
Abstract
Abstract
Background:
Pacific Kids DASH for Health (PacDASH) aimed to improve child diet and physical activity (PA) level and prevent excess weight gain and elevation in blood pressure (BP) at 9 months.
Methods:
PacDASH was a two-arm, randomized, controlled trial (ClinicalTrials.gov: NCT00905411). Eighty-five 5- to 8-year-olds in the 50th–99th percentile for BMI were randomly assigned to treatment (n=41) or control (n=44) groups; 62 completed the 9-month trial. Sixty-two percent were female. Mean age was 7.1±0.95 years. Race/ethnicity was Asian (44%), Native Hawaiian or Other Pacific Islander (28%), white (21%), or other race/ethnicity (7%). Intervention was provided at baseline and 3, 6 and 9 months, with monthly supportive mailings between intervention visits, and a follow-up visit at 15 months to observe maintenance. Diet and PA were assessed by 2-day log. Body size, composition, and BP were measured. The intervention effect on diet and PA, body size and composition, and BP by the end of the intervention was tested using an F test from a mixed regression model, after adjustment for sex, age, and ethnic group.
Results:
Fruit and vegetable (FV) intake decreased less in the treatment than control group (p=0.04). Diastolic BP (DBP) was 12 percentile units lower in the treatment than control group after 9 months of intervention (p=0.01). There were no group differences in systolic BP (SBP) or body size/composition.
Conclusions:
The PacDASH trial enhanced FV intake and DBP, but not SBP or body size/composition.
Introduction
Obesity remains an important problem in the United States; primary prevention must start in childhood. Seventeen percent of 2- to 19-year-olds in the United States were obese in 2011–2012. 1 Hypertension (HTN) has been shown to increase with obesity in children, resulting in recommendations of weight management for children. 2 However, few trials targeting prevention of weight gain and an increase in blood pressure (BP) have been done in young children. Additionally, few trials have been conducted in the Pacific region or in Asian and Pacific Islander populations, such as those that are found in Hawaii.
The Pacific Kids DASH for Health (PacDASH) intervention was built on the successful Dietary Approaches to Stop Hypertension (DASH) trials conducted in white and black adult populations 3 and previous work in an adolescent population, 4 approaches of which have become the basis of US dietary recommendations. 5 The DASH approach is a diet high in fruit and vegetables (FV), high in whole grains and legumes, high in low- or nonfat dairy products, moderately high in protein, low in red meat, and low in fats and sweets. 6 The PacDASH trial promoted these six dietary messages and also aimed to increase active play (the term dash also refers to running or rapid movement) and decrease screen time among children, which is important for weight management as well as healthy growth and development.
The PacDASH trial was designed by the investigators (R.N. and C.N.) and set in the clinic environment of Kaiser Permanente Hawaii (KP). The trial provided protocols and staff time to help parents and health providers meet the requirements of the study. The requirements of the parents included scheduling and attending their child's well-child visit, completing questionnaires, and, in the intervention group, making PacDASH-type food and physical activity (PA) opportunities available to their children. The requirements of the health providers included conducting qualitative assessment of dietary patterns and PA of pediatric patients at each well-child visit and, in the intervention group, providing supportive counseling to meet targeted goals. The assessment includes evaluation of self-efficacy and readiness to change, environment and social support, ability to address barriers to PA, meeting of national recommendations of 60 minutes of moderate or vigorous PA (MVPA) per day, decreasing sedentary behavior, and increasing the consumption of FV. This guidance is recommended by the American Medical Association/Health Services and Resources Administration/CDC Expert Committee Recommendations on Assessment, Prevention, and Treatment of Child and Adolescent Overweight and Obesity.7–9
The PacDASH intervention was designed to deliver tailored information to each member of the child, parent, and physician team. The information was specifically tailored to improve FV intake and PA level of each child based on his or her stage of readiness to change and self-efficacy. 9 Children were addressed directly, and parents assisted children as needed. The goal of PacDASH was to prevent excess weight gain and elevation in BP in a population with high rates of obesity and cardiovascular disease. 10
The aim of this study was to evaluate the efficacy of a clinic-based intervention that targets children of the Pacific Region who are in the upper half of the BMI distribution against recent US reference data (of a population that has increased in BMI over the years), in order to slow and prevent excess weight gain and, specifically, to test the effect of the PacDASH intervention on body size and BP among understudied multiethnic children in Hawaii, as well as to test whether behavior (PA and dietary) changes mediated the intervention's effect on health outcomes.
