
Abstract
Abstract
Background:
RealFit is a 13-week weight reduction program for youth that focuses on nutrition, physical activity (PA), psychology, and parental participation. The short-term effectiveness of the RealFit intervention, in terms of body composition, aerobic fitness, and dietary and PA behavior, having been proven, the present study evaluated the long-term effects of the intervention.
Methods:
The study had a quasi-experimental design. Height, weight, waist circumference, aerobic fitness, and self-reported dietary and PA behavior were assessed at baseline (T0), immediately after the 13-week RealFit intervention (T1), after 5 months (T2), and 1 year (T3) of follow-up. A total of 86 adolescents participated in the intervention group. The control group (n=32) comprised overweight adolescents who did not receive any treatment.
Results:
One year after the RealFit intervention, significant decreases in BMI z-score (mean difference [MD]: −0.39) and waist circumference (MD, −3.24) were found. The comparison between the intervention and control groups, controlling for confounders, resulted in a significant difference (BMI z-score: −0.41; 95% confidence interval [CI]: −0.67 to −0.15; waist circumference: −8.07; 95% CI: −11.58 to −4.56). The results for dietary and PA behavior consistently showed favorable changes in the intervention group.
Conclusions:
The RealFit intervention appears to have significant favorable long-term effects on BMI z-score and waist circumference. These changes in body composition obviously represent changes in adolescents' energy balance-related behavior. Taking all results and limitations into account, it may cautiously be concluded that RealFit is an effective weight loss intervention.
Introduction
Overweight and obesity are world-wide health problems, whose prevalence, among both adults and youth, has increased dramatically in recent decades. 1 Globally, approximately 180 million children (<18 years) are overweight.2,3 In The Netherlands, 13–15% of children (ages 2–21 years) are overweight, a 2- to 3-fold increase compared to the 1980 prevalence rates. 4 More specifically, research conducted by the Public Health Services (GGD) in the Southern Limburg region of the Netherlands (2010) has shown that 14.5% of boys and 16.3% of girls ages 13–14 years were overweight. In the 15–16 years age category, 16.1% of boys were overweight and 18.6% of girls. 5 These prevalence rates are alarming, because overweight can lead to health problems, such as type 2 diabetes (T2D), hypertension (HTN), dyslipidemia, cardiovascular diseases (CVDs), and metabolic syndrome, developing even at a young age. 6 In addition, overweight at a young age can lead to psychological problems (e.g., loneliness, sadness, and low self-esteem), 7 and overweight children are at higher risk for being overweight in adulthood.8–10
In response to the rising overweight prevalence, the RealFit intervention was developed in 2003 by three collaborating regional health organizations (GGD Westelijke Mijnstreek, Huis voor de Sport Limburg, and Thuiszorg Westelijke Mijnstreek). RealFit is, unlike most other standard weight treatments for overweight adolescents, a non-school-based program, which is implemented in a group and consists of four components: nutrition; physical activity (PA); psychology; and parental participation.11–13 The primary goal of RealFit is to reduce or stabilize weight by intervening on multiple energy-balance–related behaviors (i.e., increasing PA [in daily life] and the consumption of fruit and vegetables), but also reducing sedentary behavior and the consumption of food and beverages with a high content of saturated fat and/or sugar.13,14 To achieve this, the RealFit intervention includes nutrition and PA lessons. The PA lessons also aimed to increase the level of physical fitness, which is associated with total and abdominal adiposity, CVD risk factors, and it has a positive effect on depression, anxiety, self-esteem, and academic performance. 15 Besides this, several (review) studies have demonstrated that a combination of psychology lessons and diet and/or PA interventions enhance weight loss by identifying and modifying aversive thinking patterns and mood states to facilitate weight loss, thereby achieving a modest, sustainable weight loss.13,16–18 Hence, the added psychological lessons are crucial to prevent adolescents from regaining weight immediately after the intervention and successfully maintain the healthy behavior in the long term. 13 Finally, parental participation is an important part of RealFit. Greater involvement of family members has been shown to increase the effectiveness of weight-related interventions.19–22 When parents are conscious of appropriate weight loss behavior, and able to reinforce this to the benefit of their child, they provide an optimal social and physical environment to facilitate healthier choices.22–24 Parental involvement has been recognized in several studies as an important feature of behavioral weight loss programs. 13
Since the start of RealFit, several studies, though with suboptimal research designs, have examined the effectiveness of the intervention.25–28 A study conducted by Croezen found a significant decrease in BMI in the short term, but no changes in aerobic fitness or self-esteem. 25 Mulkens and colleagues underlined the importance of the added psychological lessons: This resulted in a greater decrease in BMI and an increase in self-esteem in the short term, compared with the earlier (standard) RealFit version.26,27 A study by Slinger and colleagues showed a favorable short-term effect on BMI, hip circumference, and blood pressure. 28 The results of all studies have led to further improvements to the RealFit intervention. Although these improvements and the favorable short-term effects are promising, the effects in the long term have not yet been investigated. The aim of the current study was therefore to investigate the long-term effects of RealFit on body composition, aerobic fitness, and behavior.
