
Abstract
Abstract
This prospective clinical case series aimed to investigate the safety and efficacy of suprachoroidal adipose tissue-derived mesenchymal stem cell (ADMSC) implantation in patients with dry-type age-related macular degeneration (AMD) and Stargardt's macular dystrophy (SMD). This study included four patients with advanced-stage dry-type AMD and four patients with SMD who underwent suprachoroidal implantation of ADMSCs. The best-corrected visual acuity (BCVA) in the study was 20/200. The worse eye of the patient was operated on. Patients were evaluated on the first day, first week, and first, third, and sixth months postoperatively. BCVA, anterior segment and fundus examination, color photography, fundus autofluorescence, optical coherence tomography, and visual field examination were carried out at each visit. Fundus fluorescein angiography and multifocal electroretinography (mf-ERG) recordings were performed at the end of the first, third, and sixth months and anytime if necessary during the follow-up. All eight patients completed the sixth month follow-up. None of them had any systemic or ocular complications. All of the eight patients experienced visual acuity improvement, visual field improvement, and improvement in mf-ERG recordings. Stem cell treatment with suprachoroidal implantation of ADMSCs seems to be safe and effective in the treatment of dry-type AMD and SMD.
Introduction
A
The only approved treatment for dry AMD to date is the AREDS combination, which is used for delaying the progression of AMD to the advanced form (Age-Related Eye Disease Study 2 Research Group [AREDS2 Research Group], 2013).
Stargardt's macular dystrophy (SMD) is the most common inherited macular dystrophy in both adults and children with a prevalence of 1 in 8000–10,000. It has an autosomal recessive inheritance mode associated with mutations mostly in the ABCA4 gene. Different mutations can be involved, and the age at onset varies according to the mutations, from childhood to adulthood. It mainly affects young people, often starting in late teens or early 20s. Patients present with bilateral central visual loss, including dyschromatopsia and central scotomata, with characteristic macular atrophy and yellow-white flecks at the level of the RPE at the posterior pole. There is slow progressive loss of retinal function and structure over time.
Although there are currently no proven treatments, there are three main avenues of intervention being explored with human clinical trials of stem cell therapy, gene replacement therapy, and pharmacological approaches (Fujinami et al., 2013, 2015).
Stem cell therapy has been under investigation as a viable alternative in recent years as stem cells have the potential to generate new retinal cells, replace, and heal damaged cells in diseases of the retina. Nonocular-derived stem cells include embryonic stem cells (ESCs), induced pluripotent stem cells (iPSCs), mesenchymal stem cells (MSCs), which include bone marrow MSCs (BMMSCs), and adipose-derived MSCs (ADMSCs). MSCs are generated from developmentally mature organs and have the advantages of trophic support that allows slowing down retinal cell degeneration and immunosuppression, while the disadvantage is the low rate of cell migration and differentiation.
Compared with BMMSCs, ADMSCs have the advantages of easier harvest from donors, faster expansion, more protein secretion, and higher immunomodulatory capacity (Jones et al., 2017; Öner, 2018).
In this study, we aimed to investigate the safety, efficacy, and efficiency of suprachoroidal ADMSC implantation in patients with dry-type AMD and SMD.
Materials and Methods
This is a single-center, prospective, phase 1/2 clinical safety study, including eight eyes of eight patients (four with dry AMD and four with SMD) with irreversible vision loss who were admitted to the Retina and Vitreous Section of the Ophthalmology Department of our medical faculty. In cases of patients where both eyes were eligible for the study, the eye with worse visual acuity was enrolled in the study. The study was approved by the Institutional Review Board of the Medical School of Erciyes University (No: 2017/480, date: October 13, 2017) and conducted in adherence with tenets of the Declaration of Helsinki. Approval by the Review Board of Stem Cell Applications of the Ministry of Health was also obtained according to regulations in Turkey (Review number for approval: 56733164/203).
