
Abstract
Abstract:
Background:
Few interventions targeting severely obese minority youth have been implemented in community-based settings. We evaluate a 9-month multicomponent, community-based program for obese, inner-city adolescents.
Methods:
Of 5250 estimated eligible adolescents, 349 were recruited; they had a mean age of 15±2 years, mean BMI %ile 98.9±1.5, and comprised 52% African American and 44% Hispanic. Longitudinal trends of anthropometric measures were compared 1 year before enrollment (T−12), at baseline (T0) and after program completion (T9). Dietary and physical activity behaviors were compared at T0 and T9. Anthropometric changes were compared at T9 and 18 months (T18) in completers and noncompleters.
Results:
A majority of participants were severely obese (67%) and expressed low readiness to change behaviors (82%). For intervals T−12 to T0 versus T0 to T9, there were significant decreases in rates of gain in BMI (0.13 vs. 0.04, p<0.01), BMI percentile (0.0002 vs. −0.0001, p<0.01), percent overweight (0.001 vs. −0.001, p<0.01), and BMI z-score (0.003 vs. −0.003, p<0.01). Significant increases in vegetable and fruit consumption and in vigorous physical activity participation were observed. From T9 to T18, except for a significant increase in BMI (38.3±7.4 vs. 39.0±7.5, p<0.01) in completers, all other anthropometric measures remained unchanged in completers and noncompleters.
Conclusions:
We demonstrate modest clinical improvements and increased healthy lifestyle behaviors in predominantly severely obese, difficult-to-reach, ethnic minority adolescents attending a community-based weight management program. The loss of clinical improvements 9 months after program completion implies that extending the duration of such a program may prevent long-term weight regain in severely obese adolescents.
Introduction
Although most published weight management interventions have been conducted in well-controlled clinic or school-based research settings, few have been conducted in busy, understaffed health clinics, large health systems, or community settings serving low-income, severely obese, minority adolescents. 4 Furthermore, there is a lack of evidence indicating that interventions that prove efficacious in randomized trials are effective in the general population or that such interventions can be sustained on a long-term basis. Developed in 2005 as a collaborative effort between the Children's Hospital at Montefiore (CHAM) and the Mosholu Montefiore Community Center (MMCC), The Bronx Nutrition and Fitness Initiative for Teens (B'N Fit) program is a community-based weight loss program for low-income obese minority adolescents, ages 12 through 21 years. The program incorporates evidence-based elements of successful weight loss interventions, including a multicomponent program with nutrition, sedentary behavior reduction education, and parental involvement.5,6 We report on the characteristics of participants who access the program as well as the impact of the program on participant anthropometrics and self-reported diet and physical activity behaviors.
Methods
Design
This is a quasi-experimental single arm pre–post test 9-month study. In a previous randomized controlled trial examining the efficacy of the B'N Fit program, patients presenting to the B'N Fit program for weight management were recruited. In the control arm, subjects received monthly doctor visits and healthy lifestyle printed material for 3 months compared to the study arm, where subjects received all components of the B'N Fit program, including monthly doctor visits, nutrition groups, and physical activity sessions. There was poor acceptability of the randomized controlled trial from patients and parents initiating the program. Of patients who agreed to participate in the study, we had much higher attrition rates in the control arm at initiation (33%) and at 6-month follow-up (62%) compared to the study arm (9% and 41%, respectively). The insufficient follow-up data made it difficult to compare changes in anthropometric measures between the two arms, and the findings of this pilot study were reported as the association of BMI to changes in cardiovascular disease risk markers for all subjects. 7 Our experience of low participant acceptability and high attrition rates in the control arm resulted in the present pre–post 9-month study design where all youth presenting to the B'N Fit program in search of comprehensive weight management services would be offered such services. In effect, we evaluated the B'N Fit program, which incorporates efficacious elements of successful randomized trials in a community setting utilizing a pre–post design that we anticipated would be more acceptable to the youth that the program intends to serve.
Subjects
Approximately 250,000 people reside in the Fordham and Bronx Park Neighborhoods surrounding two Bronx institutions, the CHAM and the MMCC. 8 According to the US Census Bureau American Community Survey Housing Estimates (2005–2009), adolescents comprise 16% of the Bronx County population. 9 Extrapolating from this proportion, an estimated 40,080 adolescents live in the Fordham and Bronx Park neighborhoods. On the basis of the 2009 New York City Youth Risk Behavior Surveillance (YRBS) data, with a 13.1% rate of obesity among Bronx teens, an estimated 5250 obese adolescents reside in these neighborhoods. 10 Adolescents are referred to the program by general pediatric and subspecialty practices, MMCC youth programs, word-of-mouth, school-based health clinics, and by the CHAM Pediatric Emergency Department and Inpatient Adolescent units.
