
Abstract
Abstract
Background:
The Healthy Obsession Model posits that committed weight controllers develop preoccupations with the planning and execution of target behaviors to reach healthy goals. We expected that successful weight controllers, more so than unsuccessful weight controllers, would report more elaborate definitions of their healthy obsessions, negative reactions to lapses, and constructive responses to high-risk situations. We also expected to find differential sources of commitment between losers and gainers, including a greater emphasis on emotional and experiential consequences by losers, as documented in the authors' 2012 study.
Methods:
Sixteen adolescent participants who had completed cognitive-behavior therapy immersion treatment for obesity at least 1 year before the interviews (8 successful and 8 unsuccessful weight controllers) completed in-depth interviews based on the Scanlan Collaborative Interview Method. A qualitative analysis followed in which two coders identified themes within the interviews.
Results:
Reliable coding of the interviews produced results that supported the hypothesis that highly successful weight controllers nurture strong healthy obsessions. Successful weight controllers also reported using significantly more helpful motivators than did unsuccessful weight controllers. In addition, these adolescent weight controllers seemed motivated by some of the same factors that elite athletes identified in the Sport Commitment Model.
Conclusions:
Clinical implications include focusing weight loss interventions on nurturing healthy obsessions in general and, more specifically, on helping weight controllers use more diverse sources of commitment.
Introduction
Over the past three decades, prevalence rates of obesity have doubled or tripled in some countries on all six of the world's populated continents, with highest incidence rates observed in the richest countries, such as the United States. 1 Almost 40% of America's children and teenagers are now either overweight or obese, and epidemiological analyses suggest that this alarming rate will continue to grow in the foreseeable future.2,3 These overweight and obese young people will develop, later in life, major and expensive health problems at far greater rates than their leaner, more fit peers, including type 2 diabetes, cardiovascular problems, many forms of cancer, and other health conditions. 4 Childhood obesity can also negatively and substantially affect quality of life, academic achievement, social and vocational opportunities, and emotional well-being. 5
Fortunately, for those suffering from obesity, treatment can improve health, physical fitness, mood, and psychosocial functioning.6–8 Education, outpatient cognitive-behavior therapy (CBT), bariatric surgery, and immersion are the four primary interventions currently used to treat childhood and adolescent obesity. Immersion treatment is defined as an intervention that places participants into a therapeutic and educational environment for an extended period of time, thereby removing them from obesogenic environments. 9 In a recent review, Kelly and Kirschenbaum concluded that educational interventions rarely produce significant improvements and that outpatient CBT produced significant, but variable, degrees of success; however, immersion programs that included CBT seemed to produce greater reductions in percent overweight at post-treatment and follow-up, with much less attrition, than outpatient CBT. 9
The Healthy Obsession Model
Kirschenbaum recently proposed the Immersion-to-Lifestyle Change model to help explain the promising effects of CBT immersion treatment. 10 The model asserts that the rapid weight loss typical of immersion treatment, when combined with CBT, helps participants attribute success to their own improvements in self-regulatory skills, behaviors, and knowledge. According to the model, this increase in self-efficacy, in conjunction with a healthy obsession and social support, maximizes lifestyle change after immersion treatment.
Kirschenbaum and colleagues defined a healthy obsession as “a sustained preoccupation with the planning and execution of target behaviors to reach a healthy goal” (p. 169).1,11,12 A variety of studies have demonstrated support for various aspects of the Healthy Obsession Model (HOM). For example, the model suggests that weight controllers' success depends on establishing and maintaining strong commitments to target behaviors, such as consistent self-monitoring and planning. Correlational and experimental evidence supports the vital role of consistent self-monitoring and planning for successful weight control. For example, two experiments found that interventions that increased self-monitoring improved weight loss among active weight controllers in CBT programs.13,14 A recent study of successful weight controllers showed that they exerted far more effort in planning and focusing on their eating and activity patterns (analogous to exhibiting healthy obsessions) during the high-risk holiday season than did nonweight controllers; those masters of weight control that managed to avoid gaining weight reported self-monitoring more consistently than those that gained weight during the holidays. 15 Even a study of neural activity suggests that highly successful weight controllers differentially activate areas of the brain (e.g., dorsal prefrontal cortex) after eating, suggesting higher levels of concern and planning after eating compared to nonweight controllers. 16
Direct Tests of the Healthy Obsession Model
A recent study by Byrne and Kirschenbaum 17 tested the HOM directly. The study included 55 adolescents who participated in a CBT immersion program. The researchers suddenly removed access to self-monitoring journals after several successful weeks at the camp. Virtually all of the campers had self-monitored very consistently during these successful weeks at the camp. The HOM would predict a negative reaction to this removal of self-monitoring. As expected, journal/monitoring removal resulted in decreased positive affect for the campers, as measured by changes in ratings by staff members. Also as expected, campers who demonstrated heightened commitment to the program, based on higher levels of activity and more journaling, reacted especially negatively to the withdrawal of the opportunity to self-monitor.
A very recent study served as the primary impetus for the current research. 18 In that study, we investigated obese adolescents' healthy obsessions and how they seemed to impact long-term success at weight control. The study examined a variety of factors by qualitative analysis to compare highly successful adolescent weight controllers (“losers”) to unsuccessful weight controllers (“gainers”) 1 year after completion of a CBT immersion treatment program (Wellspring Camps). We found that successful weight controllers evidenced more fully developed healthy obsessions, including more overtly negative reactions to barriers to execution of their plans. They also reacted more negatively to lapses from their usual weight-controlling behaviors and to concomitant weight regain.
That study also examined the sources of commitment mentioned by losers and gainers. In accord with the HOM, losers and gainers identified sources of commitment consistent with the sources of commitment identified by other groups of individuals demonstrating high levels of commitment or healthy obsessions with other behaviors (e.g., elite athletes). More specifically, the Sport Commitment Model (SCM) distinguishes between six sources of commitment used by elite athletes: emotional and experiential consequences; social support of parents, friends, and peers; institutional influences; and valuable opportunities. 19 The parallels in healthy obsessions between weight controllers and elite athletes suggested the possibility of using the sources identified in the SCM to examine differential use of those sources by weight controllers. Some interesting findings emerged when applying the SCM in this way to the study of success in long-term weight control. Losers in our previous qualitative study 18 reported that they relied on a slightly wider variety of those sources of commitment than gainers. Most notably, losers reported relying on emotional consequences and experiential consequences for motivation more than gainers.
