests, as they chose to receive outpatient care or continue treatment at another hospital of their choice. The available background data, including age and gender distribution, socioeconomic status, and the constellation and severity of symptoms, did not differ from those of the included patients. None of these patients was immunocompromised or had any unusual comorbidities. Therefore, the authors believe that the exclusion of these patients will not impact the study’s generalizability.
Of the remaining 30 patients, all underwent 99mTc-UBI scintigraphy of chest before administration of any antiviral and antibiotic medication, the procedure of which will be explained in the following section. Chest CT scan, COVID-19 nasopharyngeal swab PCR, and laboratory tests, including serum PCT, were performed for all patients during their admission in the pulmonology ward. Patients diagnosed with bacterial pneumonia, regardless of suspicion of coexisting viral etiology, were allocated into group A, and patients with nonbacterial pneumonia into group B. Diagnosis was based on the clinical judgment of the pulmonologist in charge of the patient, accounting for patient’s medical history, clinical examination, and all available paraclinical data except for the UBI scan.
Acquisition protocols and image processing
All 99mTc-UBI kits underwent thin-layer chromatography, and radiochemical purity > 95% was deemed acceptable for utilization. Following IV administration of 555 MBq 99mTc-UBI, imaging of chest was performed at 30 min and 3 h postinjection with the patient lying supine. Images were acquired with a variable-angle, dual-head Evo-Voxel Siemens gamma camera with low-energy high-resolution collimator, 140 Kev photopeak setting, symmetrical width energy window of 10%, 64 × 64 matrix; including planar (anterior and posterior view, 2-min duration) and SPECT images (128 projections; 25 s/projection, noncircular orbit). Images were processed by a single board-certified nuclear medicine physician, blinded to patient allocations. Hand-drawn regions of interest (ROI) were set on any region within the thorax (expected location of lung parenchyma) with visually discernible uptake. Identical size and shape ROIs were placed on the same location on the contralateral lung, representing the background count. The target-to-background (T/B) ratios were calculated based on mean count per pixel value. Values equal or above 1.4 on either time point images of a patient were defined as positive for UBI uptake, hence the presence of bacterial infection (Fig. 1). With respect to lack of any prior studies assessing UBI in lung parenchyma, this empirical threshold was chosen based on the findings of a study assessing the utility of 99mTc-UBI in vertebral osteomyelitis, which suggested this threshold as the most accurate based on receiver operating characteristic (ROC) curve analysis. 26