Participants who joined the program between April 1, 2007, and April 30, 2009, were recruited consecutively. Participants with co-morbid illnesses, such as type 2 diabetes, were included, as many of these conditions are secondary to obesity. Adolescents with secondary obesity (1%) or a diagnosed major mental illness or intellectual disability, who were unable to consent or unable to comply with the protocol (2%), were excluded.
Additional recruitment was conducted at MMCC's six afterschool programs. Parents were notified by letter of a BMI screening and for adolescents whose parents did not explicitly decline BMI screening, height and weight were measured, BMI was calculated, and referrals to B'N Fit were made if obesity criteria were met.
At the initial B'N Fit clinic visit at CHAM, adolescents were offered study enrollment. The study was approved by both the Montefiore Medical Center and Albert Einstein College of Medicine Institutional Review Boards. Both participants and parents signed informed consent and HIPAA authorization.
The B'N Fit Intervention
Overview of program structure
The Program was designed as a 9-month program that consists of a 12-week Induction phase followed by a 6-month Maintenance phase. (Fig. 1).

Hospital-based activities at CHAM
At enrollment, the physicians complete a comprehensive medical history and physical examination at the B'N Fit clinic. The social worker (SW) conducts a psychosocial evaluation and assesses participant readiness to adopt healthy lifestyle behaviors. The dietician (RD) conducts an assessment of dietary and physical activity behaviors and determines nutrition and healthy lifestyle goals. Referrals to medical, psychiatric, or surgical subspecialties for the treatment of co-morbid conditions are made if indicated. In accordance with the Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report, physicians determine weight loss goals based on participant age, sex, and on patient/family readiness to change. 11 For all participants 12 years of age and older with a BMI >95th percentile, the Expert Committee recommends weight loss until BMI reaches <85th percentile with no more than an average of two pounds of weight loss per week. The dietary and physical activity habits and eating behaviors that are encouraged in patients and families of the patient are as listed in the Key Program Features section, below. 11 Physicians review weight loss, healthy lifestyle, and nutrition goals and monitor co-morbidities and medical, social or psychiatric barriers to participation monthly for the first 3 months and then every 3 months. Participants with depression, anxiety, binge eating, personality disorders, or other significant psychosocial stressors are identified by the physician and/or SW and referred for mental health services.
Community-based activities at MMCC
Following the initial evaluation, participants attend program activities in an adolescent-focused afterschool setting at MMCC to coincide with the NYC Public School system schedule for school hours and vacation. Program teaching occurs primarily during weekly Induction 60-minute group sessions. The sessions co-led by the RD, SW, and youth leader emphasize an adolescent-focused approach to teach healthy lifestyle principles. (Table 1). Concepts taught during the Induction curriculum are reviewed during Maintenance group sessions and applied to adolescent-relevant topics taught in monthly themes (Table 1). Induction and Maintenance participants have joint access to up to four 60-minute physical activity sessions per week. These sessions consist of moderate physical activity aimed at promoting fitness, strength, flexibility, increased caloric expenditure, team-building skills, and relationship-building opportunities. A monthly family night for all participants and their families mirrors topics discussed in participant group sessions with an emphasis on how the entire family can adopt healthy behaviors. Individual or family SW and RD sessions are implemented to follow-up behavior, nutrition and lifestyle change goals and barriers to achieving these goals.
Program Curriculum
Maintenance curriculum topics follow monthly themes for each of the 12 months of the year. Participants receive 6 of the 12 monthly topics depending on when they begin their 6-month maintenance portion of the program.
