
Abstract
Abstract
Background:
Immersion treatment (IT) provided in a camp setting has been shown to promote short-term improvements in weight and health status in obese adolescents. However, evidence of IT's long-term efficacy and efficacy for multi-ethnic and lower socioeconomic status (SES) adolescents is limited.
Methods:
This was a cohort study with a pre/post design and longitudinal follow-up. The intervention was a 19-day camp-based IT program comprising (1) a nutrition curriculum and ad-lib access to a nutritious diet, (2) several hours of physical activity daily, (3) group therapy, and (4) cognitive-behavioral therapy (CBT). This analysis included 52 low-SES adolescents that participated in 2009 and 2010. A subgroup of 33 campers and their families was offered follow-up monthly for 10 months. Primary outcome measures were change in weight-related parameters immediately postcamp and after 10 months of follow-up.
Results:
Campers had significant short-term improvements in mean waist circumference (mean [M], 2.6; standard deviation [SD], 3.2 cm), weight (M, 2.6; SD, 1.9 kg), BMI (M, 1.1; SD, 0.9 kg/m2), BMI z-score (M, 0.06; SD, 0.07), and percent overweight (M, 6.1; SD, 4.7). Campers offered follow-up had a modest increase in mean percent overweight (M, 2.0; SD, 8.4) during 10 months of follow-up. However, 33% experienced continuing decline in percent overweight during follow-up, and long-term follow-up was associated with significant overall (precamp vs. end of follow-up) improvements in percent overweight (M, 4.9; SD, 7.2).
Conclusions:
Camp-based IT with CBT is a promising intervention for improving short- and long-term weight status of low-SES adolescents. Additional research is needed to increase long-term efficacy.
Introduction
The prevalence of obesity (BMI ≥95th percentile for age and sex) in 12 to 19 year olds in the United States is currently 18.5% 1 with higher rates for rural,2,3 minority, 1 and low socioeconomic populations. 4 Consistent with these risk factors for obesity, direct anthropometric assessment of 1656 seventh graders enrolled in an integrated, interdisciplinary, school-based approach to student wellness5,6 in rural, racially diverse middle schools in eastern North Carolina revealed that 31% were obese, with an additional 10.2% meeting criteria for severe obesity (BMI ≥99th percentile). The prevalence of both obesity and severe obesity in this population was the highest among African American girls (37.8% and 14.4%, respectively; Hardison G, Lazorick S, Crawford Y, unpublished data, October 2013). Durable improvement in weight status was documented for 66–75% of overweight and obese adolescents enrolled in participating schools. 5 However, severely obese adolescents were less responsive to this program and likely need more intensive interventions, 7 such as comprehensive multidisciplinary intervention, tertiary care intervention, possibly including use of medications, very-low-calorie diets, bariatric surgery, or immersion treatment.
Immersion treatment (IT) has been defined as “an intervention or program designed to produce therapeutic change in weight that includes 24-hour attendance for at least 10 consecutive days” and may include inpatient, residential, and camp-based immersion components.8,9 Programming typically includes reduced caloric intake, increased physical activity, behavior modification principles, and parental or familial components.8,9 Camp-based IT has demonstrated success in helping obese adolescents achieve both short-10–16 and medium- to long-term improvements in weight status.15,17,18 In a review of pediatric IT programs, children and adolescents participating in camp-based IT programs were reported or estimated to have a decline in percent overweight of 3–21% immediately postintervention (treatment duration ranging from 10 days to 8 weeks) and an overall decline in percent overweight of 12–21.8% between baseline and final follow-up (follow-up duration ranging from 9 months to 3.6 years).8,15 However, with certain exceptions,13,14 studies reporting outcomes for camp-based IT included predominantly high socioeconomic status (SES) and white subjects. Hence, their efficacy for low-SES, racially diverse populations is largely untested. Therefore, there is a need for better understanding of the effect of IT on objective outcomes in high-risk populations.
The purpose of this study is to (1) describe the development of a 3-week summer camp-based IT healthy lifestyle and weight management program targeting a severely obese, low-SES multi-ethnic population and (2) evaluate short-term objective changes in all participants' weight status across the 19-day IT phase as well as long-term changes in weight status in a subset enrolled in a 10-month follow-up program.