The Present Study
The 2012 qualitative evaluation of the HOM by our group clearly supported the viability of the model, but it had some limitations. 18 It included only 4 losers and gainers, thereby limiting potential generalizability. The relative novelty of the findings showing strength of healthy obsession as potentially vital for success also merits replication. Therefore, we extended and attempted to replicate the 2012 study by doubling the sample size of each group. We again examined a variety of factors by qualitative analysis to compare highly successful young weight controllers to unsuccessful weight controllers 1 year after completion of CBT immersion treatment (Wellspring Camps). Based on the HOM, we also expected to find differential evidence in successful weight controllers of more fully developed healthy obsessions, including more overtly negative reactions to barriers to execution of their plans, lapses from their usual weight-controlling behaviors, and associated weight regain. We also anticipated, based on the 2012 qualitative study, to find differential sources of commitment between losers and gainers, including a greater emphasis on emotional and experiential consequences by losers, as documented in the 2012 study. The novelty and potentially substantial clinical implications of this finding from the 2012 study made this latter hypothesis particularly important. Therefore, it seemed worthwhile to compare directly findings of the 2012 study to the present study regarding differential sources of commitment between losers and gainers.
Methods
Participants
Participants attended immersion CBT camps in Texas (Wellspring Texas; WTX) or New York (Wellspring New York; WNY) for at least 4 weeks in the summer of 2010. We conducted a 1-year follow-up in which parents and participants provided height and weight data. Of 232 campers, repeated e-mails, phone calls, and a $25 incentive yielded data on 157 of 232 (68%). Table 1 shows precamp, postcamp, and follow-up data on this initial group of campers.
Original 157 Participant Data: Initial to 1-Year Follow-Up
SDs, standard deviations.
We will first describe the final group of 16 participants (8 losers and 8 gainers) and then describe in more detail how they were selected (i.e., the procedures followed in Fig. 1). Of the 8 losers, 7 were female, 4 were Caucasian, 3 were African American, and 1 was categorized as “other”; ethnicity; 3 attended WNY and 5 attended WTX; average age was 16.5 years (standard deviation [SD], 4.3); average initial BMI was 36.81 (SD, 7.04); average initial percent overweight was 84.36 (SD, 37.85); and average length of the program was 5.25 weeks (SD, 1.49). The 8 gainers were all female; 6 were Caucasian; 2 were African American; 4 attended WNY, 4 attended WTX, average age was 14.0 years (SD, 2.6); average initial BMI was 37.33 (SD, 7.25); average initial percent overweight was 95.52 (SD, 40.24); and average length of the program was 5.50 weeks (SD, 1.41). Despite substantial incentives and numerous efforts to recruit participants who resembled one another closely in age, it became necessary to expand the age range from adolescents to include young adults to obtain adequate data for this replication/extension. Table 2 presents the initial, post-treatment, and follow-up data for both loser and gainer groups (N=16). Figure 2 shows the percent overweight of both losers and gainers from initial assessment through follow-up.

Participant recruitment flowchart.
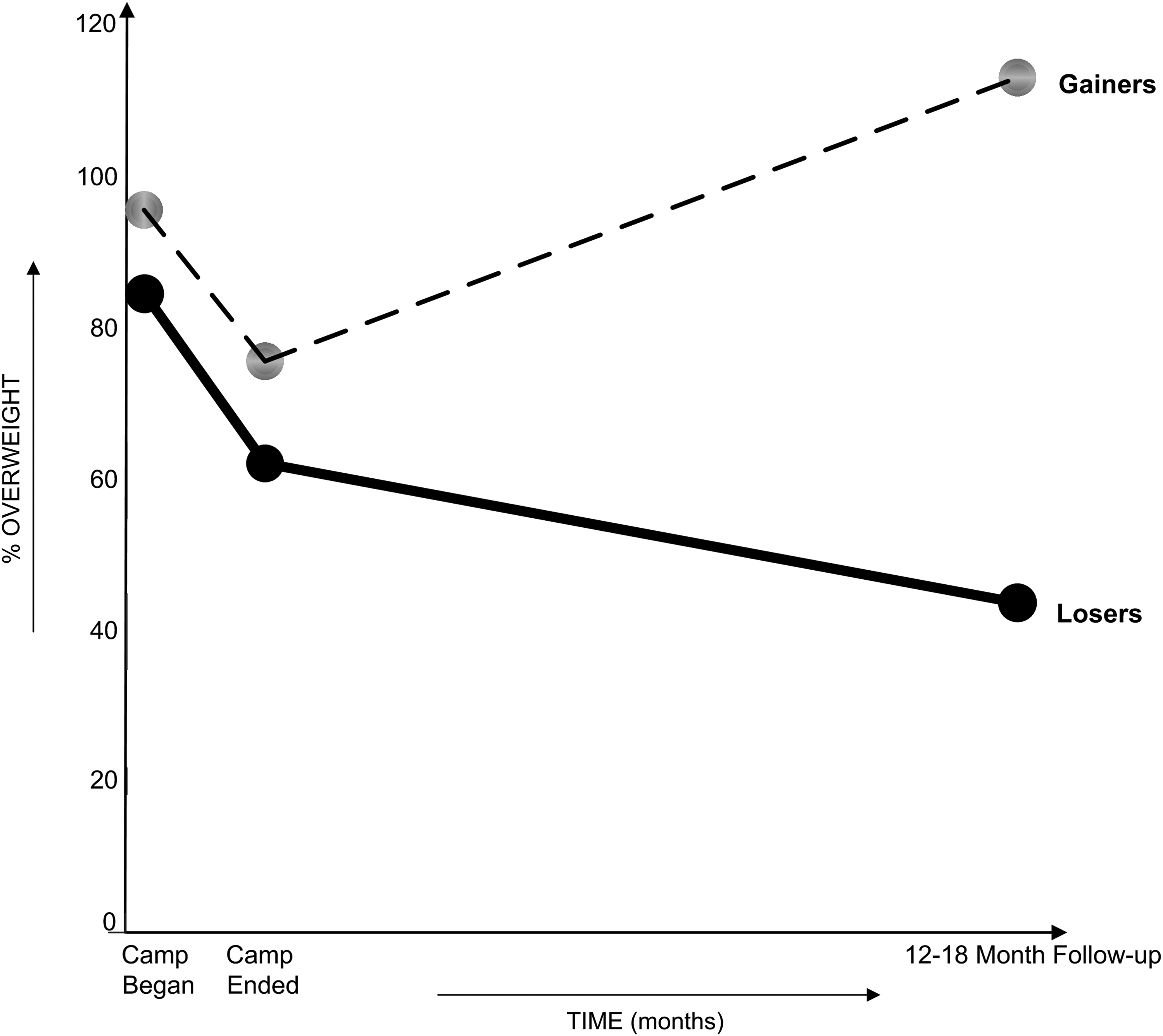
Initial, postcamp, and follow-up percent overweight: losers versus gainers.
