
Abstract
Abstract
Background:
Obesity runs in families, and family-based behavioral treatment (FBT) is associated with weight loss in overweight/obese children and their overweight/obese parents. This study was designed to estimate the costs and cost-effectiveness of FBT compared to separate group treatments of the overweight/obese parent and child (PC).
Methods:
Fifty overweight/obese 8- to 12-year-old children with overweight/obese parents were randomly assigned to 12 months of either FBT or PC treatment program. Assessment of societal costs (payer plus opportunity costs) were completed based on two assumptions: (1) programs for parent and child were available on separate days (PC-1) or (2) interventions for parent and child were available in the same location at sequential times on the same day (PC-2). Cost-effectiveness was calculated based on societal cost per unit of change using percent overBMI for children and weight for parents.
Results:
The average societal cost per family was $1,448 for FBT and $2,260 for PC-1 (p<0.001) and $2,124 for PC-2 (p<0.001). Child cost-effectiveness for FBT was $209.17/percent overBMI, compared to $1,036.50/percent overBMI for PC-1 and $973.98/percent overBMI for PC-2. Parent cost-effectiveness was $132.97/pound (lb) for FBT and $373.53/lb (PC-1) or $351.00/lb (PC-2).
Conclusions:
For families with overweight/obese children and parents, FBT presents a lower cost per unit of weight loss for parents and children than treating the parent and child separately. Given the high rates of pediatric and adult obesity, FBT may provide a unique cost-effective platform for obesity intervention that alters weight in overweight/obese parents and their overweight/obese children.
Introduction
Many pediatric obesity treatments logically focus on the child, either by intervening directly with the child, or by teaching the parent to be the agent of change for their child.1,2 Yet, obesity runs in families, and parental obesity is a risk factor for childhood obesity. 3 The shared eating and activity environment provides a unique opportunity for simultaneous treatment of obese parents and children.
Family-based treatment (FBT) is designed to simultaneously target weight control in overweight/obese parents and their overweight/obese children. FBT has a strong evidence base, 4 with research showing positive long-term outcomes for both parents and children.5–8 For example, in a recent retrospective analysis, children participating in FBT showed an average reduction in percent overBMI of approximately 20% after 6 months of treatment and 14% after 2 years. Parents showed an average weight loss of 22.9 pounds (lbs) after 6 months of treatment and 11.8 lbs after 2 years. 7
In addition to producing significant improvements in both children and parents, simultaneous FBT treatment of parent and child overweight/obesity may be more cost-effective than treating each one separately because simultaneous FBT treatment reduces time and travel costs associated with separate treatment for the parent and child and allows for coordination in familial efforts to improve processes associated with food consumption and physical activity. If the parent is changing their behaviors, then they can become a model of change for their child. Further, concurrent behavior change among family members facilitates positive reinforcement and promotes long-term behavior change. Such coordination and interplay between parent and child behavior change may facilitate weight loss outcomes that may be less likely to occur in interventions that treat the parent and child separately.
Given the prevalence of multi-generational obesity and rising healthcare costs, it is important to document the most cost-effective treatment options for overweight/obese children and their overweight/obese parents who are treated in community adult or child obesity treatment programs. The aim of this study is to estimate the costs and cost-effectiveness of FBT for treating overweight/obesity in children and their parents, compared to treating the parent and child separately (PC).