Methods
Study Design
The current study had a quasi-experimental design. Measurements took place before the start of the intervention (T0, baseline), immediately after the intervention (T1), at 5-month follow-up (T2), and at 1-year follow-up (T3). Ethical approval for the study was obtained from the ethics committee of the Faculty of Psychology and Neuroscience of Maastricht University (Maastricht, The Netherlands).
RealFit Intervention
RealFit is a 13-week group-based intervention for adolescents (ages 13–18). Each RealFit group consists of maximum 15 participants (for more details about the intervention, see Table 1).
The RealFit Intervention
Combined nutrition and psychology lesson.
Before the start of RealFit, an information meeting was given for interested adolescents and their parents. The goal and intentions of RealFit were discussed during this meeting, where it is clearly stated that losing weight is not the main goal. The participants should work on becoming conscious of healthy behavior and feeling more fit. One week after this information meeting, the RealFit intervention started.
In total, seven different RealFit groups started (average of 12 participants per group), where each group had their own professional team (dietician, sports instructor, and psychologist). This team filled out a logbook of each lesson to inform each other during the intervention. Three of seven RealFit groups started during spring 2011, three started during autumn 2011, and one started during spring 2012. To facilitate all seven RealFit groups, three psychologists, four dieticians, and five sports instructors were used. All these professionals received a full day of training and a manual with among others detailed information about each lesson.
Implementing RealFit in a group was primarily done in order to increase the feeling of relatedness as one of the three basic psychological needs underlying human motivation. Previous studies have shown that interventions with a focus on the three psychological needs of the self-determination theory (relatedness, competence, and autonomy) increase autonomous types of motivation and thereby have a better chance of achieving behavior maintenance.29–32 Autonomy-supportive coaching techniques (step-wise skills training, positive reinforcement, motivational interviewing, and creating awareness of adolescents' free choice regarding PA and dietary behavior) were used to promote the other two psychological needs: the participants' feelings of autonomy and competence.29,31,32
RealFit consists of four main components:
1. Exercise lessons: The thirteen 1-hour group exercise lessons were led by the sports instructor and included endurance training, strength training, and/or circuit training. The aim of these lessons was to increase aerobic fitness, show the many possibilities of PA, and let the participants experience that PA feels good and can be fun. 2. Nutrition lessons: The three 1-hour group nutrition lessons were led by the dietician. The subject matter of the lessons mainly focused on the importance of increasing the consumption of fruit and vegetables and reducing the consumption of food and beverages with a high content of saturated fat and/or sugar, as well as on how the participants could achieve this. In addition to these three lessons, each participant received personal advice from the dietician during three individual sessions, in which their personal situation was discussed and an action plan was designed to improve the participants' eating behavior. 3. Psychological lessons: Ten 1-hour group psychological lessons were led by the psychologist. The lessons comprised three different components: (1) cognitive therapy, based on cognitive theory, where the participants were taught to replace negative irrational cognitions about food, eating, body weight (or body shape), and the self as a person by more-rational cognitions
33
; (2) social skills, to improve their ability to maintain healthy behavior in certain difficult situations (e.g., when food is offered)
34
; and (3) cue exposure, to decrease craving (e.g., for high-caloric food): Conditioned stimuli (cues, such as the presence of high-caloric food) were detached from conditioned responses (binge eating) by smelling the food without eating it, thereby extinguishing craving.