Loser/Gainer Data: Initial to 1-Year Follow-Up
L1=% overweight decreased most from postcamp to follow-up; L8=% overweight decreased least; G1=% overweight increased the most postcamp to follow-up; G8=% overweight increased the least postcamp to follow-up.
SDs, standard deviations.
The procedures associated with Figure 1 used to select the final participants began with defining maintenance of weight, using percent overweight as a standard measure for all campers. Percent overweight was defined by the following formula: percent overweight=([BMI/50th percentile BMI] – 1)×100. 9 Normative (50th percentile) BMIs were determined using data generated by the CDC based on age, gender, and height. 20
To determine follow-up status (loser, gainer, or maintainer), we began with a standard definition in the literature for “maintenance”: ±3% of actual weight over time. 21 This definition of maintenance functions well for adults whose heights are stable and for whom norms provide a convenient definition of acceptable weight (e.g., BMI≤25). For growing children, however, heights change over time as do ideal weights based on age and gender. So, we approximated the adult definition of maintenance by first establishing BMI cutoffs that mirrored the adult definition of ±3%. This necessitated adding 3% of weight to the post-treatment weight and then subtracting 3% from that post-treatment weight. These values were then translated to BMIs for each camper. The higher value (+3% of post-treatment weight BMI) therefore became the upper cutoff; conversely, the lower BMI (−3% of post-treatment weight) became the lower cutoff. Campers whose follow-up BMIs fell below the lower BMI cutoffs were then classified as losers; similarly, gainers were campers whose BMIs at follow-up exceeded the upper BMI maintenance cutoff; maintainers had BMIs at follow-up between their own upper and lower BMI cutoffs.
This sample of 157 was then categorized into subgroups of 39 losers, 71 gainers, and 47 maintainers. Once labeled as a loser or gainer, the potential participants were ranked on the amount of difference in percent overweight from the end of camp to the follow-up percent overweight. These rankings served to illustrate the “top” or most extreme losers and gainers. In other words, the rankings identified those who had the biggest decreases in percent overweight from the end of camp to 1 year follow-up and the biggest increases in percent overweight from the end of camp to 1 year follow-up. Finally, we matched losers to gainers based on initial percent overweight, attempting to include losers and gainers whose initial percent overweight matched within 3%. After matching the participants, 32 losers were reasonably well matched, based on initial percent overweight, to 51 gainers. Those 83 individuals were the targets for inclusion in this study. Of the targeted 83 losers and gainers, repeated e-mails, phone calls, and up to a $200 incentive yielded interview data and verified heights and weights by healthcare providers on 16 final participants.
Procedures
Wellspring Camp immersion program
The Wellspring program, based on the HOM, uses a 3-1-8 approach outlined in the The Wellspring Weight Loss Plan. 22 The “3” represents three primary goals: to eat zero fat grams (accepting <20 g per day); to move at least the equivalent of 10,000 steps daily measured on a pedometer; and to self-monitor 100% of food and activity. The “1” represents the overarching mission—to develop a healthy obsession. Finally, the “8” identifies eight steps recommended to help understand the rationale for the three primary goals and develop robust healthy obsessions: step 1, make the decision; step 2, know the enemy—your biology; step 3, eat to lose; step 4, find lovable foods that love you back; step 5, move to lose; step 6, self-monitor and plan consistently; step 7, understand and manage stress; and step 8, use slump busters to overcome slumps.
In Wellspring's camps in 2010, all participants experienced: a CBT immersion approach, including four weekly CBT sessions (two individual, two group) conducted by advanced graduated students, as well as master's- and doctoral-level therapists; nutrition and culinary education; family involvement through workshops during camp; and an Internet-based interactive continuing care self-monitoring system for 10 months postcamp. Evaluations of Wellspring's programs have demonstrated substantial promise, including large and sustained changes in weight status for many participants.6,10,23,24
Participant recruitment and administration
One year after completion of WNY's and WTX's 2010 camp session (i.e., beginning in fall 2011), the first author and one research assistant contacted all campers and parents by e-mail and telephone to obtain reports of follow-up height and weight. As mentioned previously and shown in Figure 2, the authors used change in percent overweight from post-treatment to follow-up to identify the 32 campers who lost the most additional weight and 51 who regained most (top losers and gainers, respectively). Both losers and gainers were asked to provide verification of reported height and weight by any healthcare provider (e.g., doctor, school nurse, or pharmacist) and were also asked to complete a telephone interview about their weight loss experiences during the follow-up period. Participants received between $25 and $200 for providing verified height and weight and for completing the requested interviews. On average, researchers contacted losers 1.3 times by e-mail and phone to obtain verified weights and heights. In sharp contrast, researchers had to pursue gainers much more vigorously to obtain this critical data, requiring, on average, 12.13 contacts—almost 10 times more effort to obtain the data.
All parents and campers over age 18 signed consent forms that provided permission for Wellspring researchers to include their children's or their data at camp and at follow-up in evaluation studies. In addition, this study was approved by an institutional review board from the Illinois School of Professional Psychology at Argosy University (Chicago, IL).
Before beginning the interviews, researchers e-mailed to all participants' consent, assent, and introduction forms explaining details of the study and confidentiality. Interviews lasted between 17 and 74 minutes (losers: mean [M], 40.54; SD, 16.16; gainers: M, 29.11; SD, 9.06; all participants: M, 34.82; SD, 13.97) and were recorded and transcribed from digital audio copies.
Measures
Weight change
Weight change was defined as change in percent overweight, using the formula cited previously and CDC norms to determine 50th percentile BMIs (percent overweight=([BMI/50th percentile BMI] – 1)×100).9,20 Many studies of the treatment of childhood obesity focus on this statistic.6,9 The simplicity of the concept of percent overweight makes it more readily understood than the other frequently used alternative, BMI z-score: BMI z-score=Reported BMI – 50%ile BMI/SD of the Normative Group BMI. These two statistics, percent overweight and BMI z-score, both rely on normative data (e.g., CDC norms) and are therefore sensitive to changes in BMI associated with growth, age, and gender. These two statistics also are highly intercorrelated and essentially provide similar information about relative weight status. For example, in the present sample of 16 participants, the initial BMI z-scores correlated very significantly with the initial percent overweight values (r=0.967; p<0.00001).
Clinical staff obtained initial and postcamp height and weight using high-quality calibrated digital scales and standard stadiometers. Verified follow-up height and weight were provided by healthcare professionals in campers' home communities.