Methods
Participants and Design
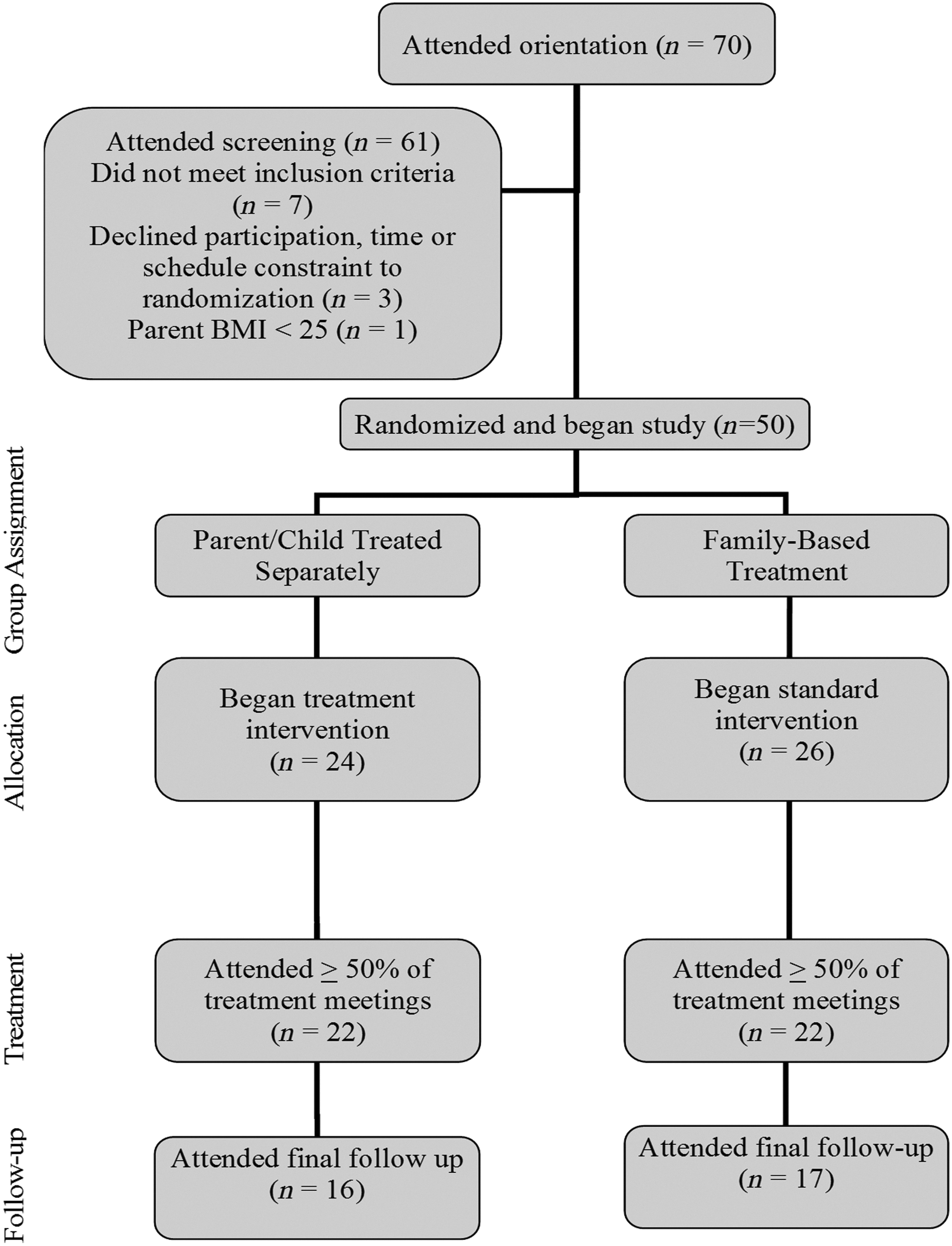
Participants were recruited in Buffalo, New York, through radio and newspaper advertisements, posters, flyers, television interviews, direct mailings, and personal and physician referrals. Eligible children were 8 to 12 years old, at or above the 85th BMI percentile, and had an overweight/obese parent (BMI of 25 or above) willing to attend a weight loss treatment. Exclusion criteria included participation of a family member in alternative weight loss programs, history of eating disorders (including anorexia nervosa, bulimia nervosa, or binge eating disorder) in either parent, child, or first-degree relative, parent or child having untreated psychiatric problems (but participants with concurrent treated disorders were accepted), dietary or exercise restrictions that would prevent participants from program adherence, and child's inability to read at a third-grade reading level. Families were screened over the phone and attended an orientation meeting, and interested persons were further screened to assess eligibility. Sixty-one families were screened to identify 54 eligible families who were randomized into FBT or PC conditions. After randomization, but preceding study initiation and collection of baseline data, three families with scheduling constraints (one in FBT and two in PC) chose to drop out of the study, leaving 51 families. One family shifted the target parent from an overweight/obese parent to a parent who was not overweight (BMI<25), making them ineligible and leaving a sample of 50 families meeting all eligibility criteria (Fig. 1). This research was approved by the Health Sciences Institutional Review Board at the University at Buffalo (Buffalo, NY). Participating parents and children signed consent and assent forms, respectively.
