
Abstract
Abstract
Background:
A family-based multidisciplinary weight management program for obese children 7–11 years old was implemented by a pediatric weight management center and local YMCA. The purpose of this study was to explore parents' and children's perceptions of the program to gain insight about factors that may enhance engagement and retention of families in weight management treatment.
Methods:
Families were invited to participate in a telephone interview after their participation in the program. The interviews assessed satisfaction with program components, acceptability of the intervention, barriers to treatment participation, and suggestions for improvement.
Results:
A total of 34 semistructured telephone interviews were performed, including 19 parents and 15 children. The majority of children (mean age=9.2±1.5 years) interviewed were female (74%) and recipients of Medicaid (79%). The population was racially diverse (63% black, 26% white, 11% other). Results suggest families were generally very positive about the program and viewed the major components of the program as helpful (i.e., nutrition, exercise, behavior). Families particularly enjoyed exercise and cooking demonstrations, whereas self-monitoring activities and learning about behavior change strategies were less enjoyable. Parents noted that increasing the length of individual sessions would likely be beneficial. Families who did not complete the program cited factors such as transportation barriers (e.g., gas money, distance), scheduling conflicts, and unmet expectations as contributing to their decision to discontinue participation.
Conclusions:
This study may have implications for how to enhance family-based pediatric weight management programs for children ages 7–11 years.
Introduction
Together with the local YMCA, C.S. Mott Children's Hospital implemented a family-based multidisciplinary weight management program for children ages 7–11 years. The purpose of this study was to explore parents' and children's perceptions of the program in order to gain insight about factors that may enhance engagement and retention of families in weight management treatment.
Method
Study Design
Semistructured telephone interviews were performed with parents and children who participated in the Michigan Pediatric Outpatient Weight Evaluation and Reduction (MPOWER) Junior Program. Telephone interviews were performed with parents and children separately between March, 2010, and September, 2010. The interviews assessed for satisfaction with the program's various components and obtained feedback about how to improve the program. This study was approved by the Institutional Review Board of the University of Michigan Medical School, and parental consent and child assent was obtained.
Sample and Recruitment
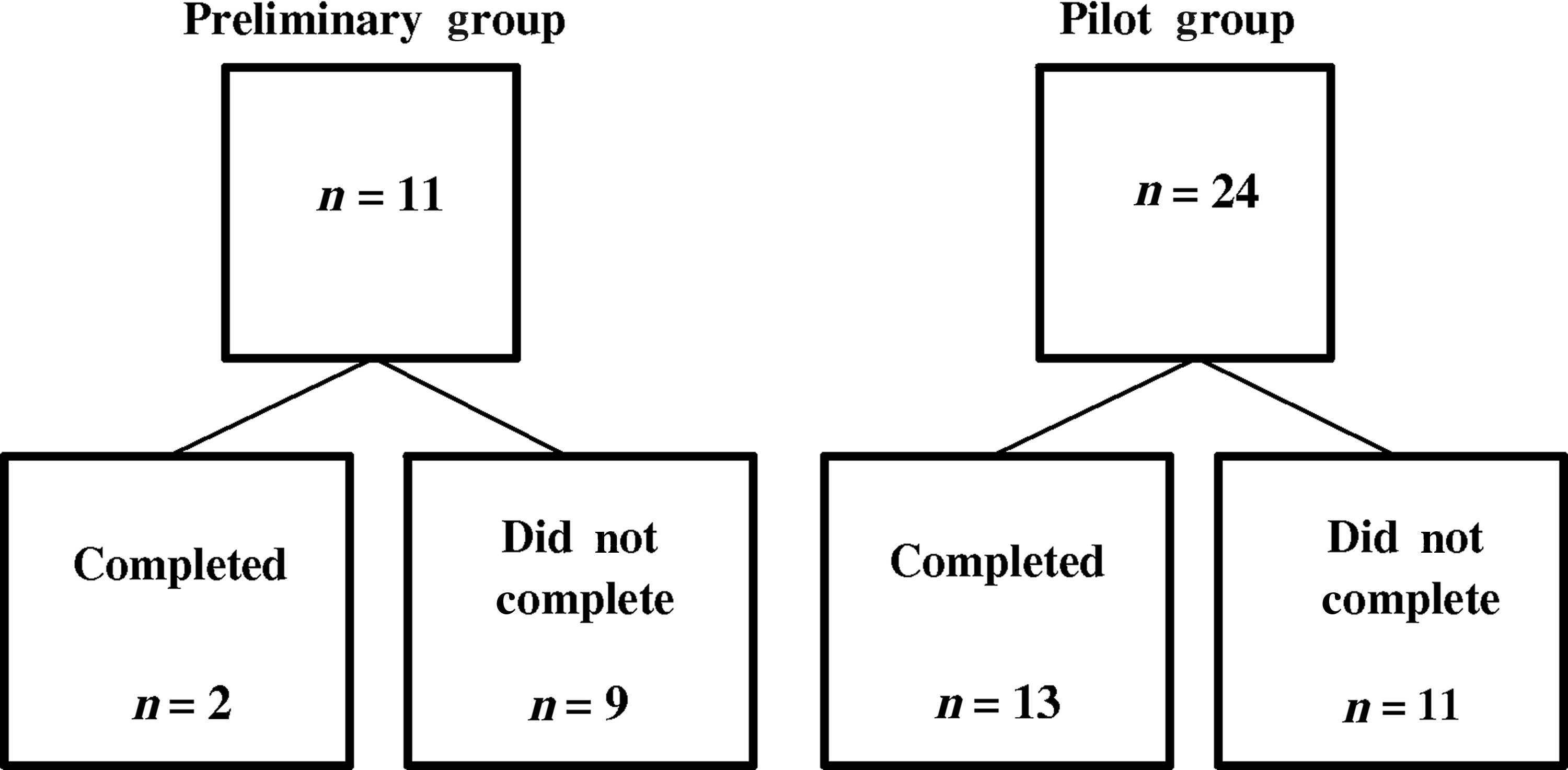
Children and their parents who participated in the MPOWER Junior program between September, 2008, and August, 2010, were eligible and agreed to participate. Children required a referral from their primary care physician and a BMI at or above the 95th percentile for age and sex. Eleven parents in the preliminary group and 24 parents in the pilot group were called to request an interview (please refer to Fig. 1 for sample sizes of completers and noncompleters in each group). Following the parent interview, parents were asked permission to interview their child. If the parent and/or child were willing to participate in an interview, but were unable to complete the interview at the time of the phone call, the interview was scheduled for a subsequent time. Up to three attempts were made to contact parents in an effort to recruit them for this study. A total of 34 interviews were conducted (i.e., completers, 12 parents and 11 children; noncompleters, 7 parents and 4 children).