35
4. Parental participation: The intervention included three 1-hour parental group meetings, led by the dietician, psychologist, and sports instructor, to increase the parents' awareness of their child's overweight and provide them with advice on how to help their child change his or her behavior. For example, specific parenting practices, such as giving the child social support and being involved in the child's life, were addressed in order to provide a social environment to help the child reach his or her goal. In addition, the responsibility of the parents as a role model for their children was extensively discussed during the meetings.
Intervention Group
Participants of the seven different intervention groups were recruited by pediatricians and dieticians, as well as through advertisements in newspapers, face-to-face promotion campaigns, and public relations materials disseminated in schools, pharmacies, libraries, and physiotherapy practices in the South Limburg region. The inclusion criteria were age between 13 and 18 years and being classified as overweight or obese based on the BMI cut-off points proposed by Cole and colleagues. 36 All participating adolescents and their parents signed an informed consent form. A total of 86 participants were included in the RealFit intervention between February 2011 and February 2012.
Control Group
The participants in the control group (n=32) were recruited in three different ways. First, adolescents who were on the waiting list for the RealFit intervention (n=17) were asked to participate in the control group. Eight of them accepted. Second, the Youth Health Care service recruited 20 participants during regular healthcare contacts. When an adolescent was classified as overweight or obese, he or she was invited to participate in the control group. They had no option to join the intervention group. Third, 19 adolescents signed up for the seventh RealFit group. Because only 15 adolescents could participate in the RealFit intervention, the other 4 participated in the control group. This selection was done by randomization. The same inclusion criteria and informed consent form were used for the control group. This group did not receive the RealFit intervention, or any other treatment beyond care as usual, which means that they did not receive any additional care or attention relative to their normal weight age group. The participants were included between February and June 2012. A total of 32 adolescents were included in the control group.
Primary Outcome Measures
The primary outcome measure of this study was body composition, assessed by BMI z-score and waist circumference. BMI (calculated from height and weight measurements) and waist circumference were assessed by the dietician during a personal consultation based on a standardized protocol. Age- and gender-specific BMI cut-off points were used to define overweight and obesity. 36 Additionally, BMI was converted to a standardized z-score, adjusted for age and gender, based on reference data from the Fourth Dutch National Growth Study. 37
Secondary Outcome Measures
Secondary outcome measures were aerobic fitness and dietary and PA behaviors. Aerobic fitness was assessed by the sports instructor using the Åstrand test. This is a validated submaximal test where the participant has to cycle for 6 minutes at a specific workload. 38 Workload and mean heart rate are then used to estimate the VO2max for boys and girls.38–44 VO2max provides important information about the capacity of the cardiorespiratory system 43 and is used as the gold standard to assess aerobic fitness.40,45 Changes in dietary and physical activity behavior were assessed by the Food Frequency Questionnaire (FFQ) and the Physical Activity Questionnaire for Adolescents (PAQ-A).46–48 Both questionnaires are valid, reliable instruments and are regarded as the national standard.46,47,49 The FFQ, consisting of 19 items, assesses daily food intake (breakfast, fruit, vegetables, beverages, and snacks) by asking, for example, “How often do you eat fruit in a normal week?” and “How much do you eat at one time?”. The PAQ-A assesses PA and sedentary behavior during the last 7 days. 49 The questionnaire consists of 12 items, with questions about active transport to school, PA at school, PA at or outside a sports club, and time spent watching television and using a computer. The questions are structured on the basis of a segmented time-of-day or day-of-the-week strategy (e.g., first, “How often did you exercise at a sports club last week?” and then, “How long did you exercise at a sports club on each occasion?”). The participants filled out both questionnaires online or on paper immediately after the primary outcome measurements.
Statistical Analysis
Data were analyzed using SPSS 21.0 software (SPSS, Inc., Chicago, IL). The general characteristics of the intervention and control groups were analyzed using descriptive statistics. Pearson's chi-square tests and independent t-tests were conducted to analyze the comparability of the two groups at baseline. Multivariate linear regression analyses were used to examine the differences between the intervention and control groups at 1-year follow-up, compared with baseline, while controlling for age, gender, BMI z-score at baseline, and the baseline measurement of the dependent variable. Multilevel analyses were used to study possible differences between the seven RealFit intervention groups, but yielded no significant results. Possible moderators of outcome could not be examined because some subgroups became too small to analyze. Therefore, both multilevel analyses and analyses of possible moderators are not discussed any further in this article.