Key Program Features
The nutrition and behavioral goals of the program follow the Expert Committee Recommendations. 11 Girls are counseled not to exceed 1800 calories/day, and boys are counseled not to exceed 2200 calories/day in accordance with the USDA guidelines for caloric intake. 12 Individualized recommendations are provided based on participants' typical diets and activity level and follow these general guidelines: Limit consumption of sugar-sweetened beverages; encourage consumption of recommended quantities of fruits and vegetables; limit television and other screen time to no more than 2 hours per day and removing television and other screens from participant's sleeping area; eat breakfast daily; limit eating out, especially at fast food restaurants; encourage family meals; limit portions to appropriate serving sizes; eat a diet high in fiber; promote moderate to vigorous physical activity for at least 60 minutes per day; and limit consumption of energy dense foods. 11 Patient and/or family readiness to change was determined based on family support, psychosocial and environment stressors, and household structure and was taken into consideration when implementing recommendations.
The program incorporates the Transtheoretical/Stages of Change model to assess participant readiness to change behaviors and motivational interviewing (MI) techniques to support behavior change.13,14 The Transtheoretical/Stages of Change model has been used in adults and adolescents to assess their readiness to adopt healthy lifestyle behaviors, including increasing physical activity and consuming less fat, higher levels of fiber, and more fruits and vegetables.15–18 MI is a focused, guided counseling style that achieves behavior change by helping individuals increase their intrinsic motivation for behavior change using reflective listening and empathy to help clients resolve ambivalence about behavior change. Motivational enhancement (ME), an abbreviated form of MI, has been applied to dietary behavior change.19,20 The ME approach is not only nonconfrontational, but is also respectful of the adolescent's autonomy; an ME approach is incorporated into all clinical and program activities.
Program Staff and Training
The hospital-based RD, SW, program coordinator, and physicians contributed program content and the community center–based youth leaders and administrators created a youth-focused environment and operationalized the program structure. The youth leaders were trained to facilitate and engage large groups of teens through annual youth development training workshops and ongoing on-site training by MMCC senior administration. All staff received training by a member of the Motivational Interviewing Network of Trainers (MINT) 19 in ME Interviewing approaches during a 1-day workshop. The Trainer used role playing to introduce skills, such as use of open-ended questions, and affirmations, reflections, and summary to work with staff to engage youth and their families in decision-making.
Program Effectiveness Evaluation
Methods
At baseline, a research nurse at the Clinical Research Center (CRC) at CHAM obtained weight using the Scale Tronix digital scale (Scale-Tronix 5002, White Plains, NY) and height using a stadiometer (measured to 0.1-cm accuracy). BMI was calculated using the formula weight (kg)/height (m) 2 . BMI z-score and BMI percentile were obtained using the CDC Epi Info program. 21 Percent overweight was calculated as percent over the median BMI for age and gender. 22 The medical and family histories were reviewed for obesity related co-morbidities. Family structure was defined as single- or two-parent household, or other, including foster care. The social worker used the Transtheoretical model to assess participants' readiness to change lifestyle behaviors. 19 The following stages of change were assigned: ‘Pre-contemplation’ if there was no intention to change; ‘Contemplation’ if there was a long-term intention to change; ‘Preparation’ if there was a short-term intention to change; and ‘Action’ if there was evidence of behavior change. 23 To obtain dietary behaviors, participants completed a dietary questionnaire incorporating items from the youth NHANES food frequency questionnaire, the YRBS, and the WAVE (Weight, Activity, Variety, and Excess).24–26 The WAVE tool was designed to facilitate nutrition assessment and counseling during brief clinical encounters. Moderate and vigorous physical activity in the prior 2 weeks was assessed using the Modifiable Activity Questionnaire for Adolescents. 27 Baseline characteristics of participants who completed the 9-month evaluation were compared to those who did not return for the 9-month evaluation to assess for differences between these two groups.
Effectiveness
Program effectiveness was evaluated by comparing the longitudinal trends of anthropometric measures, including BMI, BMI z-score, percent overweight, and BMI percentile over three time points: 1 year before joining the program (T−12), at baseline (T0), and after completing the 9-month program (T9). In addition, dietary behaviors, physical activity, and sedentary behavior assessments were compared at T0 and T9 and effectiveness of the groups and physical activity on the anthropometric measures was determined. Additional anthropometric measures were obtained 9 months postprogram completion (T18) to assess whether program effects were sustained. Pre-enrollment (T−12) anthropometric measures were obtained from 8 to 16 months prior to starting the program, either through the CHAM electronic medical record system (EMR) or the primary care provider. For the T0 and T9 measures, we used anthropometrics, dietary behaviors, physical activity, and sedentary behavior assessments collected at the CRC. We defined completers as subjects who returned to the CRC for T9 measurements and noncompleters as subjects who did not return to the CRC for T9 measurements and whose T9 measurements were obtained from the CHAM EMR. Postprogram completion (T18) anthropometric measures for completers and noncompleters were obtained from the CHAM EMR 18 months following the baseline visit.