Program Overview
Prior to implementing and evaluating the pilot group intervention, 11 families enrolled in a similar clinical weight management program offered during the summer of 2008. The families expressed a number of financial concerns and few finished the program. The cost of program participation was based on a sliding scale, with most families not paying anything. However, the costs of transportation and purchasing healthy foods were noted as barriers. Thus, for the pilot intervention, community connections were employed to provide some additional assistance to families. Specifically, through partnerships with a local food bank, families were given the ingredients to prepare the meals demonstrated in the program at home, and the local health department provided tokens for use at a local farmer's market. By partnering with a local grocery store, gas cards were provided for those families that requested them. The program description that follows is for the pilot intervention.
The MPOWER Junior program is a 6-month multidisciplinary weight management program for children 7–11 years old developed and implemented at the University of Michigan in conjunction with the Ann Arbor YMCA. This family-focused program incorporates medical evaluation and monitoring along with nutrition and physical activity educational components. In addition, it incorporates a behavior modification protocol consistent with the expert committee recommendations and built on evidence-based obesity interventions.4,16–18 The MPOWER Junior program focuses on parents as the agents of change.19–22 As such, parents are equipped with knowledge and behavioral strategies to implement healthy habits at home for their families. Rather than providing children with comprehensive education about lifestyle changes, the groups for children aim to prime them for change by exposing them to concepts and healthy behaviors so that they will be more compliant when parents implement specific changes at home. The program is delivered over 24 weeks by a multidisciplinary team of providers including a pediatrician, psychologist, dietitian, social worker, and exercise physiologist.
Families joined the program in monthly cohorts and attended weekly sessions at the Ann Arbor YMCA from 4:30 pm to 6:30 pm. The sessions included the following components:
Exercise
One hour of each visit consisted of an exercise session. For children this involved a variety of group activities such as swimming, yoga, kick boxing, basketball, relay games, and floor hockey. Parents participated in personal training sessions with YMCA staff and joined the group activities with their children once per month. In addition, they received brief presentations about physical activity covering topics such as safety measures for exercise, ways to encourage their families to be more active, and calories burned with various forms of activity. All families were given a free 6-month YMCA membership allowing them to use the facility at any time.