There were some missing values for variables used in the analysis. In total, 70.1% of the cases in the intervention group and 79.3% in the control group were fully complete. Given that using complete cases only results in a loss of precision and may even introduce bias, regression imputation was used to replace the missing values with the estimate derived from the imputation model. 50 Alpha was set at 5%, whereas values between 5% and 10% were regarded as indicating a trend.
Results
Participants of the seven RealFit groups (N=67; 37.3% boys) had a mean age of 14.1 years (range, 13–18) and an average BMI z-score of 2.38 (56.7% were obese). The control group (N=29; 44.8% boys) had a mean age of 13.6 years (range, 13–16) and had a significantly lower BMI z-score (1.98), with 27.6% of the participants classified as obese (Table 2). Sixty-nine percent of the participants in the intervention group did not miss more than one RealFit lesson. In total, parental meetings were visited by 84% of the participants' parent(s). Nineteen participants dropped out during the intervention or did not participate in at least two measurements. In the control group, only 3 participants dropped out. The participants who dropped out did not significantly differ from other participants.
Demographic and Baseline Characteristics of the Intervention and Control Groups a
Low educational level: lower secondary vocational education (VMBO).
High educational level: higher general secondary education (HAVO) or pre-university education (VWO).
Bold p value=significant/trend difference.
Data are presented as percentage or as mean (±standard deviation).
Pearson's chi-square.
Variances not equal.
Primary school, free school.
Trend (p<0.10); **significant (p<0.05).
Primary Outcome Measures