Wellspring Transformative Change Interview
As shown in Table 3, the Wellspring Transformative Change Interview (WTCI) is a 53-item mixed qualitative (n=19 questions) and quantitative (n=34 questions) structured interview based on the Scanlan Collaborative Interview Method (SCIM).19,25 The SCIM has been used previously in multiple studies and obtained 100% consensus validation of each of its themes and constructs. The WTCI was also validated by Gierut and colleagues, 18 demonstrating a high degree of convergence in their numerical ratings (rater A vs. B: r=0.87, p<0.0001; rater A vs. C: r=0.91, p<0.0001; rater B vs. C: r=0.97, p<0.0001) and categorical ratings (average: r=0.64; p<0.008). Specifically, the WTCI contains items measuring participants' commitment and responses to eight hypothetical situations. The responses to those eight hypothetical situations (items 24–50) included seven open-ended or qualitative questions and 19 questions requiring a numerical response or quantitative questions. This measure includes verbiage to enable campers to describe their sources of commitment. More specifically, the WTCI states,
Wellspring Transformative Change Interview
In discussing your sources of commitment, please keep two important things in mind. 1. First, please feel free to draw on any aspect of your Wellspring experience in identifying the causes of your commitment—you do not need to limit yourself only to camp. Your sources of commitment could come from things or people. For example, your sources could come from your experiences at Wellspring, relationships and interactions with people at Wellspring OR outside/before/after your Wellspring experience—such as your family, friends, teammates, coach, the public—or from any other important part of your experience. So when you are thinking about what your sources of commitment are—think big and broad. Are you clear on this? 2. The second point to keep in mind as we discuss the sources of your commitment is that there are two general types of sources that can operate at any given time—those that strengthen your commitment, and those that weaken your commitment (chip away at it). So in discussing the causes of your commitment, please consider both kinds. Are you clear on this?
WTCIs were analyzed using an open coding system to identify themes of commitment.19,25 The SCM previously identified themes of sustained sport commitment in elite athletes, 19 and we hypothesized that themes in this study would fall along similar lines. Therefore, questions in the WTCI inquired about emotional and experiential consequences, support, and valuable opportunities. Additional open-ended questions in the WTCI pertaining directly to the HOM require participants to rate their degrees of distress (subjective units of distress [SUDS], ranging from 0=no impact to 100=extreme distress) on various aspects of the HOM (i.e., eating more than 20 g of fat in a particular day).
Evidence of healthy obsessions in responses to hypothetical situations
Participants responded to a series of hypothetical questions about healthy obsession behaviors in various situations, such as planning ahead in high-risk situations. We devised these questions to provide clear indicators of the degree to which respondents developed functional healthy obsessions, in accord with previously published definitions of this construct.9,19 In order to examine the degree to which the expected answers conformed to the healthy obsession construct, we asked two groups of raters (Wellspring Academies' clinical teams: North Carolina and California) to evaluate the campers' responses. This provided an independent check on their validity as measures of healthy obsessions.
More specifically, we asked these two groups of raters, both of whom had documented expertise on the construct of healthy obsessions, to rate responses for degrees of healthy obsessions. Each group of raters read the responses to three of the questions that seemed to differentiate the actual participants and rated participants' levels of healthy obsession from 1=not healthfully obsessed to 5=extremely healthfully obsessed. We also asked the raters to guess whether participants were losers or gainers based on deidentified responses to the same three healthy obsessions questions.
Raters' responses correlated highly both with one another and with the authors' ratings (authors vs. raters A: r=0.81, p<0.01; authors vs. B: r=0.68, p<0.01; raters A vs. B: r=0.79, p<0.01). The two external groups of raters correctly identified the loser/gainer status of 72% of the participants (z=1.85; p=0.03). Therefore, these external ratings helped establish the validity of the questions as measures of the construct of healthy obsession.
Two psychology graduate students (including the first author) coded the interviews independently and blinded to loser/gainer status in the case of the second coder. Coders demonstrated a high degree of inter-rater reliability in their numerical ratings (rater A vs. B: r=0.99; p<0.01) and qualitative ratings (rater A vs. B: r=0.88; p<0.01).
Results
In accord with hypotheses, the common themes expressed by all 16 participants mirrored, to a substantial degree, the sources of commitment reported by elite athletes identified in the SCM, as well as campers in our 2012 qualitative study. 18 Specifically, as noted in the 2012 study, the young weight controllers in this study identified six primary sources of commitment: social support-friends/peers (SSF); social support-parents (SSP); valuable opportunities (VO); emotional consequences (EmC); experiential consequences (ExC); and institutional influences (II). After defining these sources of commitment based on the responses of all 16 participants, we will compare losers to gainers regarding their sources of commitment and healthy obsessions.
Sources of Commitment
Social support
Participants described two types of social support (parental and peer/friend support) and viewed these sources as helping or hindering their efforts to maintain healthy lifestyles. For example, some campers identified one of their parents as both providing verbal encouragement (helpful), but still eating high-fat foods in front of them occasionally (hindering).
Valuable opportunities
Participants mentioned that they obtained valuable opportunities because of their efforts at lifestyle change. Such opportunities included better quality of health and a sense of accomplishment and self-efficacy.
Emotional consequences
Participants discussed the emotional consequences of losing weight as positive and negative motivators, including avoidance of depressive feelings associated with obesity (a positive or helpful motivator) and becoming angry and wanting to rebel against bullying by remaining overweight (a negative motivator).
Experiential consequences
Participants mentioned various situations that served to motivate them or impact their motivation adversely. These included frustrations that motivated them positively, such as frustrations with their restricted physical abilities (tiring easily or running slowly in sport competitions). Experience with the extra time required to focus on weight control and exercising detracted from their commitment to maintain effective weight control.
Institutional influences
Participants discussed the influences of institutions as adversely affecting their motivation when schools or restaurants, for example, had many high-fat foods and few very-low-fat choices.
Losers versus Gainers
Losers and gainers differed in their reported commitments to healthy living, healthy obsessions, and adherence to weight-controlling behaviors.
Weight-controlling behaviors
As shown in Figure 3, losers reported much greater consistency with targeted behaviors, including weighing themselves almost every day (87.5% losers, 37.5% gainers; φ=–0.52, large effect), self-monitoring their weights and eating/activities more frequently (50% of days losers, 12.5% gainers; φ=–0.40, medium-to-large effect), and maintaining a very-low-fat diet (M days losers: 5.19; SD, 1.51; M days gainers: 2.94; SD, 2.56; d=1.07, large effect). However, gainers reported slightly greater consistency with the targeted behavior of high levels of activity (10,000 steps per day: 62.5% losers, 75% gainers; φ=0.13, small effect).