Parent nutrition groups
Monthly 1-hour group sessions included presentations addressing target behaviors for the entire family, such as breakfast consumption, increased consumption of vegetables and fruit, decreased consumption of sweetened beverages, and decreased consumption of fast food.
Parent behavioral groups
Monthly 1-hour behavioral group sessions addressed topics such as self-esteem, eating triggers, core values, planning ahead, parenting techniques, and problem solving. All sessions were aimed at providing parents with skills to assist their families with implementing healthy lifestyle changes.
Individual sessions
Every other week, parents participated in 20-minute individual sessions with one provider. At each individual session, participants set goals related to one of six target behaviors for their child and family: Reduction of screen time, regular consumption of a healthy breakfast, decreased consumption of sweetened beverages, decreased consumption of fast food, increased consumption of fruits and vegetables, and increased physical activity. During these sessions, diet and activity logs were reviewed and contingency plans were made. For the majority of families, only the parents participated in the individual sessions. However, older children (i.e., 10 or 11 years old) were included when requested by their parents.
Cooking demonstrations
On individual session weeks, parents and children also participated in a cooking demonstration together. Families were provided with healthy snacks at all sessions.
Child groups
When parents were meeting in a nutrition or behavioral group, children participated in a separate group for 1 hour. They engaged in activities designed to prime them for making healthy lifestyle changes, including activities to help them recognize healthy food choices and activities to address issues such as self-esteem and problem solving. Children earned points for participation in the activities. These points could then be used to select small prizes at the completion of each session.
Survey Instrument
Interview guides were developed for parents and children in this study and based on a review of the literature and expert opinions of the authors. Additional questions were added for families who did not complete the program to probe for barriers to treatment completion and ideas to facilitate treatment retention. The guides included open-ended questions (e.g., What was the most helpful part of the program?), rating scales (e.g., How would you rate your child's motivation to achieve a healthy weight on a scale of 1 (not at all motivated) to 5 (very motivated)?), and closed-ended questions (e.g., Do you think weekly weight checks are appropriate?). Questions probed for satisfaction with various aspects of the program (e.g., nutrition, exercise, behavioral) and suggestions for improvement. Families were also asked to provide specific feedback regarding the acceptability of time and length of sessions, duration of the program, and YMCA facility.
Data Collection
All interviews were recorded and detailed notes were taken. Interviews lasted from 15 to 45 minutes for parents and from 5 to 15 minutes for children. A total of 34 interviews were completed, including 19 parents and 15 children.
Data Analysis
The analysis was based on grounded theory as described by Strauss and Corbin. 23 Specifically, during open coding, the detailed interview notes were reviewed line by line and categories were developed. Categories were then reduced to themes. Two authors independently coded the transcripts and a third adjudicated differences.
Results
The majority of children (mean age=9.2±1.5 years, BMI=30.3±5.1 kg/m2) interviewed were female (74%) and recipients of Medicaid (79%). The study population was racially diverse (63% black, 26% white, 11% other). Parents were mostly mothers (95%, BMI=35.7±10.4 kg/m2).
Program Components
Exercise
The majority of participants rated exercise as an important and enjoyable component of the MPOWER Junior program. Parents enjoyed the variety of activities offered, and the children particularly liked the game-based activities, such as relays, basketball, and tag. Parents and children enjoyed kickboxing. Several parents noted that it was helpful to have a personal trainer assist the adults so that they could ask questions and prevent injury. Approximately one-third of parents spontaneously noted that they would like more opportunities to exercise with their children at sessions. A couple of the children who turned 12 during the program expressed that they preferred to exercise with the adults rather than the younger children. Typical quotes included:
Child quote: I had lots of fun playing different games every week. I really enjoyed the running relay races. Parent quote: We liked kickboxing. We are normally shy to try something, but we felt good about it. Child quote: I liked working out with kids like me. Parent quote: They showed you can do more than just treadmill—like kickboxing and yoga. It doesn't have to be boring.
Nutrition
Similar to exercise, the majority of participants rated nutrition as an important component of the MPOWER Junior program. The majority of parents reported nutrition education as the most helpful component of the nutrition group, and many reported receiving food samples. Of the few parents and children who remembered having a grocery store tour and/or farmer's market tour, these were positive learning experiences. Suggestions for improvement included incorporating additional hands-on activities/visuals, and several parents of older children noted that they would like the children to attend the nutrition session with the parents. Typical quotes included:
Parent quote: I liked the cooking demonstrations. My child liked things I didn't think she would even try. Child quote: It was pretty cool seeing healthy stuff like a giant cabbage [at the farmer's market]. I ate Asian eggplant and bought fruits and vegetables. Parent quote: We learned how to read labels and menus. We didn't get to learn how to pack lunches until later. It would have been better earlier in the program. Child quote: I liked helping with the cooking demonstrations. It was more fun to do it myself than just watch.
