
Abstract
Abstract
Background:
Interventions to promote physical activity (PA) in children attending family child care homes (FCCHs) require valid, yet practical, measurement tools. The aim of this study was to assess the validity of two proxy report instruments designed to measure PA in children attending FCCHs.
Methods:
A sample of 37 FCCH providers completed the Burdette parent proxy report, modified for the family child care setting for 107 children 3.4±1.2 years of age. A second sample of 42 FCCH providers completed the Harro parent and teacher proxy report, modified for the family child care setting, for 131 children 3.8±1.3 years of age. Both proxy reports were assessed for validity using accelerometry as a criterion measure.
Results:
Significant positive correlations were observed between provider-reported PA scores from the modified Burdette proxy report and objectively measured total PA (r=0.30; p<0.01) and moderate-to-vigorous PA (MVPA; r=0.34; p<0.01). Across levels of provider-reported PA, both total PA and MVPA increased significantly in a linear dose-response fashion. The modified Harro proxy report was not associated with objectively measured PA.
Conclusion:
Proxy PA reports completed by family child care providers may be a valid assessment option in studies where more burdensome objective measures are not feasible.
Introduction
With 60% of children in the United States under the age of 5 years attending some type of regular child care, child care settings provide abundant opportunities to introduce and promote healthy lifestyle behaviors. 5 Currently, family child care homes (FCCHs) are the second largest provider of nonrelative care in the United States, offering child care to just over 10% or approximately 1.9 million children under the age of 5. 6 FCCHs are unique from other types of care. Classified as small businesses, they are generally privately owned and operated by the provider, who is typically female. Providers must balance the demands of their personal home and family life concurrently with the demands of providing care and education to what is often a mixed-age group of young children. States vary widely in their licensing standards of FCCHs, including the adult-to-child ratio, group sizes, and educational and experiential requirements.7,8
Although a significant percentage of young US children attend family day care, little is known about physical activity levels in this setting. The available evidence, although limited, suggests that children attending FCCHs are insufficiently active, accumulating less than 10 minutes of moderate-to-vigorous physical activity (MVPA) per hour of child care attendance.9,10 Further, a recent study examining physical activity policies and practices in FCCHs found that most providers failed to meet established child care standards for structured play, screen time, and indoor play space. 11 Moreover, few providers reported receiving training in physical activity (PA) or having a comprehensive written policy on PA, suggesting that intervention programs to promote physical activity in FCCHs are warranted. 11
In order to evaluate interventions to promote physical activity in FCCHs, valid, yet practical, measurement tools are required. Among preschool-aged children, physical activity is typically measured using direct observation or motion sensors, such as accelerometers or pedometers. 12 However, the cost and participant burden associated with these methods make them difficult to implement in large surveillance studies and/or community-level program evaluations. For these scenarios, proxy reports completed by FCCH providers may be a viable option; however, the validity of this approach has not been evaluated. Accordingly, the aim of this study was to evaluate the concurrent validity of two brief caregiver proxy report instruments designed to measure PA in preschool-aged children attending FCCHs.
Methods
Participants and Settings
Participants for the study were recruited from FCCHs enrolled in the Healthy Home Child Care Project, a 3-year group-randomized trial testing the effects of a comprehensive, multi-level intervention to promote healthy eating and regular PA in FCCHs. FCCHs were recruited from five regional child care resource and referral hubs serving seven economically diverse counties in Oregon. Initially, 63 FCCHs were recruited into the study. Of those, five had too few children in their care when data collection began (less than 4 children), and two others withdrew from the study before data collection, leaving a possible sample of 56 FCCHs and their child attendees for the study. Thirty-seven FCCHs completed the accelerometer and proxy report measurement protocols in year 1 of the study, whereas 42 FCCHs completed the accelerometer and proxy report measurement protocols in year 2 of the study. FCCHs did not complete a proxy report in year 3. PA assessments were completed at baseline (year 1, March–May 2010), immediately postintervention (year 2, March–May 2011), and 12-month follow-up (year 3, March–May 2012). The study was approved by the Oregon State University Institutional Review Board (Corvallis, OR), and preceding participation, FCCH providers and the children's parents provided written informed consent.