Statistical Methods
Descriptive statistics were used to define participants' baseline demographics and behavioral characteristics. We used t-tests and chi-squared tests to compare differences in baseline demographics, anthropometric measures, and lifestyle behaviors between participants who completed the 9-month program evaluation and those who did not.
To compare the longitudinal trends of anthropometric measures pre- and postenrollment in the program, we tested differences in slopes of these measures from T−12 to T0 (β1) and from T0 to T9 (β2) by applying mixed-effects linear models that take within-subject correlations of repeatedly measured outcomes. To test the slope difference for BMI, BMI percentile, percent overweight, and BMI z-score, we fit two models, one with a single slope (β3) and another with two slopes (β1 and β2) connecting at baseline, and tested the significance of differences in twice log-likelihoods, referred to as −2LL, using a chi-squared test with one degree of freedom.
To examine the effectiveness of the groups and physical activity on the anthropometric measures, we used intent-to-treat analyses using data collected from T0 and T9 CRC visits as well as from all interim physician visits to the program. In this mixed-effects modeling, the longitudinal trends were modeled as a function of the number of nutrition groups and physical activity sessions attended adjusting for trends over time. The mixed-effects modeling approach is known to be valid even in the presence of missing values that occurred at random depending on the observed values. Behavioral changes were compared at T0 and T9 program evaluations using the McNemar test for categorical data.
To examine whether the outcomes were sustained following program completion, we used mixed-effects linear modeling to compare changes in anthropometric measures from T9 to T18 between completers and noncompleters.
Analyses were performed using SAS v. 7.0 (SAS® Institute Inc., Cary, NC). For all analyses, a p value of <0.05 was considered statistically significant.
Results
Figure 2 depicts the study reach, recruitment, and program completion results. Of the estimated 5250 obese adolescents living in the Fordham and Bronx Park neighborhoods, 676 (13%) scheduled an initial visit to the program. Due to low recruitment at the afterschool sites (15% of eligible youth that were screened made an appointment), recruitment was abandoned at these sites after 6 months.
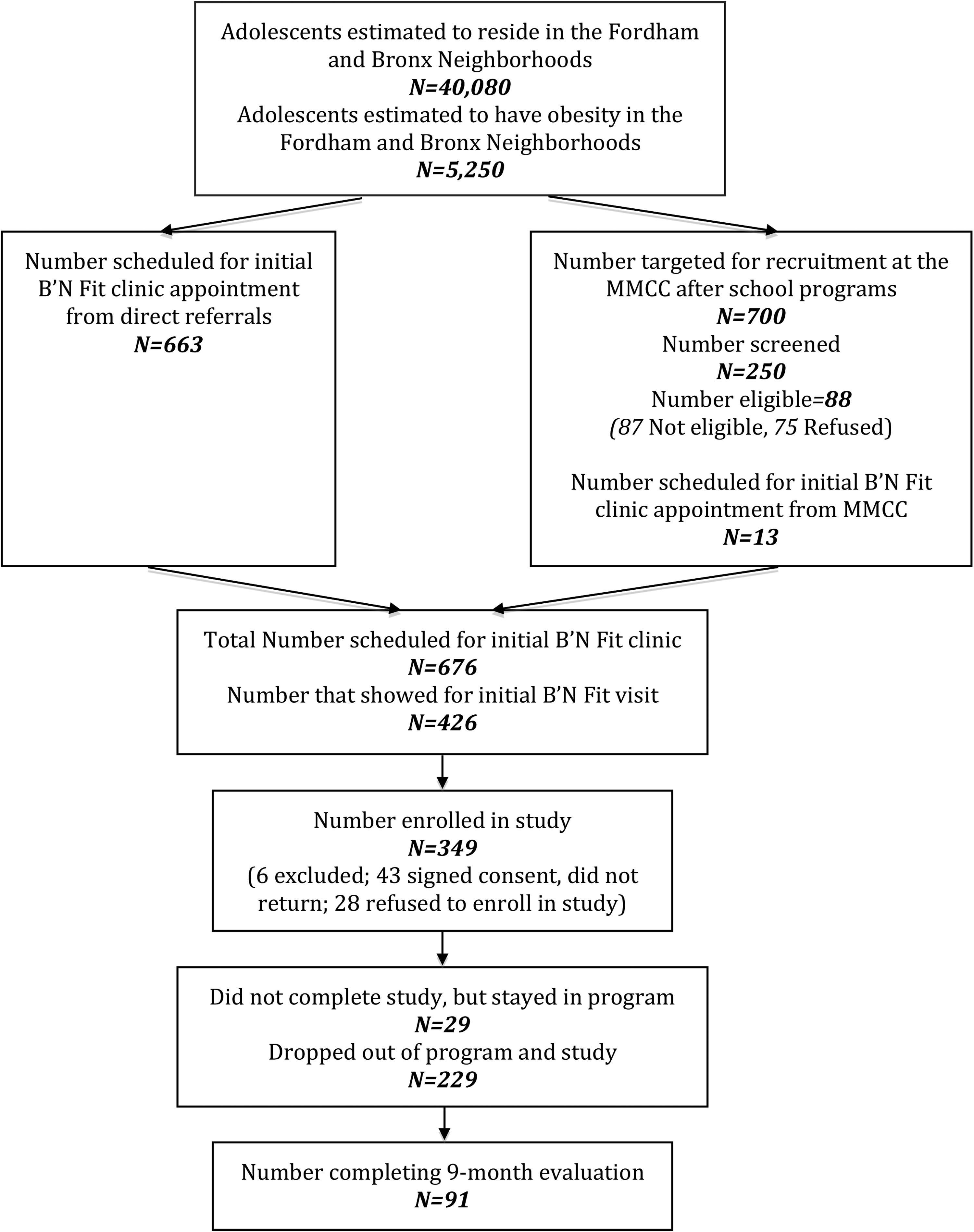