Behavioral
On a scale of 1 (not at all helpful) to 5 (very helpful), the majority of parents rated the behavioral component of the program as either a 4 or 5. Parents who rated the behavioral component “very helpful” noted that they particularly enjoyed learning how to assist children with eating in the absence of hunger, how to deal with resistance to change, and how to introduce new foods. Parents who found the groups helpful recommended additional time for the behavioral group and/or additional sessions. Typical quotes included:
Parent quote: Parent discussions were good for guidance to children's behaviors and dealing with resistance to changes. Parent quote: I liked being able to discuss with other parents. I felt comfortable. Offered suggestions and different things to motivate my child. Children were universally positive about the child group sessions. Typical child quotes included: Child quote: It was good. She taught you how to ignore people picking on you. Child quote: They were fun. I liked how we could speak freely.
Individual sessions
Parents appeared to universally find the individual sessions helpful, but noted that they would benefit from additional time. Many of the parents noted that it was important to have their child present; however, some discussed that when their child was part of these sessions, their child's level of participation was dependent on mood for the day. A couple of parents appreciated time to speak with providers without the children present. Some parents also acknowledged that they enjoyed learning about how their child felt about making healthy choices and challenges. Typical parent quotes included:
Parent quote: Good to give us a chance to sit and talk quietly with a MPOWER team member. Parent quote: My child was present and needed to be. She was more open to try if another adult also said it. I would have liked longer sessions. Parent quote: It was good. They helped you set goals. It was individualized.
Self-monitoring activities
Many parents and children acknowledged that keeping daily logs of weight management–related behaviors (e.g., dietary intake, activity, screen time, sleep) was helpful, but they also described challenges with doing it on a regular basis. Children were generally positive about monitoring activities. Many of the parents liked monitoring dietary intake the most, whereas children appeared to be most enthusiastic about monitoring physical activity. Typical quotes included:
Child quote: I thought it was fun because I could see what I did last week. Parent quote: Good to do. Sometimes we only did 3–4 logs. It helped my child to know that what she ate would be written down. Child quote: Me and the logging didn't really get along so well. I'd rather tell someone than write it down, but I got used to it. Parent quote: Excellent idea. Realistically, difficult to do.
Weekly weight checks
All but 2 parents endorsed weekly weight checks as appropriate. Only 1 parent offered an alternative to weekly weight checks (i.e., taking measurements such as waist circumference). Of the children, all but 1 indicated that weekly weight checks were “okay or fine.” Four children noted that the weight checks made them nervous. Typical child quotes:
Child quote: I liked it. It made me want to watch what I ate. Child quote: It's very hard to see my weight because I don't like the weight that I have now. Child quote: I liked it. I felt proud to lose weight. Got mad when I didn't lose, but thought about how to change behavior. It serves as a reminder. Child quote: I was nervous at first and then I was okay.
Acceptability of program time, frequency, duration, and location
The majority of parents were pleased with meeting once per week. When asked if parents would prefer to meet two times per week for a shorter period of time, there were mixed responses. Several parents would prefer if the second visit included only exercise. Others indicated that it would be challenging to attend twice per week due to distance, other children in the family, or afterschool activities. The majority of families enjoyed the YMCA facility, although some acknowledged that parking was difficult and daycare for younger siblings was limited to 2 hours. Few of the families surveyed reported using the YMCA regularly on nonprogram days or after the program. The most common barrier cited was distance to the YMCA. Typical parent quotes included:
Parent quote: It worked out well for 6 months. We were just getting in the groove and then the 6 months were up. My child wasn't as motivated after that. Parent quote: My kids did a lot after school, so sometimes we had to miss. Sometimes the daycare was full. Parent quote: We liked coming once per week. We would come two times per week if just exercise and no talking.