One year after the RealFit intervention, a significant decrease in BMI z-score was found in the intervention groups (mean difference [MD]: −0.39), compared with baseline (Fig. 1; Table 3). The BMI z-score in the control group had not changed after 1 year (MD, 0.13). The comparison between the intervention and control groups resulted in a significant difference (–0.41; 95% confidence interval [CI]: −0.67 to −0.15). One year after RealFit, waist circumference had decreased significantly in the intervention groups (MD, −3.24), compared to baseline (Table 3). The opposite effect was found in the control group (MD, 3.70). Comparing the intervention and control groups resulted in a significant difference (–8.07; 95% CI: −11.58 to −4.56).
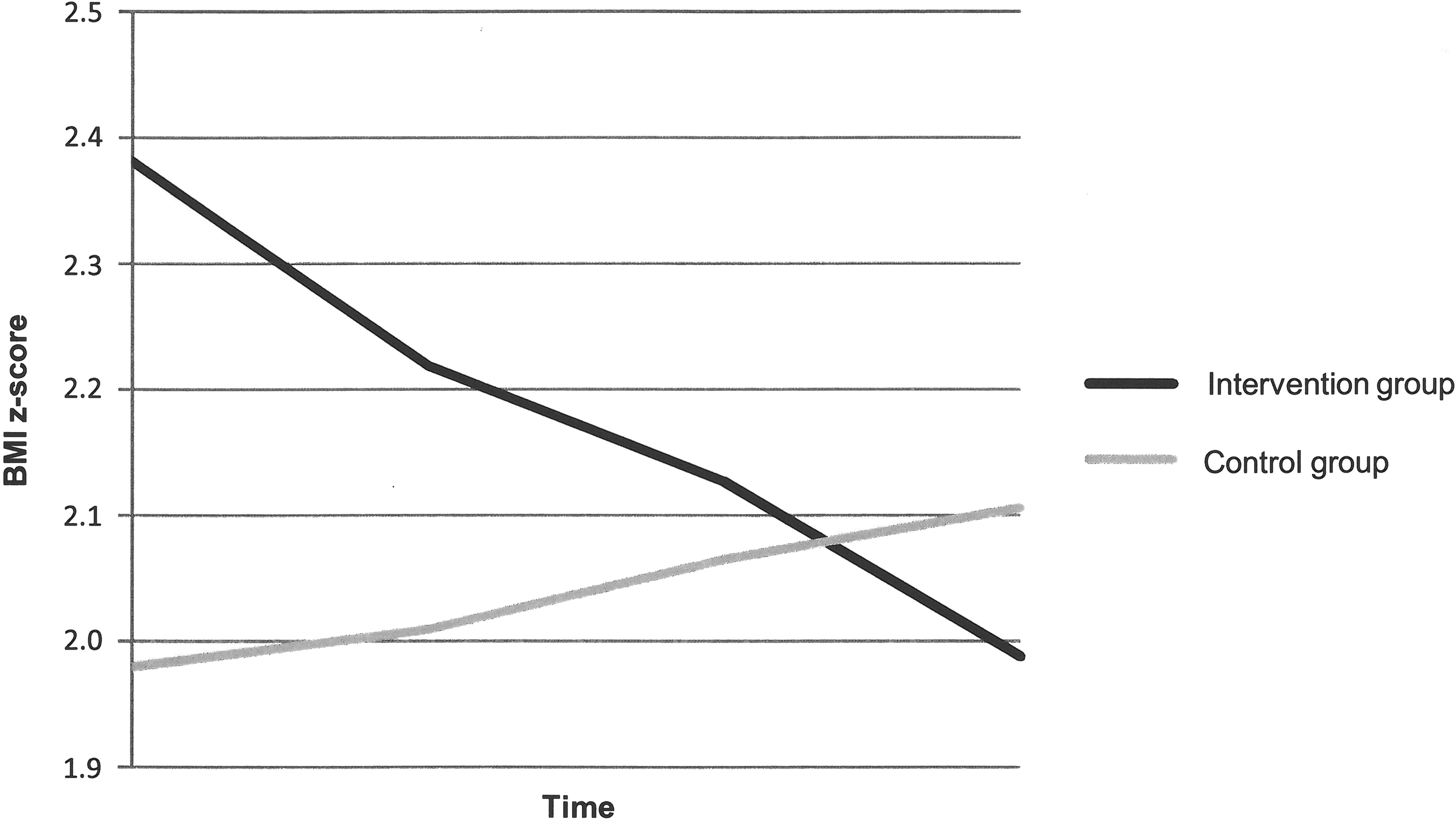
Changes in BMI z-score.
Bold p value=significant/trend difference.
Data are presented as mean (±standard deviation).
Adjusted for age, gender, BMI z-score, and baseline.
Trend (p<0.10); **significant (p<0.05).
Abbreviation: CI, confidence interval.
Secondary Outcome Measures
Analyses of aerobic fitness data showed a significant increase 1 year after RealFit in the seven intervention groups (MD, 3.61), compared with baseline (Table 3). No changes were found in the control group (MD, −0.63). The comparison between the two groups revealed a difference of 3.42 mL/kg/min (95% CI: −0.22 to 7.06), a difference that did not reach significance.
Figure 2 shows the percentage of change (percent of increase/decrease 1 year after RealFit, compared with baseline) in dietary and PA behavior in the intervention and control groups. The number of participants who joined a sports club significantly increased in the intervention groups (+20.9%), and they enjoyed PA significantly more than at baseline (+14.9%).