The primary hypothesis was that the intervention would result in changes by the end of the trial in the outcome variables of body size and BP, mediated by achieving the recommended level of FV consumption or of MVPA.
Methods
Subjects and Setting
KP covers approximately 20% of the state's population and was previously found to closely reflect the state's age distribution based on the census. 11 Inclusion criteria for PacDASH included: ages 5–8 years; BMI between the 50th and 99th percentile (initially ≥85th percentile, expanded to increase enrollment), based on CDC reference data 2000 12 ; primary care provider at one of four KP clinics; lives on Oahu; and due for, or scheduled for, a well-child/physical exam visit during months of the study. Exclusion criteria were: diabetes mellitus, polycystic ovarian syndrome, gastroesophageal reflux, gallbladder disease, nonalcoholic fatty liver disease, pseudo tumor cerebri, slipped capital femoral epiphysis, Blount's disease, obstructive sleep apnea/sleep disturbance, and other chronic disease conditions that would affect participation. Eighty-five 5- to 8-year-old children (62% female) enrolled.
Ethics
The study was approved by the institutional review boards at KP and the University of Hawaii (Honolulu, HI). Procedures followed were in accord with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Parental consent and child assent forms were sent in informational packets before the first visit, and written informed consent of the parent or guardian was obtained at the first visit. Children 7 years of age and older signed the assent; other children verbally assented. There were no adverse events among participants.
Design
The study was a 9-month randomized, controlled clinical trial with an additional 6 months of follow-up. Study visits occurred at baseline and 3, 6, 9, and 15 months (Table 1), spanning the period from August 31, 2011 (baseline started) to October 31, 2012 (follow-up maintenance ended). Condition assignment of 85 children (treatment, n=41; control, n=44) was performed by random number assignment from random.org, as part of the project's Expert System (ES) software 10 and was implemented by one staff member at the end of the baseline visit. Sixty-two children remained at the end of the trial (visit 4 at 9 months, n=33 treatment; n=29 control) when the primary outcome measures of BPs, body composition, and BMI were assessed; body composition and BMI were further assessed at visit 5 at 15 months (end of maintenance observation, n=59). This sample size allows for detection of medium-to-large effect sizes of 0.61–0.72 for continuous measures, with a power of 80% and a critical value of 0.05 (two-sided). 13
PacDASH Study Measurements and Materials by Time (Months) and Visit
Weight and height.
Welcome letter, DASH handout, DASH of Aloha book, Farmers Market locations, and physical activity map.
Diet and PA assessment with targeted behavioral messages.
Use of the environment: Farmers Market/school/home.
1% milk or less, whole grains, and less sedentary time.
PacDASH, Pacific Kids Dietary Approaches to Stop Hypertension (DASH) for Health; BP, blood pressure; PA, physical activity; PacTrac2, Pacific Tracker version 2; ES, Expert System.
Study visits lasted an average of 2.5 hours. Parents completed questionnaires and the child had measurements taken by staff for BP, height, weight, circumferences, and skin folds. Parents also completed children's 2-day food and PA logs before the visit, which were reviewed by staff with parent and child at the visit, and the computerized ES assessment was done with the parent and child. The study is a registered clinical trial (ClinicalTrials.gov: NCT00905411).