Completers versus Noncompleters
Next, differences between participants who completed the program versus participants who did not were explored. For this comparison all 35 parent–child dyads (preliminary group and pilot group) were included to increase the sample size of noncompleters. Dyads who attended more than half of the program sessions and attended the 6-month assessment were defined as “completers'” (15/35). Participants who did not meet these criteria were defined as “noncompleters” (20/35). Out of 15 completer dyads, 12 parents and 11 children were interviewed. Three dyads were unable to be reached via telephone. The completers (child mean age=8.6±1.7 years) interviewed were mainly female (94%), recipients of Medicaid (75%), and were racially diverse (44% black, 38% white, 18% other). Out of 20 noncompleter dyads, 7 parents and 4 children were interviewed. Thirteen noncompleter dyads were unable to be contacted via telephone. The noncompleters (child mean age=9.5±1.2 years) interviewed had a significantly different distribution of gender (56% females; χ2=6.3, p=0.01) compared to completers. No other significant differences in demographics emerged for completers versus noncompleters.
Program components
On a scale of 1 (not at all helpful) to 5 (very helpful), parents of completers rated exercise (4.3 versus 3.6), nutrition (4.7 versus 4.4), and behavioral (4.0 versus 3.1) components as more helpful compared to noncompleters.
Acceptability of program time, frequency, duration, and location
More than half of parents of noncompleters rated the time of the program as not acceptable, whereas the majority of the completers expressed satisfaction with the program time. Parents who expressed the program time was not acceptable noted that they had to take their child out of school (if they lived a distance from the program) or they ate dinner late due to travel time. Several parents suggested moving the program time to 5:00 pm, 5:30 pm, or weekends.
Program expectations
The majority of parents who completed the program rated MPOWER Junior as either “exceeding expectations” or “met most expectations.” None of the completers stated that the program “met none of their expectations.” In contrast, over half of parents who did not complete the program expressed that the MPOWER Junior program either “did not meet their expectations” or “met some of their expectations.” Among noncompleters, the most commonly cited reasons for discontinuing participation were scheduling conflicts, distance to the program, and limited gas money. One parent expressed that more medical testing should have been done to determine a biological cause for her child's obesity, and 1 parent stated that the program did not fit her needs as a single mother. However, half of the noncompleters stated they would join the program again, and an additional 2 stated they would if the program could be offered at no cost to them and be more individualized. Notably, all children endorsed that they would like to come back to the program.
Motivation and parent confidence
On a scale of 1 (not at all motivated) to 5 (very motivated), parents of completers rated their child's motivation higher during the program (3.8) compared to after the program (2.9). In contrast, parents of noncompleters rated higher child motivation after the program (3.8) compared to during the program (3.1). Parents of completers rated their own motivation to help their child achieve a healthy weight during the program and after the program the same (4.6). Parents of noncompleters rated their current motivation to help their child (4.2) as higher than their motivation during the program (3.3). Parents of completers and noncompleters rated similar levels of parental confidence to help their child continue to make healthy choices (4.5 versus 4.4).
Discussion
Overall, parents and children were very positive about the MPOWER Junior program. Families viewed the major components of the program as helpful (i.e., exercise, nutrition, behavior). Parents and children particularly enjoyed exercise and cooking demonstrations. Many noted that additional opportunities for exercise and hands-on nutrition related activities would improve the program. While enjoyable, it is unclear if engaging in these activities during the session led to significant changes in physical activity and eating behavior outside of the session, because only perceptions from families were gathered and behavioral outcomes were not measured. However, these activities clearly engaged families. Less enjoyable were the self-monitoring activities and learning about behavior change strategies, despite much evidence that self-monitoring and other behavior change strategies are associated with successful weight management outcomes.24–27 Self-monitoring is time intensive and requires effort from both parents and children. Many of the families noted that it was helpful and acknowledged the importance, but had difficulty doing it on a regular basis. Children were almost universally positive about self-monitoring. However, this may be related to discussions with parents about assuming primary responsibility for completing self-monitoring logs. Ways to increase acceptability of self-monitoring should be further explored.
Families appeared to appreciate individual sessions. Many parents felt that having their child present for the session was necessary. It is interesting to note that the program was developed based on emerging research, suggesting that intervening with parents alone as the agent of change provides meaningful improvements in child weight status.19–22,28 As such, parents were empowered to take responsibility for making healthy changes in their home environment. This message was communicated to families prior to joining the program, as well as during the program in both group and individual sessions. Despite discussions with parents about the evidence-based philosophy regarding how to improve child weight status, these interviews suggest that parents may experience some resistance to providers intervening with parents alone, particularly during individual sessions. It is possible that the desire to have children present during the individual session diffuses some of the parental responsibility for making changes. Further work is required to explore parents' perceptions of parent focused weight management interventions for pediatric obesity.