Methods
Setting and Participants
The initial intervention included a 3-week (19-day) residential, immersion weight management summer camp, called Take Off 4-Health (TO4H), housed at the Eastern 4-H Center in rural, eastern North Carolina. 19 As with other IT programs, a major focus of TO4H was on developing autonomous problem-solving and behavioral choice skills that were expected to promote maintenance of healthier behaviors and improved weight status once campers returned to their family and community environment. 9 Specific components of TO4H included nutrition education, physical activity, cognitive-behavior modification strategies, self-monitoring, and group therapy, which are described in detail in the ensuing paragraphs. A unique feature of TO4H was ad lib dining, rather than plated food. This less-structured approach to nutrition was adapted to allow campers the opportunity to practice newly acquired nutrition knowledge and skills in a realistic, supportive, educational environment. The multidisciplinary intervention team included 4-H center staff, nutritionists, clinical health psychologists, medical family therapists, physical therapists, and medical staff from an academic medical center.
This study was approved by the University Medical Center Institutional Review Board (no. 08-0409) at the Brody School of Medicine (Greenville, NC). All participants and their parent or legal guardian provided previous written informed assent and consent, respectively.
Criteria for participation included (1) age of 12–18 years (minimum age of 12 for 4-H facilities' liability insurance) and (2) obesity (BMI ≥95th percentile for age and sex). Though available to self-pay campers, the majority of campers received a full or partial scholarship. Eligibility for a scholarship required (1) evidence of financial need or low SES, as determined by insurance status, household income, or special extenuating circumstances, and (2) residence within a county served by the various supporting foundations (see Acknowledgments section). Cost of the program, inclusive of 19 days at camp with programming, laundry service, transportation, shorts and T-shirts, pedometers, and educational materials, but exclusive of the value of faculty time and other in-kind contributions, was $2,250 and $2,500 in 2009 and 2010, respectively. Funding was received from local foundations and private donors. Candidates for scholarships were identified through East Carolina University's Pediatric Healthy Weight Research and Treatment Center (Greenville, NC), primary care practices, health departments in eastern North Carolina, school nurses, and case management programs or were self-referral. Candidates and their families were interviewed by a multidisciplinary team, comprising a physician, social worker, psychologist, and medical family therapist. Adolescents assessed as precontemplative 20 or uninterested in making healthy lifestyle changes, or disruptive and/or potentially violent, were excluded from consideration for a scholarship.
Ninety potential candidates seeking scholarship were identified; of these, 49 received full or partial financial support. The most common reasons, in order, for not receiving financial support were (1) failure to show up for interview, (2) adolescent not interested in going to camp or not interested in making change, (3) parent unwilling to be separated from child for 3 weeks, and/or (4) a history of disruptive or aggressive behavior in the adolescent.
A total of 52 obese adolescents enrolled in TO4H across the summers of 2009 and 2010. Demographics, including self-identified race/ethnicity, are shown in Table 1. Campers were mainly female and African American. Eighty-five percent came from families earning below the US median income 21 and 67% from families with annual household income of less than $30,000. Though the extent of obesity varied broadly (Table 2), the majority (69%) of campers were severely obese, as defined by BMI ≥99th percentile. The mean values for BMI (40.4), BMI z-score (2.46), and percent overweight (106.0) were quite high. Demographic and weight-related parameters for the subgroups attending camp only and camp with follow-up did not differ significantly. Although many participants had no known major obesity-related comorbidities, 5 had type 2 diabetes, 3 had obstructive sleep apnea requiring continuous positive airway pressure, 2 had psychiatric diagnoses requiring treatment with atypical antipsychotics, and 1 had Blount's disease. A majority had lower-extremity dysfunction and/or gait abnormalities, as previously described.22,23
Baseline Demographics of Participants
Based on residency restrictions imposed by the funding foundation, only 33 of 52 campers were eligible for the long-term follow-up program.
Because of rounding not all percentages add to 100%.
SD, standard deviation.
Baseline Anthropometrics
Values are mean±standard deviation and (minimum, maximum).
Based on residency restrictions imposed by the funding foundation, only 33 of 52 campers were eligible for the long-term follow-up program.