Proxy Report Instruments
Modified Burdette proxy report
Burdette and colleagues 13 developed and validated a parent report instrument that measured outdoor play time as a surrogate measure of PA in preschool-aged children. The two-item outdoor playtime checklist asked parents to respond to the following questions: (1) “How much time did your child spend playing in the yard or street around your house (or the house of a friend, neighbor, or relative)?” and (2) “How much time did your child spend playing at a park, playground, or outdoor recreation area (for example, swimming pool, zoo, or amusement park), including while at day care or preschool?” For each item, the day was segmented into three time periods: wake-up time until noon; noon until 6 pm; and 6 pm until bedtime. For each of these time periods, outdoor playtime was reported on a 5-point scale with the following responses: 0 minutes; 1–15 minutes; 16–30 minutes; 31–60 minutes; and over 60 minutes. Responses within each time interval were coded as 0 through 4 (0=0 minutes; 1=1–15 minutes; 2=16–30 minutes; 3=31–60 minutes; and 4=over 60 minutes) and summed over both items to give a PA score ranging from 0 to 24.
For the current study, the Burdette parent proxy report instrument was modified in three ways. First, providers were asked to recall both indoor and outdoor active play. Second, the location of active play was delimited to the FCCH. Third, responses on the 5-point scale were recorded for just two time periods: arrival until lunch time and lunch time until departure. For each eligible child under their care, providers responded to the following question: “While under your care, how much time does this child spend actively playing (e.g., running, jumping, climbing) indoors or outdoors?” A single PA score ranging from 0 to 4 was calculated by averaging the responses for the two time periods.
Modified Harro proxy report
Harro developed and validated a parent and teacher proxy report instrument to assess physical activity in children 4–8 years of age. 14 Using an open-ended response format, parents reported the duration (minutes) of their child's low-to-moderate and moderate-to-vigorous indoor and outdoor activities performed in the home, whereas teachers reported the duration of low-to-moderate and moderate-to-vigorous indoor and outdoor activities performed at school. Daily MVPA was calculated by summing parent- and teacher-reported time in indoor and outdoor moderate-to-vigorous activities.
For the current study, the Harro teacher proxy report was modified by asking FCCH providers to recall time spent in the following five activity categories: sitting; low-to-moderate intensity indoor activities; low-to-moderate intensity outdoor activities; moderate-to-vigorous intensity indoor activities; and moderate-to-vigorous outdoor activities. For each activity category, examples of physical activities were provided. To assist with recall, the child care day was segmented into two time periods: arrival until lunch and lunch until departure. Daily MVPA was calculated by summing the provider-reported duration of moderate-to-vigorous indoor and outdoor activities during both time periods.
Accelerometry
Direct measurements of PA were obtained using the ActiGraph GT1M accelerometer (ActiGraph Corporation, Pensacola, FL). The ActiGraph accelerometer has been shown to be a valid instrument for assessing PA in preschool-aged children. 15 Monitors were initialized to a 15-second epoch to detect the spontaneous activities of 2- to 5-year-old children. Activity counts were uploaded to a customized data-reduction software program for the determination of daily time spent in MVPA and total PA (TPA; sum of light, moderate, and vigorous PA). Counts were classified into the aforementioned intensity groupings using the cut points developed by Pate and colleagues (sedentary, ≤37 counts per 15 seconds; light, 38–419 counts per 15 seconds; MVPA, ≥420 counts per 15 seconds). 16 Daily wear time was calculated by subtracting nonwear time from total monitoring time. Nonwear time was estimated by summing the number of consecutive zero counts accumulated in strings of 10 minutes or longer. Children were included in the analyses if they had 2 or more days in which wear time was ≥75% of attendance time.
Study Protocol
During a randomly selected week, children wore an accelerometer on the days they attended child care. At the beginning of each monitoring day, the provider attached the accelerometer to the child's right hip by an adjustable elastic belt, noting the time of attachment, the identification number of the child, and the identification number of the accelerometer. When the child left the FCCH, the provider removed the accelerometer and noted the time of departure. At the completion of the monitoring week, FCCH providers completed a proxy report instrument for each child who wore an accelerometer. The aforementioned protocol was implemented on two occasions. During the first data-collection period (study year 1), providers completed the modified Burdette proxy report. During the second data-collection period (study year 2), providers completed the modified Harro proxy report.