All patients were individually instructed on the methodology of the study and written informed consent was obtained from all individual participants included. The inclusion criteria were as follows: (1) patients older than 18 years of age, (2) a clinical diagnosis of retinal dystrophy classified as dry AMD or SMD, and (3) best-corrected visual acuity (BCVA) of <20/200.
Patients with previous ocular surgery other than cataract extraction, ocular media opacities that would make the image not of sufficient quality for ocular imaging or affect the mf-ERG or visual field evaluation, coexisting ocular disease (i.e., retinal pathology, glaucoma, uveitis, strabismus, and nystagmus), and any other systemic disease that would affect the results were excluded from the study.
A single experienced vitreoretinal surgeon (A.O.) performed all surgical procedures and ophthalmic evaluations. All patients underwent baseline ophthalmic evaluation, including baseline BCVA, applanation tonometry, slit-lamp biomicroscopy, color fundus photography, optical coherence tomography (OCT), fundus fluorescein angiography (FFA), fundus autofluorescence (FAF) imaging, and mf-ERG. Visual acuity was recorded using a Snellen chart at a distance of 3 m and presented as logarithm of the minimum angle of resolution (logMAR) units.
Fundus photography and FFA were performed using the Zeiss FF 450 (Carl Zeiss Meditec AG, Germany). Spectral-domain OCT was performed using the Heidelberg OCT device (Heidelberg Engineering, Heidelberg, Germany) with a standardized scanning protocol and enhanced depth imaging mode. FAF was carried out using the OCT device. Areas of hypoautofluorescence in the macular region were considered as GA in FAF imaging. The greatest dimension of this hypoautofluorescent area was measured and noted as greatest lesion diameter (GLD) at baseline, and the same operator did FAF imaging for all the patients at each follow-up.
Visual field examination was performed by Octopus Goldmann perimetry (Octopus 900; Haag Streit İnternational, Switzerland). mf-ERG (mf-ERG-Vision monitor, Monpack 3; Metrovision, France) readings were recorded from each eye according to the International Society for Clinical Electrophysiology of Vision (ISCEV) guidelines (Hood et al., 2012).
Surgical technique
All surgeries were carried out with local anesthesia. We performed a surgical technique defined as the Limoli retinal restoration technique (LRRT), described by Limoli et al. (2014). Each eye received a cell graft of ADMSCs between the choroid and sclera.
Isolation and culture of ADMSCs and their flow cytometry analyses were performed as previously mentioned by our study group (Oner et al., 2016).
For platelet-rich plasma (PRP) preparation, 8 mL of human peripheral blood was collected in a Regen-BCT tube (RegenKit; RegenLab, Le Mont-sur-Lausanne, CH). The collected blood was centrifuged for 10′ at 1500 g.
Details of the surgery are as follows: the globe was deviated to the superonasal quadrant and conjunctiva was dissected at the inferotemporal quadrant at 8 mm from the limbus. A deep scleral flap of about 5 × 5 mm was opened by a radial hinge at the inferotemporal quadrant. The sclerectomy was deep enough to allow viewing of the color of the choroid. A flap from the orbital fat was extracted from a gap above the inferior oblique muscle. This tissue was laid on the scleral bed and sutured with 6/0 vicryl at the proximal edge. The scleral flap was then sutured above the fat pedicle. The remaining space between the autologous fat graft, choroid, and scleral flaps was filled with 0.1 cc of 2 × 106 ADMSCs and 1 cc of PRP using a 25-gauge cannula. The conjunctiva was sutured with 8/0 vicryl.
Postoperative follow-up
Patients were hospitalized for 1 day after the surgery and received topical antibiotic and steroid drops four times a day during the first month. Ophthalmic evaluations, including BCVA, anterior and posterior segment examination, color fundus photographs, OCT, and FAF, were performed at day 1, at week 4, and then at months 3 and 6 after the surgery. Perimetry, FFA, and mf-ERG recordings were also obtained before surgery and at months 1, 3, and 6 during the follow-up period.