Nutrition
The nutrition component of TO4H included a nutrition education curriculum, modified diet, and “camper meal cards” and has been described in detail elsewhere. 24 Briefly, the nutrition curriculum included six 1-hour-long lessons with relevant activities addressing the use of the “camper meal card,” portion sizes, sugar-sweetened beverages, fruit and vegetable intake, eating out, and reading food labels. The camper meal card was a personalized nutrition prescription to guide food choices and portion sizes at meal and snack times both at camp and at home. Age- and gender-appropriate calorie levels were derived from the USDA MyPyramid Calorie Levels employing a sedentary activity level. 25 For 9- to 13- and 14- to 18-year-old girls, these were 1600 and 1800 kcal per day, respectively, and for boys, 1800 and 2200 kcal per day, respectively. 26 Because of the high level of activity at camp, these caloric targets were estimated to result in a deficit of at least 200–600 kcal per day for girls and 200–1000 kcal per day for boys. Campers could achieve these caloric targets by following their personalized nutrition prescription on their camper meal card, which guided their daily servings of each food group based on the MyPyramid food intake patterns. Researchers worked with the 4-H center's food service manager to modify food choices at meals based on the 2005 Dietary Guidelines for Americans. 26 Modifications included offering low-fat, low-sugar foods as well as whole grain foods higher in fiber. All meals included salad and fresh fruit options. Food preparation techniques were modified to target a total fat intake between 25 and 35% of total calories, carbohydrates between 45 and 65% of total calories, and protein between 10 and 35% of total calories. Family-style dining, which is 4-H center tradition, was utilized. All food was served in large serving bowls in the center of each table. Serving bowls could be refilled resulting in true ad lib dining. A nutrition graduate student, working under the direction of a registered dietician, served as “nutrition coach” in the dining hall to assist campers in applying skills learned in classes and appropriate use of their camper card. Additionally, each family received a packet of helpful resources for continued success, including a magnet with healthy tips, tear-off shopping lists, a magazine, compact disc, meal-planning whiteboard, and 450-lb capacity scale. 24
Physical Activity Programming
Campers participated in five activity periods per day, including typical camp activities such as swimming, kayaking, group games, rock wall climbing, archery, basketball, volleyball, hiking, and relay races. At least two periods per day were spent doing pool activities because these were lower impact and alleviated discomfort and risk from heat. Walking to/from the dining hall, cabins, and activity areas contributed significantly to daily physical activity. In 2010, an exercise physiology intern, working under the direction of a PhD-level licensed physical therapist, served as a “physical activity counselor.” The intern taught two classes about healthy, community/home-based physical activity and modified activities, as needed, to reduce excessive joint loading, reduce risk of musculoskeletal injuries, and provide alternative physical activity, such as lifting light weights or using dynabands, if a camper could not participate in scheduled activity. Sports and group games were also modified to accommodate the significantly reduced mobility and generally low skill level of the obese adolescents served. For example, volleyball, which requires mobility and skill to enjoy, was changed from hitting to catching and throwing the ball (known as “Newcombe”).
Cognitive Behavioral Therapy
Campers participated in weekly group-based cognitive behavioral therapy (CBT) and individual CBT sessions daily. During group sessions, graduate students in clinical health psychology, referred to as “lifestyle coaches,” used cognitive behavioral strategies to help campers learn how to monitor eating and activity, set appropriate goals, and use problem-solving skills effectively. Campers filled in worksheets related to weekly topics, discussed progress, participated in group discussion and activities, and encouraged one another.
CBT group session time was spent teaching and discussing topics such as keys to success, self-talk, and understanding thoughts, feelings, and behavior chains. Campers participated in related activities and were encouraged to reflect on ways these factors could influence their behavior and health, incorporating new skills into weekly goals, when appropriate. Campers also learned and practiced specific behavioral self-regulation skills first within the CBT group session and then throughout the day on their own, with assistance from lifestyle coaches when needed.