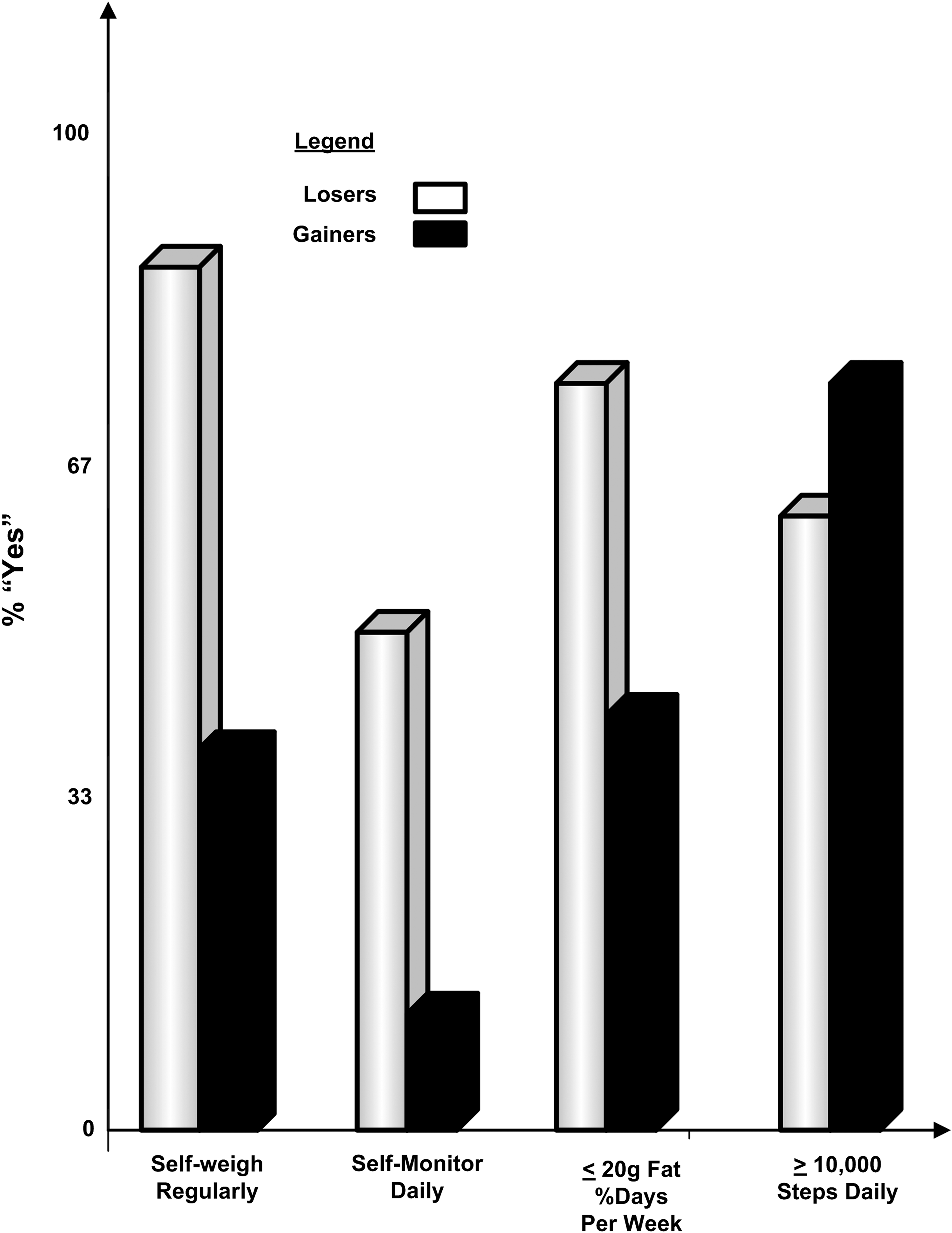
Weight controlling behaviors: losers versus gainers.
The losers and gainers did not demonstrate substantial differences regarding a hypothetical question about distress after weighing oneself and gaining weight. Losers and gainers reported similarly high levels of distress in response to this question (5 of 8 [62.5%] losers' SUDS ratings above 50; 4 of 8 [50%] gainers' above 50; φ=–0.13, small effect).
Evidence of healthy obsessions in responses to the hypothetical situations
Losers' responses to 10 (three qualitative and seven quantitative) of the 27 questions about the eight hypothetical situations described in the WTCI (quantitative questions 29, 34–36, 39, and 42–43; qualitative questions 26, 37, and 41) demonstrated reactions much more in accord with the HOM than did gainers. In the remaining 17 questions about the hypothetical situations, losers' and gainers' responses showed similar patterns, with neither group showing greater or lesser degrees of healthy obsessions. The losers seemed to respond differentially, particularly to situations (exams and fights with friends) in which they reported themselves likely to use increasing their activity levels to cope with stressors.
Quantitative differentiators
29. You're on vacation with your family for 10 days. On how many of those days would you eat 20 grams of fat or less? Losers reported that they would eat less than 20 g of fat per day on 56% more days on that vacation than gainers (M, 6.38 [SD, 1.69] vs. 4.06 days [SD, 2.82]; d=1.00, large effect).
34–36. You have three major exams coming up in school this week. You have to meet with groups, cram/study very hard, and you feel very stressed about getting everything done and doing well. Of the 7 days leading up to the exam, how many days would you monitor food? How many days would you get 10K steps? How many days would you eat 20 grams of fat or less? Losers reported that they would continue to self-monitor an average of 5.25 days (SD, 2.43) leading up to the exam versus 3.94 (SD, 2.98) days by gainers (d=0.48, medium effect). Losers indicated that they would exercise, on average, 4.94 (SD, 2.15) days leading up to the exam, compared to 3.38 (SD, 2.37) days by the gainers (d=0.68, medium to large effect). Losers also reported that they would eat less than 20 g of fat per day on an average of 5.88 (SD, 1.25) days leading up to the exam versus 4.69 (SD, 2.79) days by gainers (d=0.55, medium effect).
39. You get into a fight with your best friend (boyfriend/girlfriend), and he/she does not speak to you for the rest of the day. Will you still eat less than 20 grams of fat on this day? All losers (8 of 8; 100%) reported that they would still eat less than 20 g of fat on this day, whereas only half of the gainers (4 of 8; 50%) reported that they would still eat less than 20 g of fat on this day (φ=–0.58, large effect).
42–43. You are heading to your friend's house for a party. You know that the food there will primarily consist of high-fat pizza and chips. Will you still reach your 10K step goal today? Will you still eat less than 20 grams of fat this day? All losers (8 of 8; 100%) indicated that they would still reach their step goal versus 5 of 8 of the gainers (62.5%; φ=–0.48, large effect). Similarly, all losers (8 of 8; 100%) reported that they would still eat less than 20 g of fat on this day, whereas only 5 of 8 of the gainers (62.5%) reported that they would eat within that key guideline of the Wellspring Plan (φ=–0.48, large effect).
Qualitative differentiators
26. Let's imagine that you normally get in 10,000 steps every day by walking, but today your ankle really hurts; you injured it playing soccer yesterday, and it is uncomfortable to walk. Will this impact the food you eat this day? Only losers demonstrated attitudes consistent with a healthy obsession by noting that they would decrease their eating because they expected the injury to prevent them from reaching their activity goals. In sharp contrast, two of the gainers noted that they expected to overeat in response to the injury, not decrease their eating.