Statistical Analysis
Associations between provider-reported physical activity and objectively measured PA were assessed using partial Pearson correlations. In addition, one-way analysis of covariance was used to evaluate differences in objectively measured physical activity across tertiles of FCCH provider-reported physical activity. All analyses were adjusted for differences in daily wear time and were completed using SAS statistical software (Version 9.3; SAS Institute, Cary, NC). Statistical significance was set at an alpha level of 0.05.
Results
Sample Characteristics
A total of 37 providers completed the modified Burdette proxy report in year 1, whereas 42 providers completed the modified Harro proxy report in year 2. Twenty-seven providers completed proxy reports in years 1 and 2. As shown in Table 1, samples were comparable with respect to median years of operation, number of preschool-aged children under care, provider age, provider education, race and ethnicity, and participation in a government-subsidized food program (Child and Adult Care Food Program).
Demographic Characteristics of Family Child Care Home Providers
Abbreviations: FCCH, family child care home; GED, general educational development; CACFP, Child and Adult Care Food Program; IQR, interquartile range.
Table 2 displays the sample characteristics for children with valid accelerometer data and complete data for the provider proxy reports in years 1 (Burdette) and 2 (Harro), respectively. Consistent with the sample's slightly older age, children in the year 2 sample were slightly heavier and taller and had a marginally higher BMI than children in the year 1 sample.
Descriptive Statistics of Children Completing the Accelerometer Protocol
Accelerometer counts were classified into the aforementioned intensity groupings using the cut points developed by Pate and colleagues 16 (sedentary, ≤37 counts per 15 seconds; light, 38–419 counts per 15 seconds; moderate-to-vigorous, ≥420 counts per 15 seconds).
Abbreviations: MVPA, moderate-to-vigorous physical activity; TPA, total physical activity or sum of light, moderate, and vigorous physical activity.
Descriptive Results
Based on the accelerometer data, children in the Burdette (year 1) sample accumulated 45.0±21.8 minutes of MVPA and 164.2±57.6 minutes of TPA per day. Average wear time was 4.9±1.5 hours per day. The mean provider-reported PA score from the modified Burdette proxy report was 3.3±0.8. Scores ranged from 1.0 to 4.0. Children completing the accelerometer protocol year 2 sample accumulated 47.1±28.2 minutes of MVPA and 164.1±73.0 minutes of TPA per day. Average wear time was 5.3±1.8 hours per day. The mean provider-reported MVPA level from the modified Harro proxy report was 62.9±47.7 minutes per day. MVPA estimates ranged from 0 to 270 minutes per day.