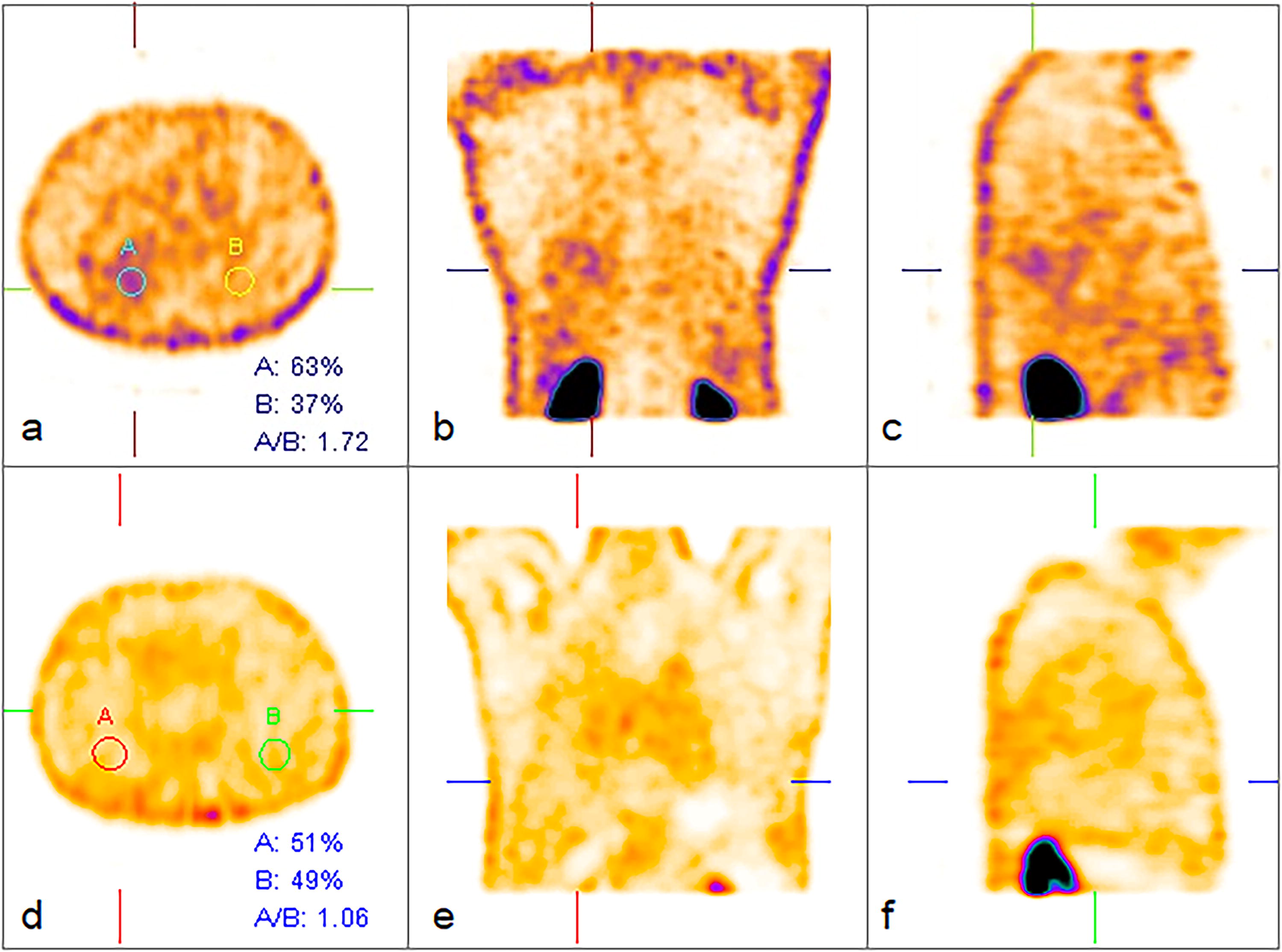
99mTc-UBI SPECT slices of thorax at 3 h postinjection. Identical size and shape regions of interest were placed on any lesion with visually discernible uptake within the lung parenchyma as well as the unremarkable contralateral lung. Target-to-background uptake ratios were calculated based on mean count per pixel values. Slices
Statistical analysis
Quantitative and categorical or qualitative data were represented by mean, standard deviation (SD), and numbers/percentages, respectively. The Mann–Whitney U test was utilized to determine the statistical differences between the two groups of bacterial pneumonia and nonbacterial pneumonia patients. Pearson χ2-square test was implemented to assess the correlation between the results of CT scan, PCR, and UBI scan. A p-value of <0.05 was considered significant. ROC curve analysis was performed to determine the most accurate cutoff for UBI T/B uptake ratios on 30 min and 3 h images.
Results
Thirty patients with CAP, consisting of 21 males (70%) and 9 females (30%), were categorized into groups A, diagnosed with bacterial pneumonia (n = 15), and B, diagnosed with nonbacterial pneumonia (n = 15). The demographic, clinical, and laboratory characteristics of the participants are presented in Table 1. Age and gender distribution had no statistically significant difference among the groups (p-value > 0.05).
Baseline Characteristics of Patients
The statistically significant P-values (<0.05) are bolded.
BUN, Blood Urea Nitrogen; Cr, Creatinine; CRP, C-reactive protein; ESR, Erythrocyte Sedimentation Rate; HCT, Hematocrit; Hgb, Hemoglobin; LYMPH, Lymphocyte; NEUT, Neutrophil; PLT, Platelet; PT, Prothrombin Time; PTT, Partial Thromboplastin Time; RBC, Red Blood Cell; WBC, White Blood Cell.
The red blood cell count, hematocrit, serum PCT levels, D-dimer, and ferritin levels were significantly higher in group A (p-value < 0.05). The erythrocyte sedimentation rate (ESR) was significantly higher in group B (p-value = 0.033). C-reactive protein, white blood cell count, and lymphocyte percentage were also higher in group B, but the difference was not statistically significant (p-value > 0.05).