For example, one Loser stated, “Yes it would [impact the food I eat]. You have to change your diet since you'll do less exercise. You still need to lose weight that day.” Another loser mentioned, “I would make sure I'm being very careful of what I'm eating because I cannot meet my step goal.” In contrast, a gainer, stated, “Probably [impact the food I eat], more in a negative way. I would probably feel sorry for myself. I would be less likely to get up and cook things because my ankle would hurt and go out and get healthy things is unlikely if I'm injured.” Another gainer stated, “Um, I do find myself getting bored in situations like this and then I'd just eat more.”
37. You get into a fight with your best friend (boyfriend/girlfriend), and he/she does not speak to you for the rest of the day. How does this impact your activity for the day? Losers again demonstrated more substantial healthy obsessions than gainers. Losers reported that the fight with their friend would not impact their weight control programs, whereas gainers expected negative outcomes. For example, one loser stated, “I'll suck it up and do what I need to do. It wouldn't affect me.” Similarly, another loser reported, “It [fight with friend] doesn't impact my activity; well, to me that's a nonrelated event. You must exercise and you cannot let things hinder you.” In contrast, a gainer stated, “Um, I'd sit there eating frozen yogurt and watch TV and cry. It affects me very much when I get into an argument.” Another gainer mentioned, “Lower it [my activity] dramatically.”
41. You are heading to your friend's house for a party. You know that the food there will primarily consist of high-fat pizza and chips. Do you have a plan for eating at the party? Losers used more-definitive language about their plans, whereas gainers used language such as “probably” and “I guess,” illustrating less confidence in their responses. For example, one loser stated, “Yes [I have a plan]. I'll bring a lean cuisine. I don't care what people say.” Another loser stated, “Yes, I would eat before. It's a little trick that I do, because if you are already full you are not going to eat anything else. And just be like ‘oh, no I am not hungry thank you.’ I would definitely eat before and make sure that it was fulfilling food so that I am satisfied.” In contrast, a gainer predicted, “Probably eat one plate and a few chips and go hang out.”
Sources of commitment
We compared losers to gainers on the degree to which they relied on the six sources of commitment identified in the SCM: social support-friends/peers; social support-parents; emotional consequences; experiential consequences; institutional influences; and valuable opportunities. Losers reported that their parents provided more support than gainers (8 of 8 [100%] losers vs. 5 of 8 [62.5%] gainers; φ=–0.48, large effect), but that difference seems less noteworthy than the degree to which losers found a wider array of sources as helpful to their efforts.
Losers and gainers could have identified a maximum of six sources of commitment as either helpful or nonhelpful (SSF, SSP, EmC, ExC; II, and VO). On average, losers considered 3.5 (SD, 1.07) of the 6 sources as helpful, whereas gainers only considered an average of 2.1 (SD, 1.13) to be helpful (d=1.27, large effect). Thus, the losers' identified 66.7% more of the six possible sources as helpful (58.3%) than gainers (35.4%).
The 2012 investigation elicited similar results. In that study, on average, losers considered 3.25 (SD, 1.71) of 6 sources as helpful versus gainers viewing only 2.0 (SD, 0.82) to be helpful, although, in this case, the difference between proportions for losers and gainers failed to reach statistical significance (d=0.93, large effect).
We also compared losers to gainers by combining both the 2012 study and the current study. We calculated that losers and gainers each had a maximum possibility of endorsing 72 sources of commitment as either helpful or nonhelpful (48 sources+24 sources). Therefore, of 72 possible sources, losers identified most sources as helpful: 41 (56.9%) versus gainers, who identified only approximately half as many sources as helpful, compared to losers (25 [34.7%]; φ=–0.22, small-to-medium effect). In other words, of six possible sources, on average, losers believed 3.42 (SD, 1.24) sources helped motivate them, whereas gainers only considered 2.1 (SD, 1.00) to be helpful (d=1.17, large effect). Figure 4 clearly illustrates the similar trends from both studies and the collective difference indicating that losers, overall, reported benefiting from 62.8% more sources of positive motivation than gainers.
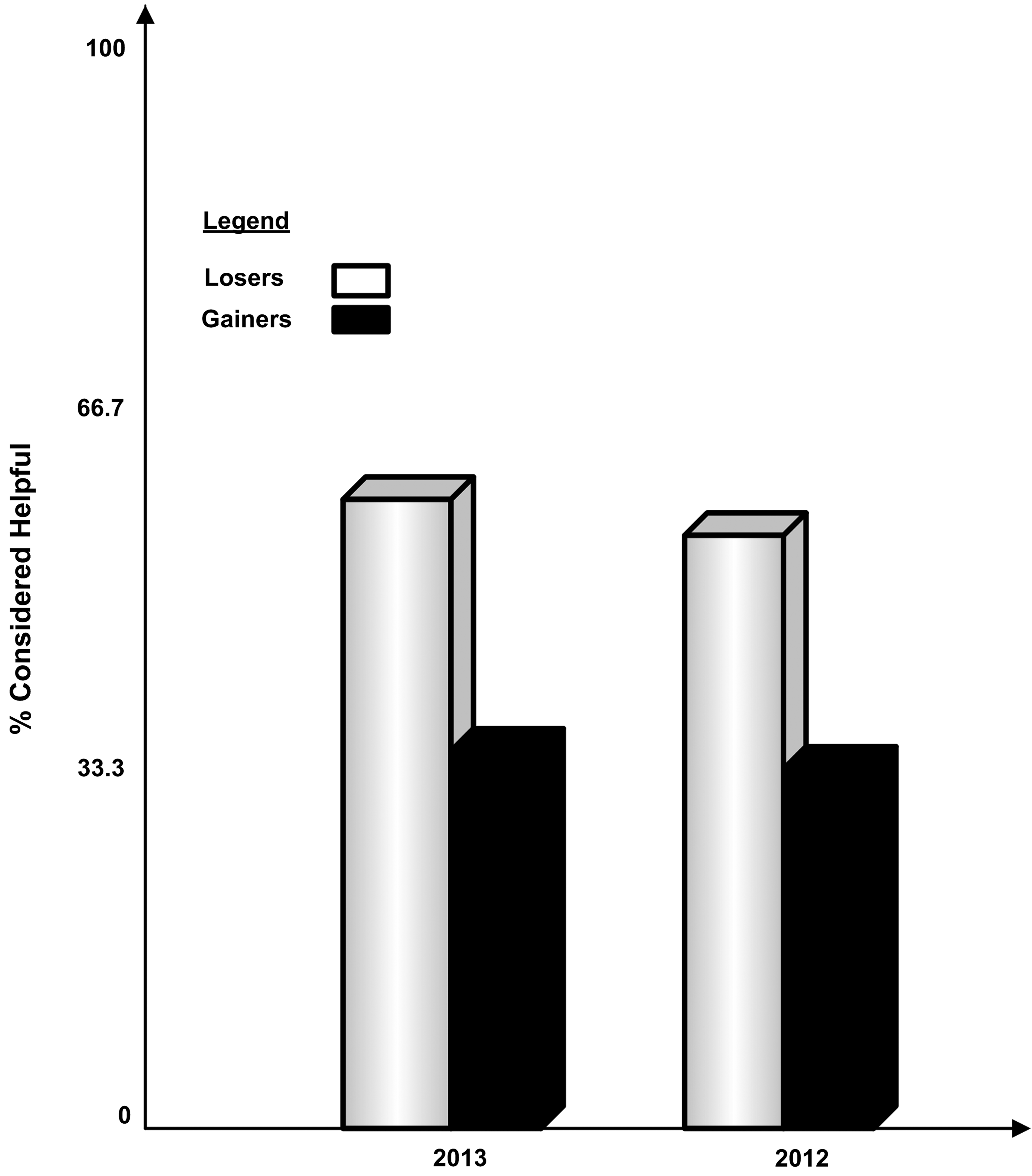
Sources of commitment considered helpful by losers and gainers in the 2012 and 2013 studies.