From April, 2007, to April, 2009, there were 349 adolescents that completed baseline assessments. The mean age was 15±2 years, 54% were female, the mean BMI was 39.2±7.3; and 52% were African American, whereas 44% were of Hispanic ethnicity (Table 2). At baseline, a majority of participants (68%) were in the precontemplation or contemplation stage of behavioral readiness, 67% fulfilled the criteria for severe obesity, and there were multiple obesity-related co-morbid illnesses. In all, 79% of participants consumed one or more sugary drinks per day, many consumed no fruits (50%) or vegetable (57%) servings per day, and less than 5% consumed four or more servings of fruits or vegetables per day. Only 17% of participants spent 6 or more hours participating in vigorous physical activity in the preceding 2-week period, yet almost 90% spent 2 or more hours per day watching television or playing computer or video games and 31% spent 6 or more hours doing so.
Baseline Characteristics of Study Cohort N=349
SD, standard deviation.
Ninety-one participants (26%) completed the 9-month program. There were no significant differences in age, sex, ethnicity, baseline anthropometrics, the presence of co-morbidities, parental history of obesity, family structure, readiness to change behaviors, and baseline nutrition, physical activity, and sedentary behavior assessments between those that completed the 9-month evaluation and those that dropped out.
Program Effectiveness
Comparing the changes in anthropometric measures from 1 year prior to joining the program (T−12) to the changes following program participation (T9), we found significant, but modest clinical improvements in the rate of change in all anthropometric measures (Fig. 3). For example, prior to enrollment, BMI increased by 0.13 kg/m2 per month and after enrollment, the rate of increase in BMI decreased to 0.04 kg/m2 per month (Fig. 3a).

For each nutrition group attended, there were significant decreases in BMI (−0.07 kg/m2 per month; p<0.001), percent overweight (−0.002%/month; p<0.001) and BMI z-score (−0.003/month; p<0.01) and a near significant decrease in BMI percentile (−0.006 %ile/month; p=0.06). There were also significant decreases in BMI (−0.03 kg/m2 per month; p<0.0001), percent overweight (−0.0008 %/month; p<0.0001), BMI z-score (−0.001/month; p<0.001) and BMI percentile (−0.005/month; p<0.01) for each physical activity session attended. Sensitivity analyses examining changes in anthropometric measures, based on application of the same mixed-effects modeling approaches with only actual attendance data, showed similar improvements (data not shown).
We found a significant increase in the number of vegetable and fruit servings consumed per day and significant improvements in vigorous physical activity behaviors (Table 3).