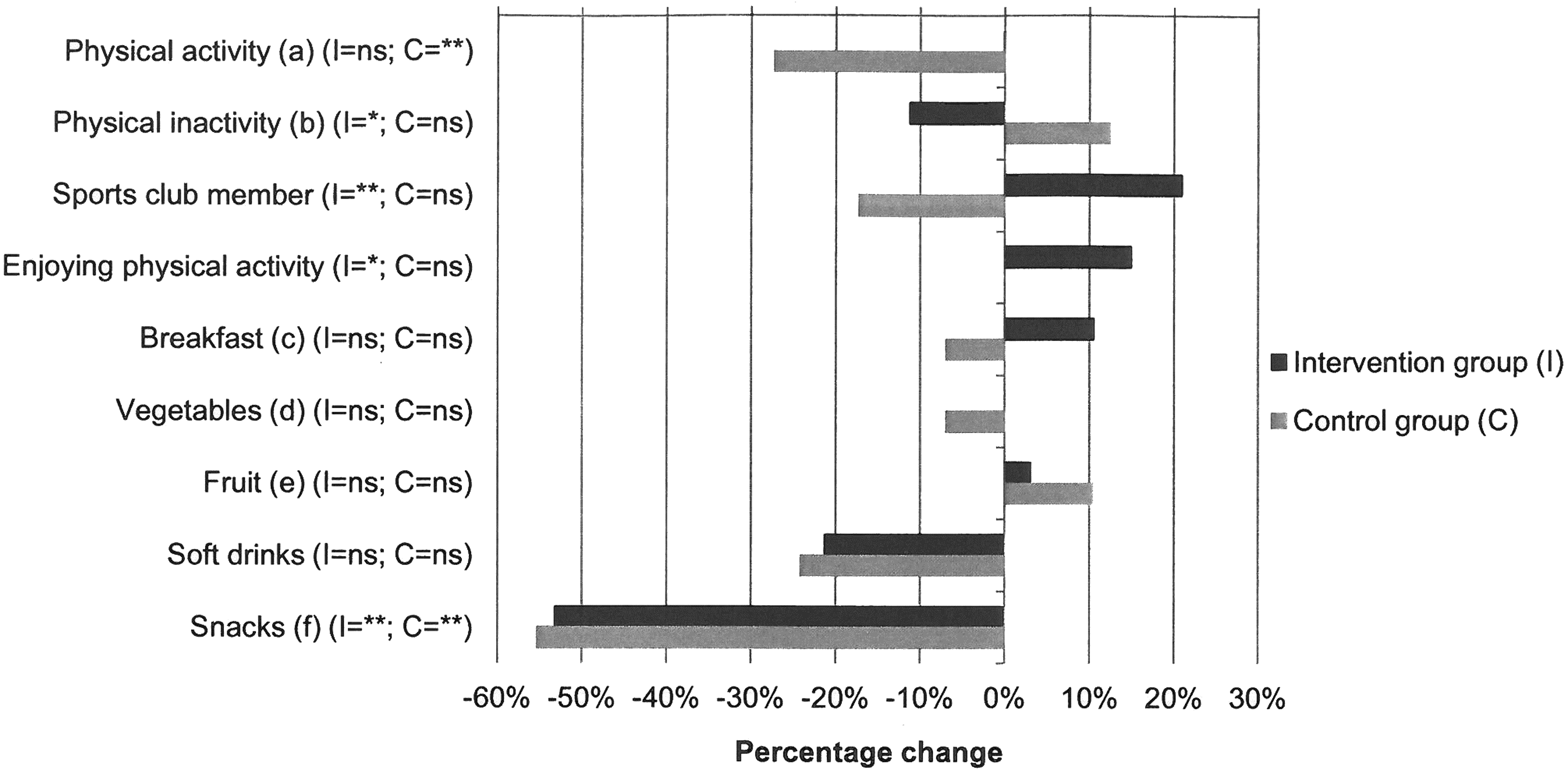
Percentage change between baseline (T0) and 1-year follow-up (T3) on dietary and physical activity behavior for intervention and control group. Paired t-test (continuous variables) and McNemar's test (dichotomous variables) is used. ns, not significant. *Trend (p<0.10); **significant (p<0.05). (A) Dutch Healthy Physical Activity Guidelines for children: 60 minutes of moderate activity per day. (B) Minutes per day of watching television or using a computer. (C) Has breakfast minimum of five times per week. (D) Consumes a minimum of 200 g/day. (E) Consumes a minimum of two portions per day. (F) Consumption of snacks and candy.
Overall, the secondary outcome changes in the intervention groups did not significantly differ from those in the control groups, but they were all in a favorable direction, except for vegetable consumption (no change).
Discussion
The current study examined the long-term effect of the RealFit intervention on body composition, aerobic fitness, and behavior, using a control group for comparison. The results indicated that BMI z-score and waist circumference significantly differed between the intervention and control groups. Both outcomes decreased in the intervention groups, whereas they did not change, or even increase, in the control group (Table 3; Fig. 1). Kolsgaard and colleagues showed that even a small reduction in BMI z-score (0.00<z<0.10) is associated with improved insulin resistance, decreasing the risk of T2D and CVDs. 51 The lower waist circumference shows that abdominal fat had decreased, which is associated with a lower risk of diabetes, HTN, and CVDs.52–54 Based on these results, it may cautiously be concluded that the decrease in BMI z-score and waist circumference in the intervention group can be considered a positive intervention effect of RealFit.