Concurrent Validity
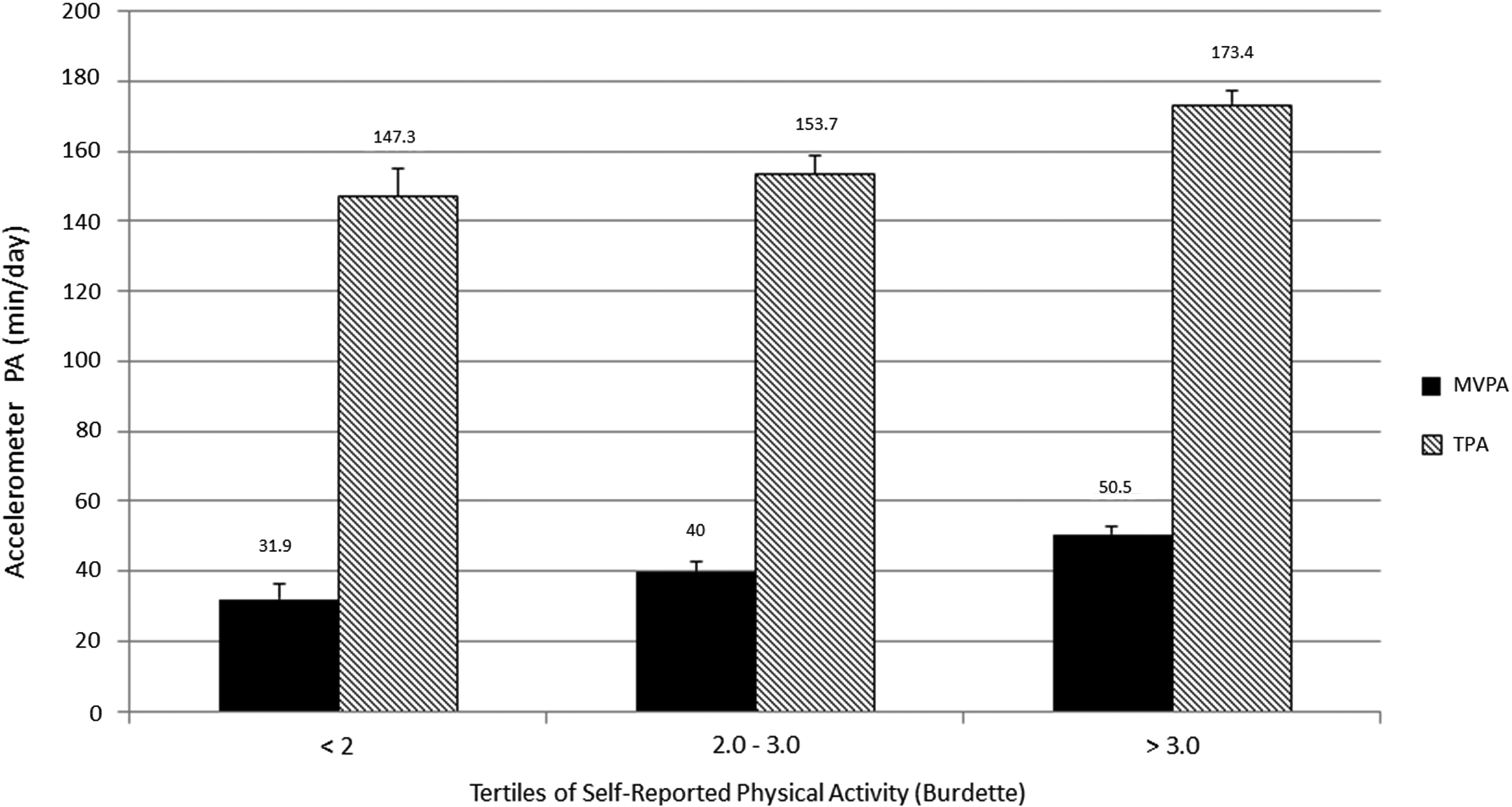
Significant positive correlations were observed between provider-reported PA scores from the modified Burdette proxy report and objectively measured TPA (r=0.30; p<0.01) and MVPA (r=0.34; p<0.01). Across tertiles of the Burdette PA score, objectively measured TPA (F(1, 103)=9.01; p=0.003) and MVPA (F(1, 103)=13.8; p=0.0003) increased significantly in a linear dose-response manner (Figure 1).
Provider-reported MVPA scores from the modified Harro proxy report were not associated with objectively measured PA. Correlations between provider-reported MVPA and objectively measured TPA and MVPA were (r=0.09; p=0.30) and (r=0.10; p=0.25), respectively. Across tertiles of Harro MVPA scores, there were no significant differences in objectively measured TPA (F(1, 127)=1.36; p=0.24) or MVPA (F(1, 127)=1.56; p=0.21; (Figure 2).

Discussion
To our knowledge, this is the first study to evaluate the concurrent validity of two brief proxy report instruments designed to measure PA in preschool-aged children attending FCCHs. The results indicate that the Burdette parent proxy report, modified for the family child care setting, has moderate evidence of relative validity. In contrast, the modified Harro proxy report was not associated with objectively measured PA. These findings suggest that the modified Burdette proxy report may be a useful measurement tool in larger scale PA studies involving FCCHs in which objective measures, such as direct observation or accelerometry, are not practical.
In absolute terms, the validity coefficients for the modified Burdette proxy report are modest. However, the magnitude of the observed correlation coefficients (r=0.30–0.34) are similar to those reported for other self-report instruments for older children. 17 Moreover, the validity coefficients are comparable to those reported by Burdette for parent responses. In that study, the correlation between parent reports of outdoor playtime, as measured by a two-item checklist, and objectively measured PA (tri-axial accelerometry) was r=0.33. 13 Therefore, the results of the current study are consistent with those obtained in previous validation studies of PA self-reports and support the contention that, in situations where more burdensome objective measures are not feasible, relatively simple, easy-to-administer proxy report instruments can be used to measure relative participation in PA among preschool-aged children.