UBI scan results were significantly correlated with the diagnosis of patients (p-value = 0.000). UBI scan was positive in 43.3% (n = 13) and negative in 56.7% (n = 17) of patients, with sensitivity, specificity, and accuracy of 86.7%, 100%, and 93.3%, respectively. UBI scan results were also significantly correlated with both chest CT scan and PCR results (p-value = 0.000). All patients with positive UBI scan had congruent findings suggesting bacterial pneumonia on CT scan, while 3 of the patients with negative UBI scan had findings suggesting bacterial pneumonia based on CT scan (Table 2).
Ubiquicidin Scan Results Were Closely Correlated with Both Computed Tomography Scan Results and Polymerase Chain Reaction Results (p-value = 0.000)
Of the 13 patients with positive UBI scan, all had congruent CT scan and expectedly negative PCR results. Of the 17 patients with negative UBI scan, 3 had CT scans in favor of bacterial pneumonia and 4 had negative PCR results.
CT, computed tomography; PCR polymerase chain reaction; UBI, ubiquicidin.
Planar images were commonly not reliable in accurate interpretation of UBI uptake, as even in patients with significant, focally high T/B ratios on SPECT images, the planar images could either be unremarkable or the activity in lungs was too smeared to be able to accurately localize a lesion (Fig. 2).
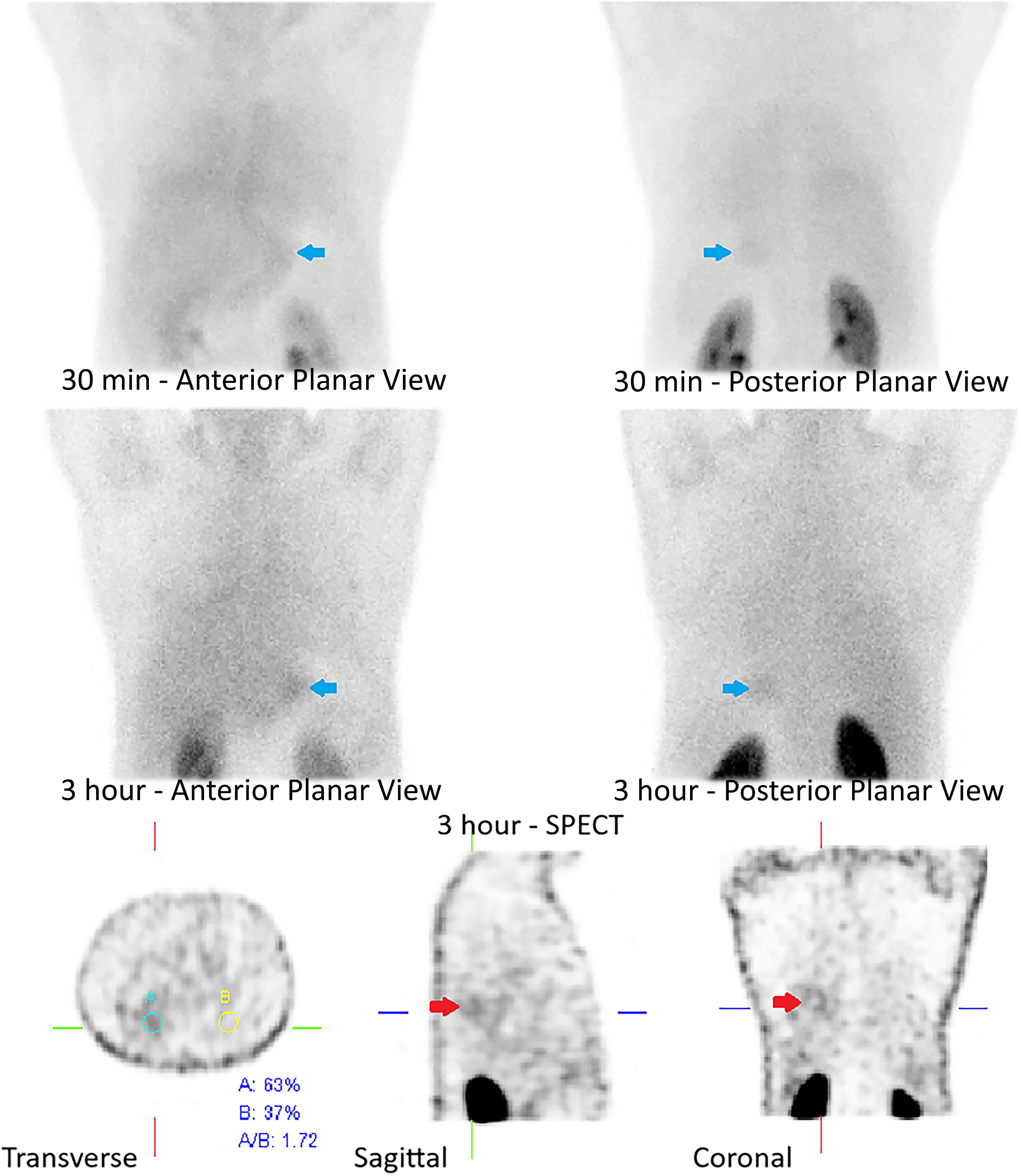
99mTc-UBI planar and SPECT slices of a patient from group A (diagnosed with bacterial pneumonia). As seen, the focus of tracer accumulation about the posterior aspect of right lung lower lobe (T/B = 1.72), which is better appreciated in sagittal and coronal slices (red arrows), is barely evident in planar images, visualized as an ill-defined haziness that cannot be delineated. Of incidental note is uptake of gastric mucosa (blue arrows), which may be caused by the presence of free technetium. The SPECT slices can differentiate the gastric fundus uptake in posterior view from a left lung posterior basal segment uptake. UBI, ubiquicidin; T/B, target to background.