Structure of Treatment
Both treatment groups received an evidence-based behavioral obesity treatment program that included 15 approximately 60-minute sessions scheduled as 12 weekly sessions, two biweekly sessions, and one monthly session, with one additional session in which final treatment was delivered and follow-up collected 12 months after randomization. Each session consisted of separate large groups for parents and children, which lasted approximately 45–50 minutes, and small group counseling with three to four families with a case manager, which lasted 15–20 minutes. In FBT, families were weighed together and small group sessions were completed with the parent and child together, whereas in PC, parents and children were weighed separately and attended separate small group sessions. Details and comparisons of the two treatment programs are outlined in Table 1.
Components of Treatment in the Two Groups
PC refers to separate parent and child treatment, and FBT refers to family-based treatment in which the parent and child are treated as a family unit.
FBT included three major components: the Traffic Light Diet 9 ; a lifestyle exercise program; and a behavioral therapy component that focuses on self-monitoring, stimulus control, problem solving, and parenting. Participants were given parent or child manuals containing modules that covered program material. Topics in each module were discussed in the large group sessions, whereas small group sessions were designed to identify behaviors that influence weight change, evaluate goals, problem solve challenges, and preplan to meet goals.
The PC treatment sessions also included diet, activity, and behavior change, but no parenting component. Small and large group sessions for parents and children were completed in different locations within the medical school complex. Parents and children had large group lectures and met with a case manager in smaller groups of three to four parents to discuss behaviors that influence weight change, evaluate goals, problem solve challenges, and preplan to meet goals. The parent groups focused only on adult weight loss techniques, with no information on parenting skills for treatment of overweight children. The parent PC program is conceptualized as similar to intervention that would occur in a weight loss program for obese adults. Small and large group child PC sessions focused on changes to generate long-term weight loss. The group discussion and manuals did not focus on changes that would be coordinated between parent and child as they did in FBT. Parents of children in the PC group were provided with handouts each week on what information was covered in the child groups as well as general ideas about how to help the child, but not specific parenting information.
Diet
In both treatment programs, the Traffic Light Diet, 9 a color-coded food exchange system, was implemented to reduce high-energy-dense, low-nutrient-dense foods and increase healthier food intake, such as fruits, vegetables, and low-fat dairy. Foods were classified as red, yellow, or green based on macro- and micronutrient content. Green foods were low in fat and high in nutrient density (e.g., fruit and vegetables). Yellow foods were between 2.0 and 4.9 g of fat per serving and had moderate nutrient density (e.g., yogurt and 2% milk), 9 and red foods had more than 5 g of fat per serving or high content of simple sugars and a low nutrient density. In both treatment groups, parent and child participants were instructed to maintain a daily calorie intake between 1000 and 1500 calories, shaping a reduction in red foods to two per day, and to maintain a nutritionally balanced diet based on USDA dietary guideline recommendations. 10 When participants' weight decreased to the nonobese range, they were given the option of eating an additional 100 calories in the form of green and yellow foods, unless weight gain occurred. These participants were then encouraged to maintain a calorie intake consistent with weight maintenance.
Lifestyle exercise program
In both treatment groups, participants were educated on the benefits of increased physical activity and decreasing sedentary activities for health and weight loss.11,12 They were instructed to incorporate additional 10-minute increments of moderate-to-vigorous physical activity (MVPA) per day, increasing to 60 minutes per day of MVPA at least 5 days/week over the program. Participants were also encouraged to increase lifestyle activity, such as parking further away from stores.
Behavioral therapy
All participants were instructed to self-monitor their weight, eating, and activity behaviors and were taught preplanning and problem solving to facilitate decision making and handling of difficult eating and activity situations. There were several key differences in the behavioral therapy components of the two treatment programs. (1) In FBT, parents were trained on how to assist their children in recording weight, eating, and activity information. This training was not provided to parents in the PC program. (2) In FBT, parents were encouraged to model positive behavior changes for the entire family; however, parent modeling was not emphasized in PC. (3) In FBT, several forms of positive reinforcement were used to increase the occurrence of healthy behaviors, including praise for practicing healthy behaviors from family members. A home-based point system for parents and children was implemented to help meet targeted goals, and a monthly gift card drawing was performed to reinforce parents ($20) and children ($10) for meeting program goals. In the PC group, there were separate monthly gift card drawings for parents and children based on points earned for behavior change, but training in praise and the home-based point system were not implemented.