Campers learned to self-monitor both food intake and activity levels. They used a camper-friendly food record, which allowed them to tally servings of food groups at each meal and calculate daily and weekly totals for comparison with their camper card. A pedometer, together with time spent doing water-based activities, was used to monitor their total daily activity level. The lifestyle coaches were present at meals to assist campers with accurate monitoring, including recording and interpreting pedometer step counts and minutes of water-based activity, and recording daily and weekly totals in their food diary. Campers used these food and physical activity totals to set weekly behavioral goals and monitor progress. Goal-setting skills were taught, practiced, and shaped in CBT group sessions. Campers were taught to make goals using the SMALL acronym: Self-selected, Measurable, Action-oriented, Linked to your life, and Long-term. 27 Problem-solving therapy 28 was also used to assist campers to overcome challenges and obstacles that hindered goal achievement as well as in preparation for future challenges upon returning to the home environment. At the end of each day, campers met with their lifestyle coach for a 15-minute individual session to review their day, discuss successes and challenges, and to goal set for the next day.
In recognition that an integral part of changing health behavior for adolescents is the family environment, a half-day “family day” or workshop was included at camp in 2010. Families received information about important skills learned and changes made by campers and then worked together to establish a plan to ensure success upon reintegration into the home environment.
Group Therapy
Group therapy was added to individual and group CBT to facilitate interpersonal skills acquisition. 29 Campers participated in group therapy sessions led by master's- and doctoral-level medical family therapists two times per week. Groups were divided by age and gender. Topics, as previously described, 30 included rapport building, self-esteem, body image, bullying, and teasing, and relationships and using social support. The focus of group therapy was skill building relevant to inter-relational challenges campers may face with peers, family, and other community elements. Group sessions were also used to process issues that arose during the preceding days at camp.
Follow-Up Intervention
A local grant-funded pediatric healthy weight case management program provided 10-month postcamp follow-up for a subset of 33 campers. Although campers resided in numerous counties in North Carolina, the terms of the grant allowed enrollment of only residents of Pitt County, North Carolina. Before the camp follow-up, the program invited parents of campers to attend three evening sessions while youth were at TO4H. These sessions provided an overview of the nutrition, physical activity, and psychosocial components of camp and other activities to foster a supportive, healthy environment for campers upon return home. The follow-up program was provided by an interdisciplinary team (nutritionist, nurse, and social worker) and consisted of 10 monthly meetings with campers and their families to provide support, reinforcement, accountability, and education. Educational topics included health risks of obesity, the Food Guide Pyramid, healthy eating away from home, preparing healthy meals and snacks, self-esteem and coping, effective communication, emotional eating and eating disorders, and identification of familial/community support systems and resources. Campers and a parent/guardian were also given the opportunity to exercise at a local wellness facility at very low cost, and case management services were provided as needed. Height and weight were measured at each monthly meeting.
Design
This was a cohort intervention study with pre/post design and longitudinal follow-up.
Measures
Participants dressed in light clothing were weighed before breakfast on a seca model 703 digital scale (Seca GmbH & Co. KG, Hamburg, Germany) in kilograms to the nearest 0.1 kg; height was measured in centimeters to the nearest millimter with a Seca model 220 integrated mechanical measuring rod. Waist circumference was measured in centimeters to the nearest millimeter over light clothing at the level of the iliac crest with a Gulick tape measure. Pre- and postcamp waist circumference measurements were made by the same two individuals following instruction by, and under the direct observed supervision of, the senior investigator (D.N.C.). The procedure was not standardized between individuals. Percent overweight was calculated as
Statistical Analysis
Changes in BMI z-score in a single group were analyzed using the one sample t-test with the 95% confidence interval (CI) for the mean difference. This analysis was used for all numeric variables. Numerical summaries were provided on various subgroups of the data. Formal statistical analyses were confined to the comparison of two groups. For these comparisons, the two-sample t-test, along with the associated 95% CI was used to compare changes in BMI z-score, percent overweight, and other numeric variables. For dichotomous variables, such as gender, groups were compared using Fisher's exact test along with 95% CIs for the odds ratio. All calculations were done using version 3.0.1 of the statistical software R. 31
Three enrollees were asked to leave before completion of camp for behavioral reasons. Assessment of short-term outcomes employed an intention-to-treat (ITT) analysis comprising actual end-of-camp measurements for the 49 completers and baseline measurements carried forward for the three noncompleters. 32 Evaluation of long-term outcomes (n=33) employed both an ITT analysis, in which baseline BMI z-score and percent overweight were used as final measures for noncompleters (n=10), as well as analysis of completers (n=23) only.