Discussion
Participants in this study spoke about key factors in their personal journeys toward permanent and substantial lifestyle change, illustrating what it takes to commit to living a healthier life, and maintain—or falter—in that pursuit. In accord with hypotheses, the common themes expressed by this group of young weight controllers mirrored, to a substantial degree, the sources of commitment reported by elite athletes identified in the SCM, as well as campers in our 2012 qualitative study.18,19 More specifically, the following sources of commitment seemed to affect these young weight controllers: SSF, SSP, VO, EmC, ExC, and II.
Losers versus Gainers
Overall, losers and gainers demonstrated important differences in their responses in the current investigation. Losers reported that their parents provided more support than gainers (8 of 8 losers vs. 5 of 8 Gainers). Although losers did seem to find a wider array of sources as helpful overall, losers and gainers did not demonstrate major differences in their endorsement of other sources of commitment (SSF, VO, EmC, ExC, and II). Differential use of particular sources of commitment seems less noteworthy than the degree to which losers found a wider array of sources as helpful to their efforts. The losers identified as helpful 66.7% more of the six possible sources, compared to gainers. The 2012 investigation elicited similar results. Comparison of the similar trends from both studies indicated that losers reported benefiting from 62.8% more sources of positive motivation than gainers.
As expected, losers demonstrated reactions much more in accord with the HOM than did gainers to many hypothetical high-risk situations from the WTCI (10 of the 27 questions). The losers seemed to respond differentially, particularly to situations (exams and fights with friends) in which they reported themselves likely to use increasing their activity levels to cope with stressors. However, in the remaining 17 questions about the hypothetical situations, loser and gainer responses showed similar patterns, with neither group showing greater or lesser degrees of healthy obsessions.
Healthy Obsession Model
The HOM suggests that successful weight controllers sustain a preoccupation with planning and executing such target behaviors as eating very little fat, maintaining a high level of activity, and self-monitoring (of food, activity, and weight). In a recent study, for example, highly successful weight controllers, far more than obese individuals who were seeking treatment, maintained dietary restraint very consistently. 26 In a different arena, Perri and colleagues found, contrary to their expectations, that more-demanding (obsessive-type) goals produced better outcomes for adults who wanted to improve their activity levels. 27 Those assigned to an extreme goal (walk 5–7 days per week) walked more and maintained their higher activity levels over time, compared to those assigned to a moderate goal (walk 3–4 days per week). In accord with the HOM, losers in the present and previous qualitative study by our group 18 reported eating a very-low-fat diet, as well as self-monitoring food, activity, and weight, far more consistently than gainers. The fact that the sources of commitment identified in another group that relies on healthy obsessions (elite athletes) appeared to capture the themes identified by young weight controllers also supports the viability of the HOM.
In addition to reporting substantial differences directly in most key weight-controlling behaviors, losers responded to the eight hypothetical situations posed in the WTCI questionnaire very much in accord with predictions based on the HOM. In their responses to these hypotheticals, losers told the story of their relentless commitment and focus in a way that suggests that successful weight controllers not only rely on similar sources of commitment to elite athletes, but they also show an intensity and dedication to their programs that mirrors the commitment to training witnessed in elite athletes.11,12,19,22,25 These healthfully obsessed individuals do not seem to let the usual ebbs and flows of daily life distract them from their primary goals every day. For example, 100% of the losers thought that they would manage high-risk situations involving fights with best friends or attendance at pizza parties by still reaching their daily goals for fat consumption (<20 g) and activities (>10,000 steps), whereas approximately half of the gainers thought they would reach their goals on such days.
Further, losers again demonstrated more-substantial healthy obsessions than gainers. Losers reported that the fight with their friend would not impact their weight control programs, whereas gainers expected negative outcomes. For example, one loser stated, “I'll suck it up and do what I need to do. It wouldn't affect me.” Similarly, another loser reported, “It [fight with friend] doesn't impact my activity; well, to me that's a nonrelated event. You must exercise and you cannot let things hinder you.” In contrast, a gainer stated, “Um, I'd sit there eating frozen yogurt and watch TV and cry. It affects me very much when I get into an argument.” Another gainer mentioned, “Lower it [my activity] dramatically.” Losers also used more-definitive language about their plans, whereas gainers used language such as “probably” and “I guess,” illustrating less confidence in their responses. For example, one loser stated, “Yes [I have a plan]. I'll bring a lean cuisine. I don't care what people say.” Another loser stated, “Yes, I would eat before. It's a little trick that I do, because if you are already full you are not going to eat anything else. And just be like ‘oh, no I am not hungry thank you.’ I would definitely eat before and make sure that it was fulfilling food so that I am satisfied.” In contrast, a gainer predicted, “Probably eat one plate and a few chips and go hang out.” Losers also, far more than gainers, treated potential adversity by planning and problem solving in order to stay on track—very much like athletes do to maintain their level of training. 19 This differential focus on planning by successful weight controllers observed here and in other studies15,18,26 speaks to the heart of healthy obsessions. Those with healthy obsessions seem to keep their focus on target behaviors more top of mind under a variety of conditions. They may have learned that such attentiveness helps them manage the many challenges posed by the obesogenic culture and their own biologies—creating essentially a readiness to do battle with such forces at any moment.