T/B ratios were expectedly higher at 3 h versus 30 min, due to wash out of background blood pool. ROC curves of 30-min and 3-h images are demonstrated in Figure 3. The area under the curve is slightly higher for 30 min (0.951 vs. 0.924). Coordinates of the curves indicate that the most accurate cutoff values for T/B ratio at 30 min and 3 h are 1.2 and 1.325, respectively, both resulting in 86.7% sensitivity and 100% specificity.

ROC curve for Tc-UBI SPECT at 30 min and 3 h postinjection. ROC, receiver operating characteristic; UBI, ubiquicidin.
CT scan results were significantly correlated with the diagnosis of patients (p-value = 0.000). CT scan was in favor of bacterial pneumonia in 53.3% (n = 16) and viral pneumonia in 46.7% (n = 14) of patients. With regard to diagnosing bacterial pneumonia, it had a sensitivity, specificity, and an accuracy of 93.3%, 86.7%, and 90.0%, respectively.
Nasopharyngeal swab PCR results were significantly correlated with the diagnosis of patients (p-value = 0.000). PCR was positive in 43.3% (n = 13) and negative in 56.7% (n = 17) of patients. With regard to diagnosing COVID-19 pneumonia, it had a sensitivity, specificity, and an accuracy of 80.0%, 93.3%, and 86.7%, respectively. For leading to diagnosis of bacterial pneumonia, it had a sensitivity, specificity, and an accuracy of 93.3%, 80.0%, and 86.7%.
Discussion
CAP is one of the most common causes of hospitalization worldwide, affecting both children and adults. Viruses are responsible for about one-third of adult and over half of pediatric cases. Bacteria can be the primary cause, coexist with viral infections, or complicate viral pneumonia. Distinguishing between bacterial and nonbacterial pneumonia is crucial for treatment, as bacterial pneumonia requires a complex antibiotic regimen. While superimposition of bacterial pneumonia on viral pneumonia is relatively uncommon, administration of empirical antibiotic medication is disproportionately high. In practice, differentiation largely relies on the physician’s clinical judgment, taking into account patient’s available clinical and paraclinical data. 1 –5,13,14,27 To date, there is no agreed-upon clinical algorithm for definitive determination of the etiology of pneumonia, nor is there consensus on whether patients with suspected viral CAP need empirical antibiotic treatment. 3 This study indicates that 99mTc-UBI SPECT of thorax is a promising tool in the approach to CAP, which can differentiate primary or superimposed bacterial from nonbacterial pneumonia with sufficient accuracy, providing reliable evidence either to mandate administration of antibiotics or to enable withholding such treatment in patients with CAP.