Also, long-term favorable changes in aerobic fitness were found (see Table 3). Findings of several other studies showed that at least three vigorous PA lessons a week are required to improve aerobic fitness.55,56 The 13 once-per-week PA lessons in RealFit can therefore only be regarded as a starting point for the participants. With these lessons, RealFit aimed to improve the participants' confidence and internal motivation to become and remain physically active. Compared with baseline, a larger proportion of the participants had indicated that they joined a sports club 1 year after RealFit (see Fig. 2). If this indication is correct, it can be a possible explanation of why no decline in PA was found, even though such a decline is common among adolescents. 56
No significant difference in PA or dietary behavior was found between the intervention and control groups (see Fig. 2). However, the significant changes in body composition obviously represent changes in the participants' energy-balance–related behavior. The small, nonsignificant favorable changes in many different health behavior factors, which were shown in the results, can indeed lead to a significant favorable effect on body composition. 14 This effect is exactly what RealFit aimed to achieve: not focusing on extreme changes in one or two health behavior factors, but slightly improving multiple behaviors and giving the participants the autonomy and skills to maintain these behaviors in daily life in the long term, given that it is the coexistence and interaction of all specific nutrition and PA behaviors that determine the occurrence of a positive energy balance and weight gain.14,57 Achieving a healthy and active lifestyle by improving energy-balance–related behavior may lead to a reduced risk of cancer, CVDs and T2D.57,58
Limitations
The current study was subject to several limitations. First, the study was implemented in real-life conditions. Although this is, in fact, a strong point, given that interventions that are pilot tested in real life have a greater chance of implementation and dissemination when proven effective,59,60 real-life–based research also involves measurement issues. For example, the prescribed follow-up period between the measurements was sometimes not fully adhered to because of lack of time on the part of the sports instructors and dieticians.
Second, the sample size was relatively small. A lot of effort was put into the recruitment of adolescents; but, despite that, recruitment took longer than planned and was still relatively small at the end. Unfortunately, as a result of this relatively small sample size, some subgroups became too small to examine the effect of possible moderators.
Third, it appeared difficult to keep participants motivated for the measurements after the RealFit intervention had ended, which had an impact on the number of complete cases. This is why regression imputation was used, a valid, commonly used method to enable all collected data to be utilized. 50 Complete case analysis showed no differences in results.
Next, no objective information was available about whether the participants from the control group participated in another weight loss program, although the researcher who performed all the measurements in the control group asked about this at every measurement, and did not hear from anybody that they were following a weight loss program somewhere else.
Further, the questionnaires had their limitations, owing to the fact that these are subjective measurements and can lead to social desirability bias on the part of the participants. This is why, for instance, the possible change in PA was measured not only by means of a questionnaire, but also objectively by measuring aerobic fitness with the Åstrand test.
Finally, the baseline analyses showed some significant differences between the intervention and control groups, which may be the result of the fact that no full randomization was used. Also, a part of the control group (n=20) was not actively looking for a weight loss intervention and therefore probably differed from the intervention group in ways that were not measured (e.g., motivation or intent to change). Controlling for baseline variables, such as age, gender, and BMI z-score, in all analyses at least eliminated the effect of the measured significant baseline differences in these factors.
Conclusions
The RealFit intervention appears to have significant favorable long-term effects on BMI z-score, waist circumference, and aerobic fitness. Dietary and PA behavior changed in a favorable direction in the intervention groups. Taking all results and limitations into account, it may cautiously be concluded that RealFit is an effective weight loss intervention that is feasible in real-life conditions.
Footnotes
Acknowledgments
This study has been supported by a grant of the Netherlands Organization for Applied Scientific Research (TNO), Netherlands Institute for Sport and Physical Activity (NISB), and the Mulier Institute, Center for Research on Sports in Society. The funding agency had no role in the design, conduct, or data analysis of this study.
Author Disclosure Statement
No competing financial interests exist.