Results
Compared to physical activity at home, as assessed by daily step counts recorded for the week before attending camp (mean [M], 6273; standard deviation [SD], 2325), the TO4H program resulted in significantly higher levels of physical activity with daily step counts averaging 15,963 (SD, 4164) and an average of 82 minutes (SD, 25.1) of pool time recorded daily. Overall, campers demonstrated a significant reduction in BMI, BMI z-score, and percent overweight from baseline to the end of the initial intervention (Table 3). Campers lost an average of 2.6 kg (SD, 1.9) over the 19-day program. Weight change ranged from 1.1 kg gained in 1 camper taking an atypical antipsychotic to 8.7 kg lost. Campers also demonstrated a significant reduction in mean waist circumference of 2.6 cm (SD, 3.2) from baseline to the end of the initial intervention. Examination of outcomes by ethnicity revealed a significant reduction in pre- versus postcamp BMI z-score for both white (M 2.42 vs. M 2.36; t(11)=3.19; p=0.009) and African American (M 2.48 vs. M 2.42; t(29)=6.51; p<0.001) participants. Girls trended toward greater reduction in waist circumference than boys (M 3.0 vs. M 1.77 cm; p=0.11), whereas boys had significantly greater improvements in percent overweight than girls (M 8.7 vs. M 5.1; p=0.037). Boys also trended toward greater reductions in BMI (M 1.6 vs. M 1.0 kg/m2; p=0.07) and BMI z-score (M 0.10 vs. M 0.05; p=0.14) than girls. Weight loss for boys and girls was similar (M 3.0 vs. M 2.5 kg; p=0.44).
Short-Term Change in Weight-Related Parameters
Values are mean±standard deviation and (95% confidence interval [CI]) for postcamp versus baseline.
Based on residency restrictions imposed by the funding foundation, only 33 of 52 campers were eligible for the long-term follow-up program.
Thirty-three campers enrolled in the follow-up program comprised the long-term subset. Eleven campers (33.3%) attended ≤3 follow-up meetings, 10 (30.3%) attended 4–6 meetings, and 12 (36.4%) attended ≥7 meetings. None attended all 10 meetings and 1 did not attend any meetings. Mean and median number of meetings attended was 4.8 and 5, respectively. Campers were considered completers if they were present at the ninth and/or tenth session. Twenty-three (70%) were available for a final assessment (mean, 9.5 months postcamp) and were included in the long-term outcome analysis as “completers.” For an ITT analysis (n=33), baseline percent overweight or BMI z-score was carried forward and used as the final value for the 10 participants missing final measurements. Baseline BMI z-score, rather than a standard last observation carried forward (LOCF) approach whereby the last available BMI z-score is used as the final value, was chosen to avoid overestimation of effect inherent in the LOCF method. 32 Campers enrolled in follow-up demonstrated significant short-term improvements in BMI z-score and percent overweight (Table 3), but experienced a modest (2.0±8.4) increase in percent overweight during 10 months of follow-up postcamp. However, when compared to baseline, participants had a significant decline in percent overweight at the end of follow-up (M 4.9, SD 7.2, p=0.0004 all enrolled; M 5.2, SD 8.6, p=0.008, completers; Fig. 1). Eleven (48%) participants in the completers group had continued declines in percent overweight during postcamp follow-up (M, 7.8; SD, 5.2). Long-term BMI z-scores also trended down (M 0.04, SD 0.11, p=0.07, all enrolled; M 0.05, SD 0.13, p=0.07, completers).