To the authors’ knowledge, no previous study has evaluated the performance of 99mTc-UBI in diagnosis of bacterial pneumonia. These findings indicate a sensitivity, specificity, and an accuracy of 86.7%, 100%, and 93.3%, respectively. UBI scan was negative in 2 out 15 patients with diagnosed bacterial pneumonia, this may have been caused by small lesion size/low infectious burden, recent use of antibiotic medication, nonbacterial inflammation of background lung parenchyma (decreasing T/B ratio and lesion contrast), and smearing of activity caused by irregular breathing pattern or repeated coughs during SPECT. These findings are concordant with the reported efficiency of UBI scan in diagnosis of bacterial infection in other body tissues/organs, which have mostly focused on the musculoskeletal system. 19,28 –30 Sathekge et al. studied the 99mTc-UBI planar and SPECT/CT scans of 184 patients with suspected musculoskeletal infection. They reported a sensitivity, specificity, and an accuracy of 95.0%, 74.3%, and 86.9% for planar + SPECT-only imaging versus 99.0%, 94.5%, and 94.5% for SPECT/CT, respectively. 28 A study, including 20 patients with suspected osteomyelitis due to diabetic foot ulcers, inflammation at the site of prosthesis, or bone fractures, reported 100% accuracy for 99mTc-UBI scan, versus 90% and 75% for a three-phase bone scan and magnetic resonance imaging, respectively. 19 Another study, including 122 patients with diabetic foot ulcers and histopathological correlations, reported 94.6% sensitivity, 88.9% specificity, and overall, 94.2% diagnostic accuracy of 99mTc-UBI (29–41) SPECT/CT for detection of osteomyelitis. 29
The authors observed that planar images were not reliable enough and SPECT of thorax was indeed necessary for accurate interpretation. SPECT enabled detection of smaller lesions and assisted in better delineation of the infected pulmonary parenchyma, significantly improving the diagnostic sensitivity. This finding is more pronounced but still concordant with prior studies, which assessed the diagnostic performance of UBI scan in postcardiac surgery mediastinitis 31 and 99mTc-HMPAO-labeled leukocytes in poststernotomy sternal infections. 32 The limitations of planar imaging in this context may be explained by the pathophysiology of bacterial pneumonia, which involves exudative inflammation in the lung parenchyma and alveolar spaces, where pathogens are found in the serous exudate within the alveoli. Given the spatial distribution of alveoli, the focal bacterial density in infected lung tissue is likely lower compared with other infections, such as osteomyelitis, causing ill-defined and hazy uptakes on planar images and emphasizing the need for SPECT for accurate interpretation. 33
The authors observed a slightly higher area under ROC curve for 30 min versus 3 h images (0.951 vs. 0.924). The curve coordinates indicated that the most accurate cutoff values for the T/B ratio at 30 min and 3 h are 1.2 and 1.325, respectively, both resulting in 86.7% sensitivity, 100% specificity, and 93.3% accuracy. As one may have noticed, the authors acquired the exact same diagnostic performance results with their empirically applied T/B threshold of 1.4, which is justified by two simple reasons. They defined a scan positive for bacterial pneumonia even if the T/B threshold was only met on the 3 h images, and thus, the generally lower ratios of 30 min images did not impact their results. As for the 3 h images, the small sample size led to lack of any T/B ratios between 1.325 and 1.4 at this time point; therefore, despite applying a higher empirical T/B ratio, the authors acquired a similar diagnostic performance. Nevertheless, their findings suggest that applying an appropriate threshold for 30 min images resolves the necessity for delayed imaging. There is currently no consensus on the optimal time window for imaging in 99mTc-UBI scan. Prior studies have reported that uptake at the infection site seems to peak around 30 min, 28 but interpretation might be facilitated at later time points due to the lower blood pool activity. 34
These findings revealed a strong correlation between findings of UBI and CT scan. In comparison between the two modalities for diagnosis of bacterial pneumonia, the UBI scan was more accurate (93.3% vs. 90%), by having a lower sensitivity (86.7% vs. 93.3%) but a significantly higher specificity (100% vs. 86.7%). These results are concordant with studies focusing on the performance of chest CT scan in differentiating COVID-19-related pneumonia from other causes of viral and nonviral pneumonia, which have shown acceptable sensitivity (76.25%–90%) but low-to-moderate specificity ranging from 45% to 67% of CT scan on this matter. 11,12 The overlap between the ground-glass opacities seen in typical viral, COVID-19, and bacterial pneumonia—especially in the early stages of the disease which may not conform to typical distribution pattern—has been reported to significantly limit the specificity of chest CT scan. 8 –10 Typical COVID-19 pneumonia is bilateral, diffuse, and more peripheral, while segmental or lobar pneumonia is the classical pattern in primary Streptococcus pneumoniae pneumonia. Nevertheless, bacterial pneumonia may also appear diffuse based on age, clinical setting, and underlying conditions such as chronic obstructive pulmonary disease (COPD), diabetes, and smoking. In addition, superimposed bacterial infection in the context of existing or healing viral pneumonia may not conform to any typical pattern. 35 –38