Families noted that individualized treatment is desirable, and many reported that the individual sessions needed to be longer than 20 minutes. If additional time is allotted for provision of individual sessions with providers, programs will need to determine how to best deliver these services in the context of group treatment programs. Compared to other group programs, this program is novel in offering 20-minute individual sessions twice per month. Many of the families felt that weekly, 2-hour sessions for 6 months were acceptable. The addition of longer individual sessions in the context of group treatment should be examined in future studies.
Weight management programs typically weigh children to assess for progress. However, there is often concern regarding the effect of frequent weight checks, particularly for young children. In this program, parents felt that weekly child weigh-ins were appropriate, although families were only weighed every other week due to the focus on healthy behavior change. Notably, parents and children were weighed at the same time, as a means of diverting some of the focus on the child's weight. In addition, efforts were made to contextualize changes in weight as a tool to use along with nutrition and activity logs to help guide treatment, rather than just as a measure of success. Some of the older children described thinking about change in weight as helpful when determining what they needed to work on for the upcoming week. A minority of children expressed feeling nervous about the weigh-ins. For these children, focusing on the number on the scale may be counterproductive. Early identification of these children may be helpful so that an alternative schedule of weigh-ins may be created.
To better understand factors associated with attrition in the program, responses of program completers versus noncompleters were compared. Although not all noncompleters participated in the interviews, those who did participate appeared to be more likely to experience unmet expectations for the weight management program compared to completers. Reasons for discontinuing participation in this program were similar to reasons cited in other programs. These include transportation barriers (e.g., gas money, distance), scheduling conflicts, and unmet expectations.9,29,30 However, the majority of parents and all of the children indicated that they would like to come back to the program. This is consistent with findings from other programs.30,31 Among the noncompleters, the children's responses were universally more positive than the responses of their parents.
Although the sample was very small, it is interesting to note that differences emerged with respect to parent report of child motivation during the program and after the program for completers versus noncompleters. Parents of noncompleters rated higher child motivation after the program compared to during the program, whereas parents of completers reported higher child motivation during the program compared to after the program. Parents of completers rated similar levels of motivation at both time points. Decreased child motivation after participation in a weight management program may be responsible in part for weight gain that is often noted posttreatment in many programs. In fact, based on anecdotes from adults who found it difficult to motivate themselves to continue to engage in weight management related behaviors posttreatment, a randomized controlled trial of a motivation-focused maintenance weight loss program for adults was implemented. 32 It was found that targeting motivation was an effective alternative to more traditional skills-based weight maintenance treatment. The finding of parents' perception of lower child motivation after completion of the intensive weight management program highlights the need to better understand how to prepare children and families for posttreatment and/or how best to provide ongoing contact with families to assist with maintaining motivation for healthy lifestyle habits. Given that noncompleters experienced an increase in motivation following discontinuation, the mechanism for this may deserve some more attention. It is possible that noncompleters are still looking for strategies to assist with weight management because the program did not meet their needs, and thus report higher motivation.
Limitations of this study should be acknowledged. First, this study examined perspectives and impressions from participants in one pediatric weight management program. The sample size was relatively small and the age range of the children was restricted to 7–11 years. It is possible that the program had an impact on other children in the family, but this was not directly assessed. Impressions from this program may not be generalizable to other programs and clear associations between perceptions and outcomes cannot be made. Furthermore, not all participants who were contacted via phone chose to participate. However, the participants interviewed included completers and noncompleters, representing a spectrum of perspectives. A larger sample size in the future will be necessary to draw more definitive conclusions regarding rate of completion, the association with perceptions and outcomes, and continued motivation after study completion.
Conclusions
This study may have implications for how to enhance family-based pediatric weight management programs for children ages 7–11 years. Children particularly enjoyed opportunities to engage in fun, game-based activities. Families also enjoyed cooking demonstrations and being exposed to new, healthy foods. Parents noted that adding additional group exercise classes (and possibly including parents), increasing the number of cooking demonstrations/hands-on nutrition activities, and increasing the length of individual sessions would be beneficial. Future research should examine how the addition of these components, either alone or in combination, may enhance engagement, retention, and anthropometric outcomes. The study also found that many parents would prefer to include their children in individual sessions. Given emerging research in the efficacy and cost-effectiveness of intervening with parents alone in pediatric weight management treatment, further exploration of parents' perceptions of this treatment modality may be helpful to assist with determining how to increase acceptability of parent-based treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.