Measurement
Anthropometric measures
Height and weight measurements were taken at 0, 6, and 12 months by a trained staff member using a Tanita digital weight scale (Tanita, Arlington Heights, IL) and Measurement Concepts stadiometer (Measurement Concepts, North Bend, WA) calibrated daily. BMI was calculated (BMI=kg/m2), and BMI percentile was used to classify children as overweight. Percentage over BMI (overBMI) was calculated for children by comparing the participant's BMI with the BMI at the 50th BMI percentile for child age and gender. 13 BMI percentile is useful for the purpose of categorizing children into overweight and obese categories, but is less useful as a metric to evaluate treatment effectiveness. BMI percentile is not a continuous measure at the extremes because many children are above the 99th BMI percentile at baseline and may show large changes in weight, but still remain above the 99th BMI percentile, reducing the utility of the measure to determine quantitative treatment effects.
Demographics
The Hollingshead Four Factor Index 14 was used to measure socioeconomic status. The four factors were sex, marital status, educational level, and occupation. If there was more than one head of household, their individual scores were averaged.
Payer costs
Face-to-face staff time with participants was tracked by staff members based on how much time they spent in different program activities. Project coordinators checked time allocation recordings for accuracy and recorded costs of program materials. Time spent in weekly material preparation, as well as group and individual supervision of staff by the project principal investigator and project manager, was also recorded. Supervision included weekly staff meetings as well as individualized supervision based on complexity of family problems and need to maintain quality control of treatment implementation. Time spent by individual staff members was multiplied by their salaries and added across activities to generate total labor costs from the payer perspective separately for FBT and PC. The parent large groups for both FBT and PC were run by L.H.E., and the child large groups for both FBT and PC were run by C.K.K. Case managers leading the small groups had BS, MS, MSW, and PhD degrees. Indirect costs were based on the indirect cost rate for the University at Buffalo, which covers costs of room rental, heating, and air conditioning, and so on.
Participant costs
Participant costs were based on time at treatment meetings, transportation time, and fuel costs. Travel time and round-trip distance from home to the clinic were based on Google Maps calculations, and costs for fuel were estimated using 23 cents per mile driven for medical or moving purposes from the IRS standard moving rates. 15 Fuel costs per family were calculated using the following equation: mileage x $0.23×the number of sessions each family attended. Opportunity costs for treatment and transportation time were monetized using an average hourly wage rate of US adults from the Bureau of Labor Statistics of $23.31 per adult. 16 The costs for parent time were based on 90-minute sessions plus travel time. Societal costs include the sum of payer and participant costs.
Because the aim was to estimate costs for interventions to provide separate parent and child treatment or family-based treatment in primary care settings, recruitment costs, which are unique to research protocols, were not included.
Assumptions for parent and child costs
Costs to implement PC were estimated based on two different, but realistic, assumptions that characterize possible scenarios for obesity treatment delivery for a parent and child. The first assumption (PC-1) estimated costs if a parent and child attended separate group treatments on different days, doubling costs of travel and fuel, as well as opportunity costs for the parent to attend an additional treatment session. The second assumption (PC-2) assumed parent and child attended group treatments at the same location on the same night, but sessions occurred sequentially rather than concurrently (Table 2). This would be the case if a medical school or specialized obesity treatment center provided group treatment for obese children and obese adults on the same night, but at different times. We assumed there would be no time delay between delivery of the child and parent group treatments. The opportunity cost for family time is doubled for PC-2 because the parent needs to be available for the child treatment and then for their own treatment. Driving and fuel costs would not be adjusted because families would not need to make more than one trip if they were provided with sequential treatment sessions in the same facility.
Treatment and Opportunity Costs for the Two Treatments
PC-1 bases estimates for opportunity costs on the concept that the parent and child are treated on separate days, requiring the parent to drive to different treatment centers on different days, doubling travel time and time spent in treatment for waiting for child's treatment to be completed. PC-2 bases estimates for opportunity costs on the concept that the parent and child are treated sequentially on the same day. FBT bases estimates on parent and child treated as a unit on the same day, reducing travel costs and time family is in treatment.
FBT, family-based behavioral treatment.