Changes in Lifestyle Behaviors in Participants Who Completed the 9-Month Program (N=91)
Based on exact McNemar's tests.
Bold signifies p<0.05.
Program Attendance and Retention
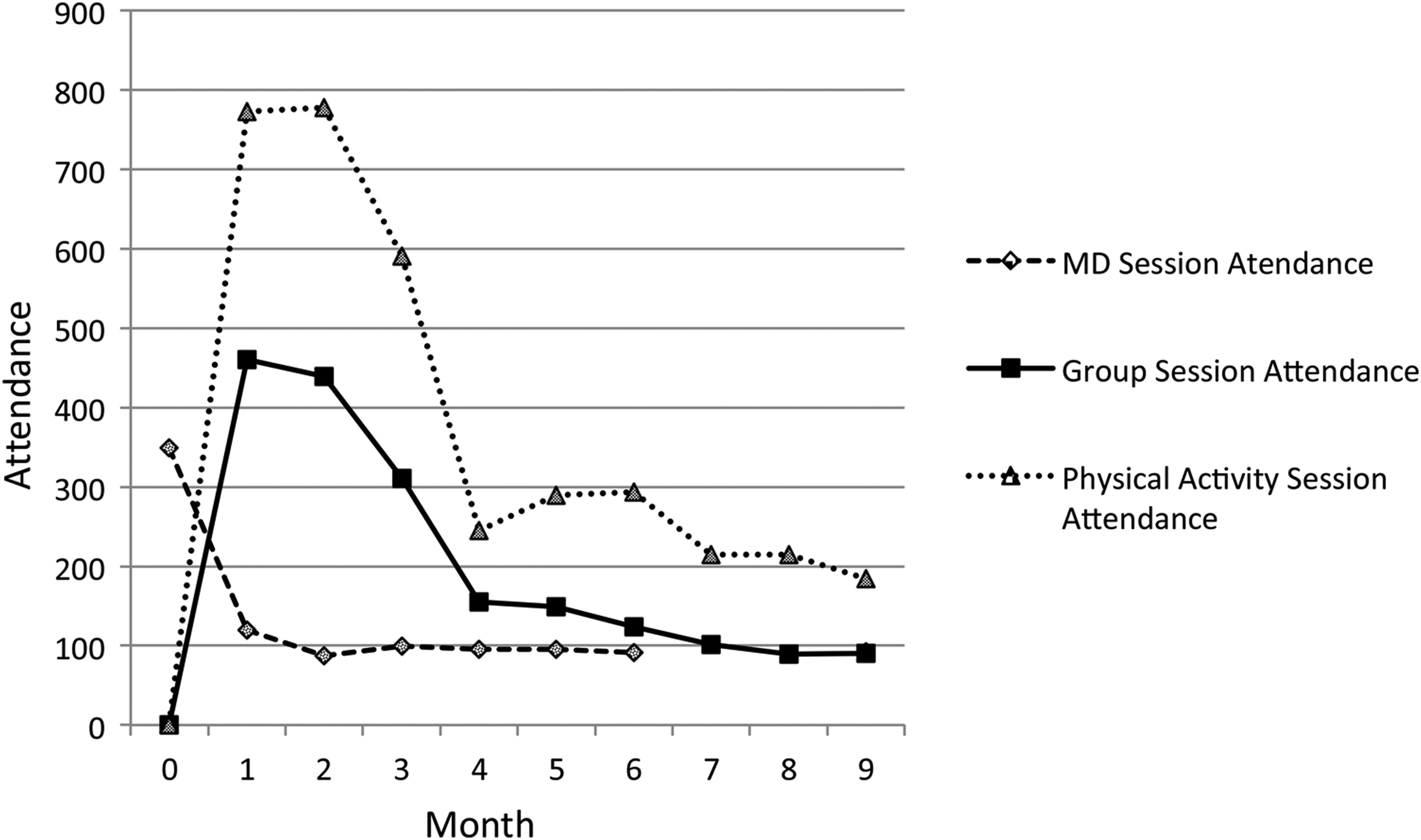
Program participation and retention were low. Although tracked inconsistently by staff, the most frequently documented barriers to participation included school obligations, family emergencies, and transportation issues. A dramatic drop in monthly attendance was noted after the baseline physician visit and after 3 months for group and physical activity session attendance. (Fig. 4).