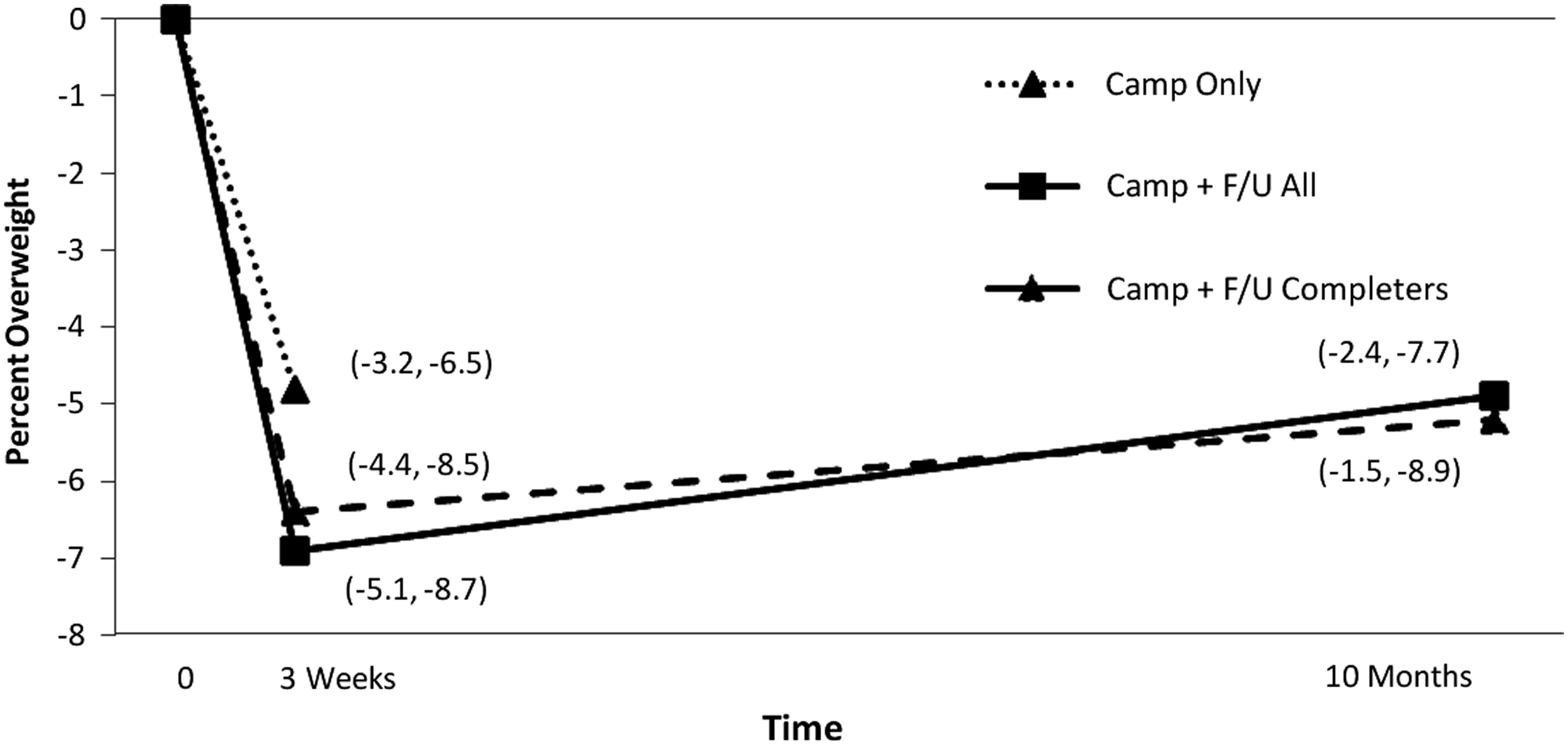
Short- and long-term change in mean percent overweight with 95% confidence intervals (95% CI).