Statistical Analysis
t-tests and chi-square tests were used to detect between-group differences at baseline. Between-group differences in payer, participant, and societal costs for FBT and PC were compared using one-way analysis of variance. Cost-effectiveness was calculated by dividing the cost by unit of percent overBMI 13 for child and weight for parent at 12 months. At 12 months, 17 families (33%) did not provide weight data. To provide the best indication of follow-up change, we imputed 12-month data based on the conservative baseline carried forward approach. Analyses were completed using SYSTAT 17 (SYSTAT Software, Inc., Richmond, CA) and SAS 18 (SAS Institute Inc., Cary, NC).
Results
Baseline characteristics of children and parents are presented in Table 3. No differences were observed in any of the child or parent characteristics. Lower costs were observed per family for FBT versus PC-1 for payer costs ($840.67±143.75 vs. $1,005.94±140.27; F(1,48)=16.88; p<0.001), participant costs ($607.41±233.97 vs. $1,254.65±338.89; F(1,48)=62.58; p<0.001), and total societal costs ($1,448.08±363.89 vs. $2,260.60±468.34; F(1,48)=47.33; p<0.001). Similarly, lower costs per family were also observed for FBT than PC-2 for payer costs ($840.67±143.75 vs. $1,005.94±140.27; F(1,48)=16.88; p<0.001), participant costs ($607.41±233.97 vs. $1,118.29±288.42; F(1,48)=47.642; p<0.001), and total societal costs ($1,448.08±363.89 vs. $2,124.24±425.29; F(1,48)=36.66; p<0.001).
Baseline Characteristics of Children and Parents in Obesity Treatment Groups
% minority refers to the percent of families who are not Caucasian.
F, female; M, male; SES, socioeconomic status; PC, parent and child; FBT, family-based behavioral treatment.
Using intent to treat, child changes in percent overBMI at 6 and 12 months for FBT were −7.4 and −6.9, respectively, whereas child changes for PC were −8.3 and −2.2, respectively. Similarly, parent changes for FBT at 6 and 12 months were −13.1 and −10.9 lbs, respectively, whereas changes in the PC group were −12.0 and −6.1 lbs. Analysis of completers showed average percent overBMI changes of −9.0 and −10.6 for FBT children, and −9.2 and −3.3 for PC children at 6 and 12 months, respectively. Parent completers demonstrated average weight changes at 6 and 12 months of −15.3 and −16.7 lbs for FBT, respectively, with average PC parent weight changes of −14.2 and −9.1 lbs at 6 and 12 months. Families in FBT attended 13.1±5.1 sessions, whereas families in PC attended 14.0±3.6 sessions (F(1,48)=0.55; p=0.46).
Child cost-effectiveness ratios were $209.17/percent overBMI lost for FBT and $1,036.50/percent overBMI and $973.98/percent overBMI for children in PC using PC-1 and PC-2, respectively. Parent cost-effectiveness ratios were $132.97/lb lost for FBT and $373.53/lb and $351.00/lb lost for PC-1 and PC-2, respectively.
Discussion
Based on PC-1 assumptions, treating parent and 8- to 12-year-old child separately was 4.96 times more expensive per unit of weight loss for children and 2.81 times more expensive for parents than FBT over 12 months. Whereas there are large differences in cost-effectiveness under both assumptions, differences between PC-1 and FBT are greater because the parent must travel twice, once for their own treatment and once for the child's treatment, and the parent must spend twice as much time away from other activities by attending separate treatment sessions for the parent and child. Because PC was relatively less efficacious for both children and parents, and costs more to deliver than FBT, PC is considered a dominated strategy and FBT should be considered for implementation.
PC costs were based on having the parent and child treated using a similar structure to that used in FBT, with a large group meeting with all group members plus smaller group meetings to review weekly performance, discuss problems, and maximize adherence. The treatment costs are impacted by the treatment structure used. Treatment would be less expensive if there were fewer visits, and some research suggests that shorter programs can be effective, 8 though other research has shown that the greater the number of treatment sessions, the better the long-term outcome.4,19 In addition, state-of-the-art adult treatment includes extensive use of treatment meetings with maintenance of contact with a case manager over time,20,21 suggesting that briefer, less-intensive treatments would save money, but at the cost of reducing treatment effectiveness.