Results
Morphology and phenotype of culture-expanded ADMSCs
ADMSCs were spindle-shaped cells with a fibroblast-like morphology and they were attached to the plate during cell culture. These cells were found to be efficient according to inhibition of lymphocyte proliferation before releasing. For immunophenotypic characterization of ADMSCs, culture-expanded cells at the third passage were examined for surface protein expression by using flow cytometry. ADMSCs were positive for CD44, CD73, CD90, and CD105 and negative for CD11b, CD34, CD45, and HLA-DR. No evidence of bacterial or fungal contamination was observed in the cells, which were tested before releasing. Cell viability evaluated by trypan blue exclusion was >90.0% ± 0.5 before cell transplantation.
Follow-up BCVA and eye examination
All eight patients completed the 6-month follow-up and none of them had any ocular or systemic complications. All of the patients experienced visual acuity improvement during the follow-up, whereas the untreated fellow eyes of the patients did not show similar improvements. Demographic details and visual acuity of eyes receiving stem cells are shown in Table 1.
Demographic Details and Visual Acuity of Eyes Receiving Stem Cells
AMD, age-related macular degeneration; BCVA, best-corrected visual acuity; logMAR, logarithm of the minimum angle of resolution; OD, oculus dexter; OS, oculus sinister; SMD, Stargardt's macular dystrophy.
Perimetry
All of the subjects showed improvement in visual field and the central visual field defect became smaller on Goldmann perimetry during the follow-up period (Fig. 1).
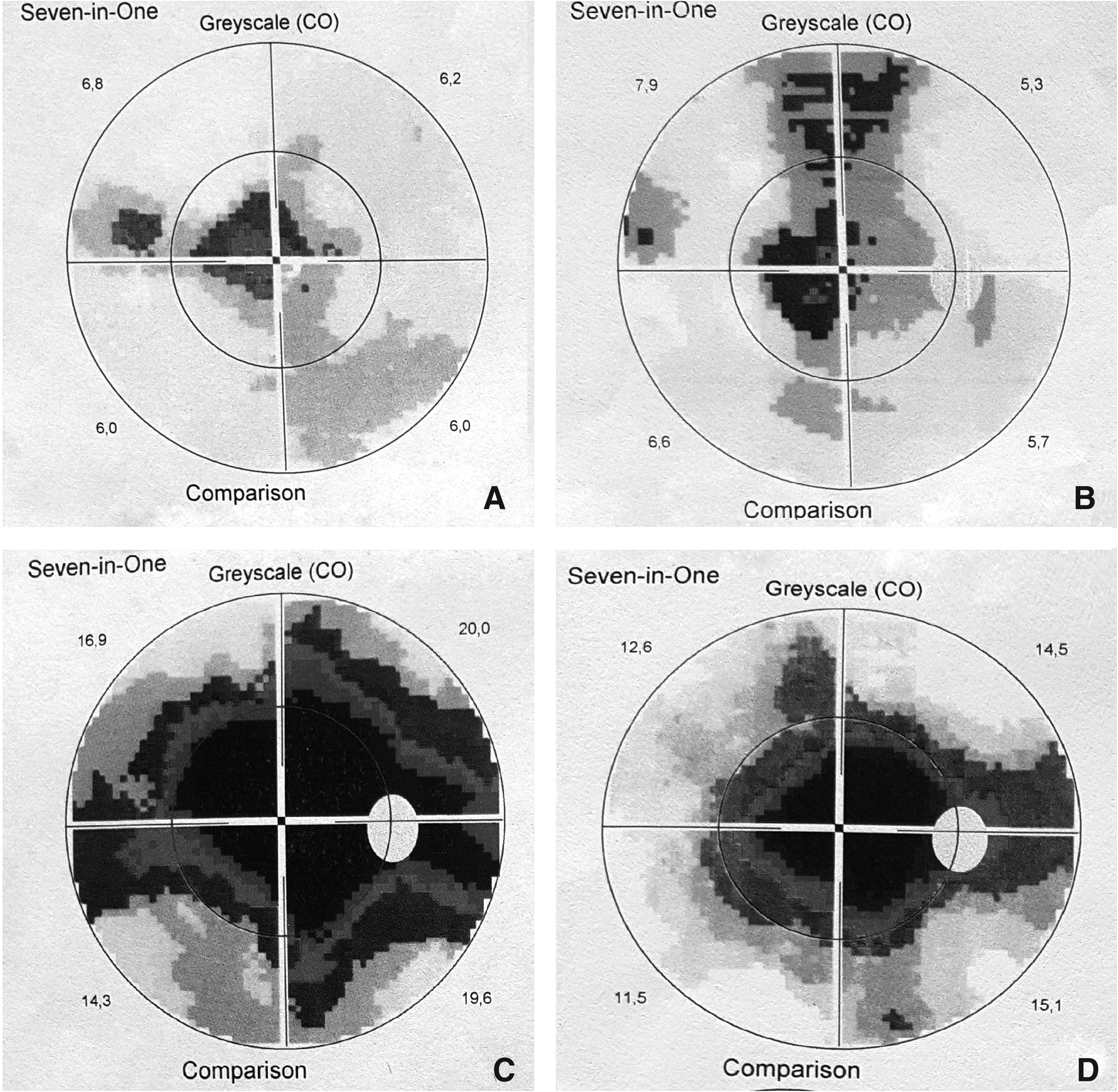
Perimetry results of an AMD subject before treatment
Multifocal electroretinography
Analysis of mf-ERG results showed improvements in amplitudes of the P1 wave over 6 months, especially in the central rings. Implicit times in all the zones showed small decreases (Tables 2, 3 and Fig. 2).
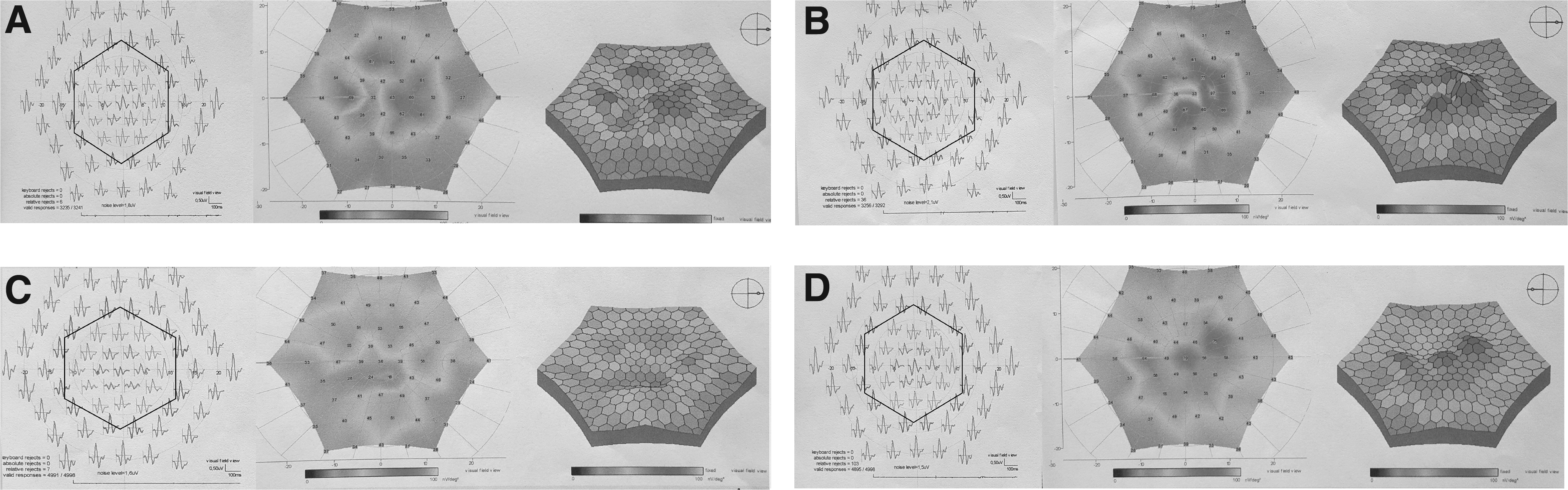
mf-ERG recordings of the same subjects before treatment
Multifocal Electroretinography Amplitude of P1 Wave (Values in Nanovolts)
Multifocal Electroretinography Implicit Time of P1 Wave (Median Values in Milliseconds)
Fluorescein angiography
There was no pathology in FFA of all patients after the treatment. No changes in perfusion and no tumors or neovessels were found following the stem cell (SC) surgery.