Discussion
Our model focused on promoting sustainable health behavior change in cohorts comprising predominantly severely obese, low-SES, African American adolescents. Overall, participants demonstrated clinically and statistically significant reductions in weight, waist circumference, BMI, BMI z-score, and percent overweight across the 19-day initial camp-based IT program. Average weight loss was 2.6 kg, and the average rate of weight loss of approximately 0.98 kg (2.3 lb) per week closely matches the rate of weight loss endorsed for adolescents with BMI ≥95th percentile. 7 These findings are consistent with previous reports of short-term weight loss success for immersion programs, especially those including CBT,8,9 and extend the current literature,13,14 confirming that a lifestyle approach to weight management can successfully assist a high-risk population in achieving short-term improvements in weight status. There were no significant differences in short-term responsiveness between white and nonwhite adolescents. However, boys had significantly greater change in percent overweight than girls. This is the result, in part, of the use of an ITT analysis (all of the boys completed TO4H, whereas all 3 of the noncompleters were girls). The 6.9% decline in percent overweight for these campers is similar to the mean 8.2% immediate post-treatment decline in percent overweight achieved by out-patient lifestyle interventions. 33 However, the extent of weight loss was less than that reported for other camp-based IT programs (ranges from 3.713,14 to 11.6 kg 15 ). Longer duration of treatment is associated with greater weight loss8,10; hence, the relatively short 2.7-week duration of TO4H likely contributes to smaller improvements in weight status. However, we calculate that average rate of weight loss per week for other camp-based IT programs is also higher than the 0.98 kg/week observed in this study (ranging from 1.511 to 1.915 kg/week), including 1.85 kg/wk for the 2-week Kamp K'aana program.13,14
Several aspects of TO4H are unique and may contribute to smaller improvements in weight status. First, with a mean BMI of 40.4, mean BMI z-score of 2.46, and mean percent overweight of 106%, we believe this to be the most severely obese cohort receiving camp-based IT reported to date. This degree of obesity is frequently associated with lower-extremity dysfunction, which may limit physical activity and contribute to the maintenance of obesity. Second, this is the first study in which a majority (59%) of participants was African American and the majority was from low-SES families. Finally, to the best of our knowledge, this is the only camp-based IT program to employ an unrestricted ad lib approach to eating. Other programs, such as Wellspring Camps, do allow unrestricted consumption of certain foods, including salads, fruits, fat-free protein, and very-low-fat soups. 15 Kamp K'aana, a 2-week IT program serving a multi-ethnic population of whom 50% were considered underserved, also offered unlimited access to a salad bar throughout camp as well as unrestricted ad lib dining on the last 2 days of camp in order to practice newly acquired nutrition knowledge and skills.13,14 As with Kamp K'aana, TO4H employed ad lib dining (but across the entire 2.7 weeks) as a means of developing and applying nutrition skills in the controlled, educational environment of camp. Low-fat diets (≈20–25% of total calories from fat) can contribute to modest, but significant, improvements in energy balance, can be sustained over the long term in some instances, and can contribute to both weight loss maintenance and improved health. 34 Hence, some IT programs, such as Wellspring Camps, employ a very-low-fat diet (≈7% of total calories from fat) 15 that may contribute to their higher rates of weight loss. However, dietary adherence (together with behavior modification and physical activity) is thought to be more important than macronutrient content for obesity management.34,35 Hence, TO4H employed a “lower-fat” diet, comprising 25–35% of total calories from fat, rather than low fat or very low fat, because it was felt to be achievable by most families served and more compatible with long-term adherence. This macronutrient content is also well below the threshold (58% of calories from fat) associated with dysregulation of satiety pathways that results from long-term consumption of a high-fat diet. 34
Caloric targets and the appropriate number of servings from various food groups were established for each camper in 2009 and 2010 using the USDA's MyPyramid method. In 2011, MyPyramid was replaced by the USDA's MyPlate method. 36 Whereas the MyPlate method is less focused on portion control and portion sizes than MyPyramid, we expect that use of MyPlate would yield similar results.
Given that 35% of African American children and 40% of low-SES children experience food insecurity, and that North Carolina is a state that has had substantial recent increases in food-insecure households, 37 it is likely that many of the TO4H participants experience food insecurity. Though the quality and consistency of meal-time recording at camp was not adequate to determine actual daily intake, we have witnessed excessive eating, with resultant weight gain, during the first 2 weeks of camp among numerous campers. Though not specifically assessed, we speculate that household food insecurity may contribute to this early overeating and may explain, in part, the lower rates of weight loss observed with this program. However, further research, including more accurate recording of intake and screening for food insecurity and eating disorders, is needed to support this contention.
Seventy percent (23 of 33) of participants offered long-term follow-up were available for final measurements. During the 10-month follow-up, completers had a mean 1.3 increase and all participants (ITT) a mean 2.0 increase in percent overweight. These results are somewhat better than the postcamp increase of 9.0 calculated by Kelly and Kirschenbaum 8 based on the 11 months of follow-up reported by Gately and colleagues, 17 similar to the 3.0 increase calculated 8 for 3.6-year follow-up reported by Braet and Van Winckel, 18 but less robust than the 21.5 and 22.0 declines reported by Kirschenbaum and colleagues during the 6–9 months of follow-up reported for Wellspring Camps. 15 A substantial fraction (48%) of the completers had continued decline in percent overweight during follow-up. The average additional postcamp decline during follow-up for this group was 7.8.