Postprogram Follow-Up
Among completers, while not significant, there was a decrease in BMI z-score (2.37±0.36 vs. 2.32±0.38, p=0.6) and a significant increase in BMI (38.3±7.4 vs. 39.0±7.5, p=0.002) from T9 to T18. Among noncompleters, while not significant, there was an increase in BMI (40.4±8.8 vs. 40.9±7.8, p=0.2). All other anthropometric measures remained unchanged from T9 to T18 in the two groups.
Discussion
The B'N Fit program was developed in response to the urgent need to develop effective, culturally appropriate, and feasible community-based weight loss interventions for severely obese, minority adolescents. The program was developed using evidence-based elements of successful weight loss interventions and has been implemented by hospital and community center staff in a community setting. We demonstrate that a majority of the ethnic minority adolescents we reached were predominantly severely obese, consumed sugary drinks on a daily basis, had low daily fruit and vegetable consumption, reported more than 2 hours of television, computer, or internet usage per day, and were largely not ready to change their behaviors. Despite educational, family, and transportation barriers to participation, we demonstrated modest but significant improvements in their anthropometric measures as well as dietary and physical activity behaviors following participation in the 9-month program. Program completers demonstrated an increase in BMI 9 months following program completion. These findings suggest that without the continued healthy lifestyle support offered by the program, weight gain is likely and a longer-term intervention may be indicated for this population.
Lessons Learned
Despite high rates of obesity in the Bronx, a small proportion of estimated eligible adolescents (13%) enrolled in the B'N Fit program and a low proportion of enrollees (26%) completed the 9-month program. Furthermore, reaching out to adolescents directly in the school setting yielded much lower results than provider referrals. Afterschool program site directors attributed low recruitment to adolescents' reluctance to undergo BMI screening, even when privacy was ensured. Furthermore, although adolescents expressed interest in joining the program, parents were often not interested when calls were made to schedule appointments. Although we did not expressly determine the representativeness of our study sample, the participants were predominantly African American and Hispanic, which is similar to the demographics of the community that we serve. Adolescents that were not reached may have shared similar characteristics to our program participants and, in addition, may have experienced even more barriers to attending the program as well as having a low awareness of the program's existence. Efforts to improve the program reach may include initiatives that strengthen partnerships between primary care providers, patients and their families, and weight loss intervention providers. In addition, increased support of the strengths of the community-based aspect of the B'N Fit program may better align programming to the needs of adolescents and their families. This, in turn, may increase engagement of the adolescents and the community that supports them.
Pediatric weight management interventions with three or more components, including physical activity, nutrition, sedentary behavior reduction, and counseling, are most likely to produce weight loss (1.9–3.3 kg/m2 decrease in BMI at 12 months). 5 Furthermore, interventions incorporating parental involvement, lifestyle change, and culturally based adaptations demonstrate up to a 1.7 kg/m2 decrease in BMI in minority youth. 6 Although the literature abundantly details the efficacy of such weight loss interventions,5,6,28,29 particularly in highly motivated, Caucasian, moderately obese populations,30,31 few studies demonstrate community setting effectiveness for severely obese ethnic minority adolescents.4,6 An emphasis on developing clinically significant outcomes often produces intensive and expensive interventions that are conducted in highly controlled specialty treatment center environments, use access to standardized protocols, and are demanding of both patients and highly trained staff. 32 Such interventions are less likely to be effective in more complex, less advantageous settings with less motivated patients and overworked staff.33,34 The B'N Fit program incorporates the evidence-based elements of successful pediatric weight loss interventions into an intensive, yet adolescent-friendly, community-based weight management program that, with minor exceptions, was highly inclusive of all interested participants and was predominantly conducted by community-based staff with an emphasis on adolescent programming.