Immersion CBT treatments may be especially helpful in generating and nurturing healthy obsessions for people, as with the losers in this study, who seemed to have substantial support at home and a tendency toward conscientiousness. 10 The actual experience of rapid weight loss along with CBT and extensive modeling by staff may accelerate self-reactions, such as favorable self-efficacy and intense commitments, to the target behaviors that produced such dramatic and positive changes in weight and fitness. Coinciding with positive commitments to target behaviors, weight controllers, as with the present losers and 2012 study losers, may keep themselves on track by reacting very strongly to lapses and weight gains. Refusing to simply rationalize away such challenging moments, and instead using negative reactions to them to re-energize more-constructive behaviors, may prove vital for long-term success.1,11,17
Sources of Commitment
The weight controllers in this sample cited social support of parents as the most common source of their motivation. This is consistent with the findings of Gierut and colleagues' 18 preliminary investigation in that successful weight controllers reported using their social resources in order to find motivation to continue their efforts. As advised in the parent workshops conducted in Wellspring's programs, parents and other family members have the ability to operationalize their support by eliminating all fats from the home, ordering according to the program's principles at restaurants, and wearing pedometers to monitor their steps every day. This finding about the potential power of social sources of commitment coincides well with research on treatment for adolescent obesity that consistently finds better outcomes associated with highly supportive families. 19 It also suggests that treatments, including most weight loss camps in the United States currently, other than Wellspring, 10 that do not make parent involvement a key component, most likely do their clients a major disservice.
The apparent impact of social support on successful weight control would surprise almost no one. However, no previous investigation has reported that successful weight controllers may use a wider variety of motivators than unsuccessful weight controllers. Combining the results of this study and the 2012 research from our group, 18 we found that losers used 64% more sources of commitment than gainers. Losers seem to find more ways to stay committed to their weight control programs by relying on their families, friends, and institutions in a notably different way than gainers. In other words, losers may find (see) sources of inspiration from a wider array of people and places than gainers. We do not know whether losers provide the primary impetus for this greater use of diverse motivators or whether those around them help make that happen for them. They could also simply live, go to school, and work in more-fortuitous health-promoting environments that positively impact their weight-controlling behaviors.
Regarding environmental influences, whether shaped by weight controllers or others around them, a variety of studies testify to the power of positive environmental influences on successful weight control. For example, Gorin and colleagues 28 demonstrated a ripple effect from the weight-controlling behaviors of one spouse impacting the contents of food cabinets and, in turn, impact weight loss by their partners. In several other studies, researchers found that priming dietary concerns through exposure to health-related magazines, flyers, and posters inhibited eating of problematic foods by participants focused on weight control. 29 Takten together, the present results, and related studies of the impact of weight-controlling environments, suggest that helping weight controllers create a wide array of positive sources of motivation may help them succeed. This could involve surrounding themselves with supportive people, keeping weight-controlling cues around them (e.g., images on the walls, healthful magazine subscriptions and websites, and food in the cabinets and refrigerators), and finding places that prompt healthful eating (e.g., certain restaurants) and movement (parks and health clubs).
Limitations of This Study
The small sample and qualitative nature of this study allowed for a thorough and rich analysis of the perceptions of these young weight controllers. However, these identical qualities—sample size and qualitative methodology—also limit the scientific merits of this approach. The participants in Wellspring's CBT immersion programs learn a particular language and conceptualization of the process of weight control. The successful—and some unsuccessful—participants responded in ways consistent with those messages. On the other hand, their reports of their behavioral consistencies clearly resembled the behaviors (high levels of activity and consistent self-monitoring) of most other highly successful weight controllers—and, as such, lends credence to their self-reports.22,26 In addition, the specificity and richness of their comments, and the novelty of some of the findings (e.g., losers seeing sources in a wider variety of places), suggests that the losers embraced the HOM to change their lives, not just to please the staff from Wellspring.
Differences in the samples of losers and gainers in this study also warrant comment. The selection process described in the Methods section made it clear that these participants were not randomly selected from Wellspring's camps. They were volunteers who were matched on certain characteristics across the groups to a reasonable extent. That matching procedure still resulted in some discrepancies. Gainers were somewhat younger and more overweight than losers. It is difficult to know how these factors impacted outcomes in this small sample study. For example, younger participants might be expected to become more successful owing to higher levels of oversight and support at home. Also, greater initial excess weight may result in greater weight losses and perhaps even higher levels of commitment to succeed. In the present sample, however, these factors (younger, more overweight) were associated with markedly poorer, not better, outcomes. Clearly, more-objective, larger-scale tests of the HOM will provide more-complete evaluations.
One direction for further study could include adapting the WTCI in terms of brevity, using less-complex language, and administering to all participants as multiple time points (initial, post, and follow-up camp) to provide objective data on a larger number of participants. However, in order to administer the WTCI and other tests to a larger sample, it will be necessary to develop more-effective recruitment strategies than the one used in the present research. Greater financial incentives might help, perhaps including the requirement of substantial deposits from participants and families to be returned contingent on provision of follow-up data.
Last, experiments that directly compare the impact of immersion treatment to other interventions may prove especially useful if they test for the degree to which immersion plus CBT enhances healthy obsessions, as predicted by the Immersion to Lifestyle Change 10 and Healthy Obsession models.11, 12, 22
Conclusions
The present study once again supported the viability of the HOM. It may help all weight controllers to focus on developing and nurturing healthy obsessions. This begins with an emphasis for weight controllers on the vital role of systematic, highly consistent self-monitoring.12,13,15,18,22,26 Previous research has demonstrated that consistency of self-monitoring, even within the first weeks of treatment, can predict long-term success.33 Therefore, clinicians would be well advised to target self-monitoring as a key process goal and take steps to improve its consistency through prompts, simplification and novelty of approach (e.g., with apps on smart phones), and reinforcement.22,30
The most interesting and novel finding in the present and the previous qualitative follow-up study of the impact of Wellspring Camps was that successful weight controllers differentially used a wider variety of sources of motivation. In addition, the findings about motivational factors in these two studies suggest that young weight controllers may find it especially beneficial to learn how to use diverse sources of commitment. Clinicians can promote this by teaching the range of sources of commitment studied in these qualitative studies directly, taking weight controllers on outings (outside of offices) and helping them see potential motivators (e.g., overweight people struggling to walk and fit people jogging). Role playing various scenarios and journaling by weight controllers could also help extend the range of potential sources of commitment.
Footnotes
Acknowledgments
The authors acknowledge, with appreciation, a grant received from the Association for Applied Sport Psychology that partially funded the present research. A version of this article was presented at the meeting of the Association for Applied Sport Psychology, New Orleans, Louisiana, October 2013.
Author Disclosure Statement
The authors were employed, in part, by Wellspring, a company that offers immersion treatment at therapeutic weight loss camps throughout the United States and in England.