Kirschenbaum and colleagues have proposed an “immersion-to-lifestyle change model,” in which three key external/environmental elements interact with and influence three key internal/personal elements. The external elements are IT, CBT, and social support. The internal elements are rapid and consistent weight loss, developing a so-called healthy obsession and making long-term lifestyle change. According to this model, IT—especially IT employing CBT—allows the individual to achieve rapid weight loss. This weight loss, together with skills developed through CBT, results in cognitive and emotional changes producing a commitment to a healthy lifestyle, or a “healthy obsession.” When coupled with adequate social support, this commitment results in sustainable lifestyle changes yielding long-term improvements in weight status.9,38
Given that almost half of the completers demonstrated continued postcamp improvements in percent overweight, we conclude that the relatively modest rates of weight loss achieved with this IT program, in concert with the CBT programming, are sufficient to promote the increases in self-efficacy that result in a healthy obsession (or commitment to long-term change) that may lead to permanent lifestyle changes if/when adequate social support is also provided. Interestingly, participants who continued to have postcamp improvements in weight status had less short-term weight loss than participants with postcamp increases, suggesting that short-term weight loss was not the limiting factor in determining overall success for this cohort. We speculate that social support may be a rate-limiting component, especially for high-risk, low-SES populations, and is an area in need of improvement. Indeed, African American girls participating in TO4H identified family involvement in goal setting and motivation as important for success and that feelings of isolation and deprivation were barriers to success in adopting healthy lifestyle behaviors. 39 Hence, identifying and addressing discrepancies between a specific adolescent's self-identified needs and their family functioning (i.e., social support) may improve durability of health behavior change and warrants additional research. We have shown that providing CBT by telephone promotes weight loss and weight loss maintenance in high-risk veteran populations40–42 and propose that telephone-based CBT may be particularly useful for enhancing social support post-IT in sparsely populated rural regions, such as eastern North Carolina.
Limitations and Strengths
This study has several limitations. First, and most significant, is the lack of control or comparison group that receives either no treatment or an alternative weight management program. Second, it involves a relatively small number of participants; and third, only 23 of the 33 participants in the long-term subset were available for 1-year follow-up. Strengths are that it focuses on severely obese, low-SES adolescents and so extends the generalizability of IT-based outcomes, reports only directly measured anthropometrics (vs. self-report), and includes an ITT analysis for both short- and long-term results.
Conclusions
Results from TO4H confirm that an immersion program utilizing a lifestyle approach can yield successful short-term improvements in weight status in low-SES, high-risk adolescents. Long-term outcomes suggest that minimal monthly follow-up may help reduce the weight regain typically associated with short-term programs. More extensive, and/or tailored care, may be necessary to promote continued improvement in weight status. Randomized controlled trials are needed to evaluate the relative contributions of each element in the immersion to lifestyle change model. Studies are also needed to examine how biological-, behavioral-, and relational-associated factors affect retention in long-term treatment programs and treatment response.
Footnotes
Acknowledgments
The authors acknowledge the generous support received from the Pitt Memorial Hospital Foundation, Roanoke Chowan Hospital Foundation, Children's Miracle Network, Bank of America, and private donors for development of Take Off 4-Health. The long-term follow-up component was supported by a grant from the Duke Endowment. The authors also acknowledge their appreciation of Mr. Chase Luker, of North Carolina State University, for his contributions to scheduling and managing the inevitable challenges that arise when managing adolescent campers; Emily Steinbaugh, PhD, of East Carolina University for her role in coleading CBT programming; and Kathy Kolasa, PhD and Ms. Nancy Harris, of East Carolina University, and Carolyn Dunn, PhD, of North Carolina State University, for their work on developing the nutrition curriculum.
Dr. Collier's and Ms. Crawford's work was supported, in part, by a grant from the Pitt Memorial Hospital Foundation.
Author Disclosure Statement
No competing financial interests exist.