The authors found a strong correlation between the results of UBI scan and nasopharyngeal swab PCR. With regard to diagnosing COVID-19 pneumonia, PCR had a sensitivity, specificity, and an accuracy of 80.0%, 93.3%, and 86.7%, respectively, emphasizing a rather low specificity for diagnosing bacterial pneumonia based on a negative PCR (80% vs. 100% for UBI and 86.7% for chest CT scan). These findings are concordant with prior studies on this matter, indicating a low sensitivity (60%–71%) in diagnosing patients with COVID-19 infection compared with the chest CT scan. 6,39,40
As previously described, the authors observed a significant difference in the level of several acute-phase reactants among the two groups, such as higher serum PCT, D-dimer, and ferritin levels in group A and higher ESR levels in group B. However, as recent studies consistently suggest, none of these parameters, including PCT—once believed to be specific to bacterial infections—is truly specific for distinguishing between bacterial and viral pneumonia but mostly reflect the severity of the infection. 41 –43
Study limitations
This study has limitations that should be acknowledged. As with most research evaluating the diagnostic efficacy of a modality in distinguishing bacterial from nonbacterial pneumonia, selecting a definitive diagnostic standard has been challenging. The gold standard—obtaining pathological confirmation via bronchoscopy—is seldom performed due to its invasive nature, high cost, and time constraints. Consequently, in this study, patient classification was based on the final assessment of the referring clinician, who considered all available clinical data, laboratory results (including PCR), and chest CT scans. Another limitation would be that despite the study taking place in the middle of the COVID-19 pandemic, the possibility of presence of other purely viral pneumonias among the patients cannot be fully excluded, which may have affected the diagnostic performance of nasopharyngeal swab test. The authors did not account for all confounding factors that may have affected the results, such as history of COPD or other interstitial lung disease (higher background blood pool), or recent use of antibiotics before admission, which as discussed before may negatively affect the sensitivity of UBI scan. In addition, the small sample size is relatively small, limiting the reliability of the proposed T/B cutoffs. Future studies with larger sample size and preferably hybrid SPECT/CT systems would be required to evaluate the diagnostic accuracy of 99mTc-UBI in differentiating bacterial from nonbacterial pneumonia.
New knowledge gained
To the authors’ knowledge, this is the first study that: Evaluated the diagnostic performance of 99mTc-UBI in differentiating bacterial from nonbacterial pneumonia. Acquired both planar and SPECT images of thorax at two separate time points. Suggested the most accurate T/B cutoff for each time point.
Conclusions
Distinguishing between pure viral and bacterial causes of CAP remains a crucial and challenging aspect of its management, a difficulty that has been further emphasized since the COVID-19 pandemic. Currently, no standardized clinical algorithm exists for definitive determination of the cause of pneumonia, and there is no consensus on whether patients with suspected viral CAP require empirical antibiotic treatment. This study demonstrates that 99mTc-UBI SPECT of the thorax, even at 30 min postinjection, is a promising tool for managing CAP. It can accurately differentiate bacterial (primary or superimposed) from nonbacterial pneumonia with fair sensitivity and perfect specificity, thus providing reliable evidence to guide the decision to administer or withhold antibiotics in these patients.
Footnotes
Acknowledgment
The authors express their appreciation to all the patients who graciously participated in this study.
Authors’ Contributions
All authors have made substantial contributions to the conception, design, as well as acquisition of patient data; have been involved in drafting and revising the article; have given final approval of the version to be published, with each of them having participated sufficiently in the work to take public responsibility for appropriate portions of the content; and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethics Approval Statement
This study was approved by the Clinical Research Ethics Committee of the Medical School of Shahid Beheshti Medical University (Trial registration number: IR.SBMU.MSP.REC.1403.206). All procedures involving human participants were carried out in accordance with the Declaration of Helsinki as revised in 2013. This article does not contain any experiments on animals.
Disclosure Statement
Except G.N., all authors are employed by Shahid Beheshti University of Medical Sciences, School of Medicine, which primarily focuses on education and medical research. The authors have no other conflict of interest to disclose. All authors confirm that this research is supported by Shahid Beheshti University of Medical Sciences, School of Medicine.
Funding Information
No funding was received to assist with the preparation of this article.