Pediatric weight loss programs targeting children and adolescents tend to have more success with children and have led some to suggest that, given limited resources, weight management efforts be placed in children rather than adolescents. Of 54 lifestyle interventions included in the most recent Cochrane review and 40 interventions included in a meta-analysis of obesity interventions among American minority youth, 37 studies included adolescents with a mean age at or above 12 years.6,35 Of these 37 studies, a majority included ethnic minority youth, 15 were community-, school-, or family-based, and only four studies had participants with baseline BMIs above 35 kg/m2.36–39 While improvements in outcome measures were demonstrated among ethnic minority adolescents with BMIs in excess of 35 kg/m2, the long-term follow-ups of these interventions were either not reported or demonstrated weight regain.36–39 Although participants were younger than our participants, Savoye et al. conducted the only RCT of all literature reviewed that reported a sustained weight loss in a predominantly diverse obese population with severe obesity (baseline BMI >35 kg/m2). 4
Despite low motivation to change lifestyle behaviors and familial and resource-related barriers to retention, we have demonstrated that with an emphasis on adolescent-focused programming in a convenient community-based setting, the B'N Fit program was effective at decreasing rate of weight gain and changing behaviors in adolescents who were predominantly severely obese (mean baseline BMI=39), and there were significant improvements in anthropometric outcomes with each nutrition and physical activity session attended.
As in other studies, 36 participants who completed the program demonstrated an increase in BMI following the completion of the program. These findings suggest that there may be a need to extend the duration of the lifestyle support offered by this program and others to continue to maintain or decrease BMI and prevent weight regain in severely obese adolescents. With augmentation of efforts to provide long-term community-based programming that adapts to the unique needs of adolescents and their families, B'N Fit is well-positioned to directly impact the healthy lifestyle behaviors of the adolescents that will potentially be parents themselves over the next 5–10 years as well as indirectly impacting the family members that support them.
Paradoxically, despite the breadth of services offered to address the complex needs of the participants, the multicomponent nature of the program may actually place further demands on participants and their families, resulting in lower program adherence. Efforts to engage participants and address barriers to retention would likely have a greater impact on participants if initiated within the first month of program participation. An incentive program and an augmentation of the use of ME may advance participants to a higher stage of readiness to change behaviors, although the effect of ME in this population requires further study. In addition, retention may improve by instituting a program orientation to facilitate an increased understanding of program requirements by potential participants. Finally, face-to-face engagement of staff and participants together on topics exploring the barriers to achieving goals as well as methods of partnering together to develop relevant approaches to achieving healthy lifestyle goals may be important to energize participants and staff alike with the goal of improving the program's impact on the adolescent, their family, and their community.
Limitations
Although our difficult-to-reach population and intensive programming poses a challenge for widespread dissemination and replication of B'N Fit at multiple sites, our evaluation of the program provided critical insights into the complex needs of the participants served by the program and confirmed the importance of intensive programming. Although we did not expressly determine the representativeness of our study sample, we limited our exclusion criteria, producing a heterogeneous sample that more closely approximates the target population. We examined the effectiveness of the groups and physical activity on the anthropometric measures, but we did not do a similar analysis for physician visits, family nights, and individual SW and RD sessions because of overall low attendance at these sessions. Although we assumed that missing observations occurred at random depending on the observed values, it is unknown if this widely accepted assumption for the mixed-effects modeling holds for the present analysis.
Conclusions
In the United States, a large proportion of ethnic minority adolescents with obesity lack the resources to make the necessary behavioral changes to adopt a healthier lifestyle. The B'N Fit program provides an example of a weight loss program that serves obese, difficult-to-reach, ethnic minority adolescents in a community-based setting. We drew from the strengths of a hospital and community center partnership to provide an adolescent-focused program that demonstrates a modest, but significant, decrease in level of obesity and a significant improvement in the adoption of healthy lifestyle behaviors. By evaluating the program, we have taken an initial step in addressing the robustness, translatability, and assessment of the long-term impact of the program on the community it serves.
Footnotes
Acknowledgments
This publication was supported by Philips Electronics of North America, The New York State Health Foundation, and in part by the CTSA Grant UL1RR025750, KL2RR025749 and TL1RR025748 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH roadmap for Medical Research. U.I.K.'s time is partially supported by the National Heart, Lung, and Blood Institute (NHLBI) Mentored Patient-Oriented Research Award (1K23HL105790). We express our appreciation to our collaborators at the Mosholu Montefiore Community Center (Rita Santelia, Don Bluestone, Lisa Nicotra, Lenora Seeley), at the Children's Hospital at Montefiore (Elaine Brennan, Philip Ozuah, Susan Coupey, Rachel Taniey, Dionne Sears, Elicia Johnson-Knox, Michelle Calderoni, Rachel Siegel, Alexandra Salazar, Bena Gershon), and our students and volunteers for their innovation and commitment to the program. Most importantly, we thank our patients and their families for the opportunity of letting us serve them.
Author Disclosure Statement
No competing financial interests exist.