OCT findings
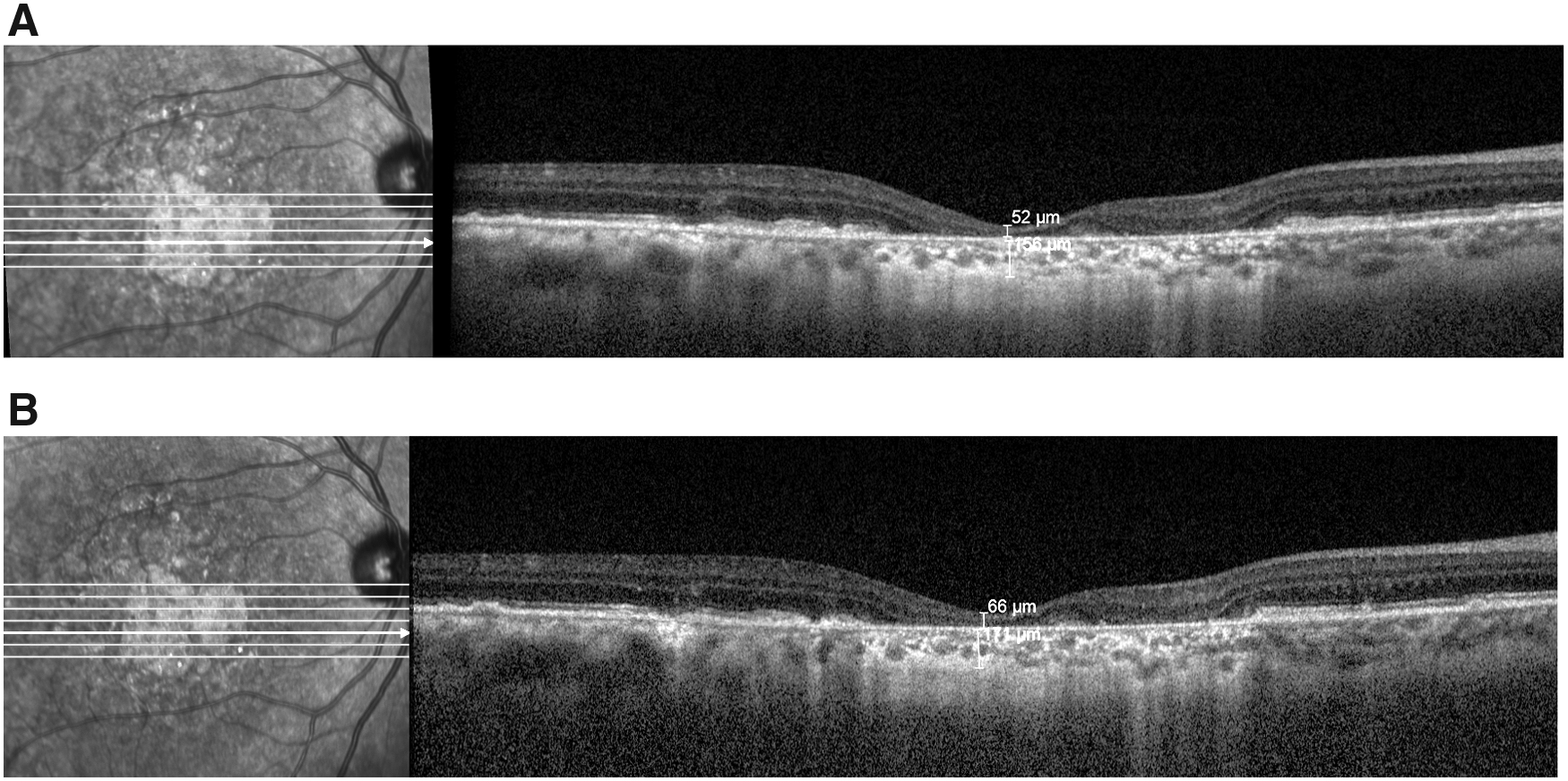
No changes were found in macular thickness or anatomy by OCT at any time point. We found an increase in choroidal thickness measurements of all patients after stem cell treatment (Table 4 and Fig. 3).