The results are also in agreement with previous studies validating proxy report measures in teachers working in center-based child care settings. Tulve and colleagues 18 assessed the feasibility and validity of a teacher-completed activity diary in infants and toddlers 4–17 months of age. For each 30-minute block within a day, teachers recorded the predominant activity level on a 4-point scale (1=sleep, 2=eating, 3=quiet play, and 4=active play). In addition, teachers recorded the location in which activity took place (home-inside, home-outside, or away from home). The diaries were completed over 4 consecutive days, including both weekend days and 2 weekdays. During this time, children wore an accelerometer on either the hip or ankle. Teachers were encouraged to complete the activity diary in real time. Teacher-reported estimates of daily activity level were significantly and positively correlated with accelerometer output (Spearman's r=0.42; p<0.001). Chen and colleagues 19 examined the validity of teacher-reported physical activity in a sample of 21 Japanese preschool children. Children wore an accelerometer and a pedometer for 3 consecutive days while attending preschool. At the completion of the 3-day monitoring period, teachers completed a three-item questionnaire assessing each child's preference for activity (1 “like very much” to 3 “do not like”), frequency of PA (1 “very often” to 3 “not often”), and intensity of PA (1 “very active” to 4 “inactive”). Children rated by teachers as “very active” exhibited significantly higher accelerometer counts and pedometer steps than children rated by teachers as “inactive.” Although the results of these two studies support the utility of proxy reports for preschool-aged children, it is important to note that both of these studies included very small samples of teachers and children. Moreover, the proxy reports evaluated in these studies were more burdensome than the measures evaluated in the current study.
The modified Harro proxy report was not significantly correlated with objectively measured PA, nor was there a significant linear trend across tertiles of provider-reported PA. The low validity of this measure may be attributable, at least in part, to the open-ended response format which required providers to recall the duration each child spent in sedentary, light-to-moderate, and moderate-to-vigorous intensity PA. Notably, as part of their evaluation of outdoor play assessment, Burdette and colleagues 13 evaluated a parent recall consisting of two open-ended questions about the duration of outdoor play. Relative to the close-ended checklist format, the open-ended items yielded a substantially lower correlation with objectively measured PA (r=0.20 vs. r=0.33). Therefore, the results of this study, as well as those from Burdette, suggest that the use of a fixed checklist format, which delimits the duration of responses to specific values, or a range of values, may be important in enhancing the accuracy of child care provider's self-reports of children's PA level during the child care day.
The present study had several strengths. First, the study was conducted in a unique study population of family child care providers. To date, studies validating proxy-report measures for children under age 5 have been conducted exclusively with parents or teachers working in center-based child care. Second, in contrast to previous validation studies, which involved a very small number of teachers and children, the present study involved two relatively large samples of FCCH providers and child care attendees. Last, the validity of two contrasting reporting formats (checklist vs. open ended) was examined, providing guidance as to the design of simple physical activity proxy-report tools for young children.
Offsetting these strengths were several limitations. First, although FCCHs were recruited from seven economically diverse counties in the state of Oregon, the sample was not ethnically diverse, with close to 90% of the providers identifying themselves as non-Hispanic white. Second, although accelerometers provide valid estimates of PA in preschool children, the use of accelerometers as a criterion measure of PA is not without limitations. Accelerometers do not fully capture the increased energy cost of climbing over structures, walking up stairs, or riding tricycles. In addition, there continues to be no consensus with respect to the application of cut points for preschool-aged children. 20 Importantly, the present study used the Pate and colleagues 16 cut points to estimate PA intensity, which are the only published cut points for preschool-aged children based on directly measured energy expenditure.
Conclusion
In summary, caregiver responses on the Burdette parent proxy report, modified for use in FCCH providers, were positively and significantly correlated with objectively measured PA in preschool children. Provider reports of child MVPA on the modified Harro proxy report were not associated with objectively measured PA. Although acknowledging the limitations of self-report instruments, the modified Burdette proxy report may be a useful PA assessment tool in large-scale intervention trials or population-based PA surveillance studies in which more burdensome objective measure are not feasible. Future studies should test the validity of the modified Burdette proxy report in larger, more diverse samples of FCCH providers as well as evaluate the measure's sensitivity to change.
Footnotes
Acknowledgments
Funding for this study was provided by a grant from the US National Institute of Food and Agriculture (NIFA; 2009-55215-05311).
Author Disclosure Statement
No competing financial interests exist.