Strengths of the study include the randomized design, use of a well-validated treatment protocol, and the ability to capture costs from multiple perspectives. 9 Despite these strengths, there are limitations to the study that may limit generalizability. The study was implemented in families with overweight/obese 8- to 12-year-old children, and the results may be different when treating older adolescents, who may require less parental intervention than younger children. Costs of treatment delivery were based on the actual costs of treatment, but did not consider costs of training. 22 PC and FBT require staff with specialized training for program implementation, as well as supervisors expert in implementing these treatments. In many communities, it may be challenging to identify and train staff qualified to implement FBT. An additional limitation is that participant costs are limited to costs associated with attending the meetings. Additional costs, such as the time to do physical activity, cook family meals, or the expense of buying exercise clothes, team memberships for children, or gym memberships for parents, for example, were not considered. Additionally, changes in the types and amounts of food purchased and prepared may require more time spent shopping and cooking and affect money spent on fresh foods; however, in a previous investigation of the cost of FBT, we did not show greater food costs for families after participation in FBT. 23 There may also be considerable savings if a family is shopping and preparing the same healthier foods for parents and children, rather than having different diets and thus buying “special” foods for a parent or child who is trying to change their eating habits. In addition, we did not consider costs of child care, which could be needed for parents while attending the meetings without their children. The study was implemented in a medical school setting in which the parent and child treatments were implemented in the same complex of buildings. In many environments, treatment for adults and children would be in different geographic locations, which could affect travel costs. Last, we attempted to model treatments that would currently be implemented for obese adults or obese children, which would typically be in different settings. We did not use the model of concurrent, but separate, treatment of parents and children that might be possible in obesity specialty clinics, but would not be common in community settings that primarily treat obese adults or children.
We did not collect medical costs saved by FBT or PC treatment. These costs would not be expected to be very great over just 1 year and may not be apparent for children who are obese, but otherwise healthy. Even very successful programs with documented treatment efficacy in preventing diabetes require a substantial follow-up period to document differences in costs. 24 There is little research on cost-effectiveness of obesity treatment in children for purposes of comparison to this study of FBT. It may be hard to estimate the influence of weight loss on long-term morbidity; thus, we did not attempt to extend the weight loss results to cost per quality-adjusted life-years saved.
The study was designed as an effectiveness trial to facilitate generalization of treatment effects to the broader population. For example, there were no upper limits for weight, families were accepted with concurrent treated psychiatric disorders, and over 25% of families were minority, which is greater than the percentage in the local population. These factors may explain, in part, the attrition rate of 33%, which is greater than we have observed in previous FBT trials. 7
The parent treatment used in the PC group was based on the parental treatments used in FBT and may be different than an intervention that is specifically implemented for adults. The treatments for the parent and child were implemented during the same time periods, but it is possible that many parents would not choose treatment for themselves and their child during the same time period, but may prefer different time periods for treatment. This would not change the costs of treatment implementation, but it could change treatment efficacy, because it may be easier for a parent to focus on one family member at a time, rather than try and change their own behavior and their children's behavior simultaneously.
FBT targeted one overweight/obese child and one overweight/obese parent. Given that obesity runs in families,3,25,26 there may be other overweight/obese family members who could benefit from treatment. FBT may have effects on other family members 27 because treatment of obese adults has shown generalization of treatment effects to the spouse. 28 In addition, treating an obese parent and child may help prevent obesity in an at-risk sibling, 29 which may amplify the effects of treatment beyond those who are directly targeted. Because FBT is designed to target the shared family environment, provide models for other family members, and modify interactions between family members, it is possible that FBT would be associated with more-generalized effects across family members than usual treatment, thus extending effects and further improving cost-effectiveness. This hypothesis should be tested in future studies.
The cost calculations are based on group treatment for the child and parent. Providing individualized treatment for the child and/or parent would influence cost-effectiveness, because it is much more costly to provide individual than group treatment. Thus, even the least cost-effective group treatment may prove to be more cost-effective than the most cost-effective individual treatment. The obvious advantage of individualized treatments is that they facilitate scheduling, whereas scheduling multiple families or people for the same time in a group is more challenging.
Conclusions
This study provides a new template for evaluation of family-based treatment and provides encouraging data for treatment of families where there is multi-generational obesity. Given the high rates of obesity in adults and children,30,31 FBT may provide a unique, cost-effective platform for obesity intervention that alters weight in obese parents and their overweight children.
Footnotes
Acknowledgments
This research was funded, in part, by funds from the Healthy Living Foundation. The funding agency was not involved in analysis or interpretation of the data. Appreciation is expressed to Alison Yee, who provided feedback on a previous version of the manuscript.
Author Disclosure Statement
No competing financial interests exist.