Optical Coherence Tomography and Fundus Autofluorescence Measurements of Eyes Receiving Stem Cells (Values in μm)
CCT, central choroidal thickness; CMT, central macular thickness; GLD, greatest lesion diameter.
Fundus autofluorescence
There was a slight decrease in GLD in all patients in the stem cell-treated eye (Table 4 and Fig. 4).

Statistical analysis
The size of the patient population in the study was not sufficient to permit a conclusive statistical analysis.
Discussion
Treatment of dry AMD and SMD poses a challenge as there is no approved therapy available. Knowing the pathology and its limitations, many researchers have looked for therapeutic alternatives, including the use of stem cells (Öner, 2018).
In 2012, Schwartz et al. reported preliminary safety data of human ESCs on one dry AMD patient and one SMD patient. The subretinal transplanted human ESC-derived RPE cells showed no signs of hyperproliferation, tumorigenicity, ectopic tissue formation, or apparent rejection after 4 months (Schwartz et al., 2012). The 22-month follow-up data of this study included nine dry AMD and nine SMD patients. BCVA improved in 10 eyes, improved or remained the same in 7 eyes, and decreased by more than 10 letters in 1 eye, whereas the untreated fellow eyes of the patients did not show similar improvements in visual acuity.
Results of this study provide the first evidence of medium-term to long-term safety, graft survival, and possible biological activity of pluripotent stem cells in individuals with retinal disease (Schwartz et al., 2015). In another clinical study with human ESC-derived RPE cells, the authors reported the safety and tolerability of subretinal transplantation in four Asian patients: two with dry AMD and two with SMD. The patients were followed for 1 year and there was no evidence of adverse proliferation, tumorigenicity, ectopic tissue formation, or other serious safety issues related to the transplanted cells. Visual acuity improved by 9–19 letters in three patients and remained stable in one patient. These results confirmed that human ESC-derived cells could serve as a potentially safe new source (Song et al., 2015).
Some studies have evaluated the trophic effect of autologous hematopoietic stem cells derived from the bone marrow in retinal diseases (Parks et al., 2015; Siqueira et al., 2011, 2015).
In a study by Park et al., six eyes with irreversible vision loss from retinal vascular occlusion, hereditary or nonexudative AMD, or RP received a mean of 3.4 million intravitreal BMMSCs. The therapy was well tolerated with no intraocular inflammation or hyperproliferation; BCVA and full-field ERG showed no worsening after 6 months, and they concluded that intravitreal autologous BMMSC therapy appeared feasible for regenerative medicine (Parks et al., 2015).
In a recent study by Kumar et al. (2017), BMMSCs were used intravitreally in the treatment of 60 advanced dry AMD patients and the effect of stem cell therapy was evaluated in terms of visual acuity, amplitude, and implicit time in mf-ERG and size of GA on FAF imaging. At the 6-month follow-up, although there was no statistically significant improvement in BCVA, mf-ERG showed significant improvement in amplitude and implicit time in the treated group. A significant decrease was also noted in GLD of GA in the eyes receiving stem cells. However, no such improvement was noted in the control group, including the fellow eyes of the patients. Adverse events were not seen in any of the patients. They concluded that electrophysiological and anatomical improvements in the treatment group may indicate the therapeutic role of BMMSCs in dry AMD.
In another study, the authors evaluate the safety and efficacy of intravitreal injections of bone marrow mononuclear fraction containing CD34+ cells in 10 patients with atrophic AMD. Patients were evaluated with tests, including microperimetry, infrared imaging, FAF, FFA, and OCT. Mean BCVA and mean sensitivity threshold improved significantly during the 12-month follow-up period. These results were better in patients with the smallest areas of atrophy. FFA did not identify choroidal new vessels or tumor growth. The authors emphasize that the paracrine effect of CD34+ cells may explain the functional improvement observed (Cotrim et al., 2017).
Limoli et al. (2014, 2016) treated 36 eyes of 25 dry AMD patients with surgically grafted autologous cells, platelets from platelet-rich plasma and ADMSCs to the suprachoroidal space, to achieve constant production of growth factors at the chorioretinal level. The surgical technique was called LRRT. After 6 months, the treatment improved visual performance and the increase was better if retinal thickness recorded by OCT was higher, probably in relation to the presence of areas with greater cellularity. They assumed that a greater number of residual cells leads to greater interaction between growth factors and chorioretinal cellular membrane receptors, more intense cellular activity, and, ultimately, improvement of visual quality.
In the current study, LRRT was used as a stem cell implantation technique. To date, no standardized treatment modality has been proved, including the route of delivery for the stem cells. The transplanted tissue or cells must survive surgical transplantation and should be able to achieve biologically viable anatomic characteristics to effectively replace the diseased tissue.
In the previous study of ours where we performed subretinal ADMSC implantation in advanced-stage patients with RP, we faced various ocular complications, including choroidal neovascular membrane at the site of the implantation and epiretinal membrane around the transplantation site and at the periphery, causing localized peripheral tractional retinal detachment, which needed second surgeries, including vitrectomy and silicon oil injections, and led us to the need for modifying the initial technique (Oner et al., 2016; Oner and Sevim, 2017; Oner, 2018). The suprachoroidal approach has the advantage of delivering the tissue to the retina and RPE, without having to violate the vitreous cavity, therefore reducing related surgical complications as this technique includes no removal of vitreous and no iatrogenic retinal hole (Oner, 2018).
To overcome surgery-related complications, we performed suprachoroidal implantation in this study and we found no systemic or ocular complications during the 6-month follow-up.
There are limitations to our study. We know that the study population is small. Furthermore, the study included patients with poor visual function (who are considered as legally blind), which hindered our ability to perform reliable measurements of visual functions.
In this study, we considered employing two important elements: (1) neurotrophic growth factors (GFs) from ADMSCs to slow down RPE cells and photoreceptor apoptosis and (2) angiotrophic GFs from ADMSCs and PRP for therapeutic purposes to improve choroidal flow. We found improvements in visual performance, visual field, and mf-ERG recordings in the treated eyes at the 6-month follow-up. A decrease was also noted in GLD of GA in the eyes receiving stem cells. Ocular complications were not observed in any of the patients.
We concluded that electrophysiological and anatomical improvements in the treatment group may indicate the therapeutic role of ADMSCs in dry AMD and SMD. In conclusion, stem cell-based treatment modalities have been showing promising results in commonly encountered retinal diseases that currently have no curative treatment options. We believe that in the near future, stem cell therapies will hold an important place in the treatment of degenerative retinal diseases.
Footnotes
Acknowledgment
This study is funded by The Scientific Research Support Division of Erciyes University.
Authors' Contributions
A.O. was involved in study design, patient selection and follow-up, surgical intervention, data collection, and manuscript preparation; Z.B.G. was involved in study design, preparation of stem cells, laboratory tests, and manuscript preparation; D.G.S. was involved in data collection and manuscript preparation; N.S. was involved in data collection and manuscript preparation; and M.U. was involved in study design and manuscript preparation. All authors read and approved the manuscript.
Declaration
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.