Trial Materials for Treatment Group
The trial consisted of a baseline visit with study informational packet and child and parent ES recommendation/reports and two subsequent visits, a physician ES recommendation/report, three stage-based mailings, and three support behavior mailings. At baseline, children in the treatment group received a welcome letter, handout on recommended (DASH) eating pattern, DASH of Aloha cook book, Farmers Market locations, and a PA location/map in the study informational packet (Table 1). After visit 1 (baseline), tailored information was generated from the study-designed computerized ES, which provided a message according to stage of readiness to change and self-efficacy for FV consumption and PA generated from questions asked of the child. 9 The message was given to the child and parent by the study team and subsequently by a KP health provider at the child's annual health visit. Participating health providers received a 1-hour study overview and training on stage-based counseling and the PacDASH protocol. 10
The ES 18 was capable of considering responses to questions, reasoning, and recommending a course of action for improving diet and PA. The ES determined the appropriate stage of change based on four to six questions (two to three questions for each domain) and current levels of intake and activity; the ES determined self-efficacy with one question for PA and one for FV consumption addressing the belief that the individual can do the target behavior. 8 The ES follows the transtheoretical model, 14 which considers that tailoring the treatment to match the stage produces optimal progress. 15 In general, persuasive texts used in the earlier stages involve thinking and feeling. Action-related or behavioral texts are used to a greater extent in the later stages.
The information was intended to improve child dietary intake (emphasizing FV intake), increase PA level, and prevent excess weight gain, body fat, and high BP. Child and parent were also mailed activities based on the stage (of readiness to change) determined at baseline, to create an environment to support these behaviors (Farmers Market/school/home) at 2, 5, and 8 months. They were mailed material to support the treatment behaviors (on 1% or nonfat milk, whole grains, and decreasing sedentary behavior) at 3, 6, and 9 months.
Trial Materials for Control Group
Child and parent in the control group received a welcome letter and attention control mailings on unrelated health topics, such as importance of hand washing, sun protection, and dental hygiene, at 2, 5, and 8 months. At the end of the maintenance measure of the study (15 months), children in the control group received the full package of materials received by the treatment group.
Study Measurements
Child ethnicity
The blended ethnicity (BLEND) method was used at baseline to capture proportion of mixed ethnicity by using the ethnicity of both biological parents to define child ethnicity. 16 Children's ethnicities were then classified as white, Filipino or other Asian, Native Hawaiian or other Pacific Islander (NHPI), or other ethnicity.
Body size and composition measurements
Height was measured on a wall-mounted stadiometer (model PE-AIM-101; Perspective Enterprises, Portage, MI) and weight on a digital floor scale (seca 876; seca Deutschland, Hamburg, Germany), according to standard methods. 17 Skinfold thicknesses (triceps, biceps, iliac, calf, and subscapular) were taken by skinfold caliper (Lange, Ann Arbor, MI). Anthropometrists were standardized by the principal investigator; correlations for inter- and intraobserver variability were acceptable (>80%). 17 BMI percentiles and z-scores were determined according to CDC definition, 12 and these were used to determine healthy weight (5≤BMI percentile <85), overweight (85≤BMI percentile <95), and obese (BMI percentile ≥95) outcome variables. Body size and composition measurements were assessed at all five visits (baseline and 3, 6, 9, and 15 months).
Blood pressure measurements
BP measurements were taken by trained clinic staff using a manual aneroid manometer and stethoscope using appropriate cuff size. Systolic and diastolic measurements were taken in duplicate, with the child at rest for at least 5 minutes with legs uncrossed. Percentile of diastolic and systolic measurements for age, sex, and height was determined by comparison to reference data from the National High Blood Pressure Education Report on the Diagnosis, Evaluation and Treatment of High Blood Pressure in Children and Adolescents 18 and used as outcome variables given that both are used to determine HTN. BP measures were assessed at the first 4 visits (baseline and 3, 6 and 9 months), until the end of the trial period.
Food and activity logs
The food and activity log was developed by the principal investigator, modified from food and activity records previously used in the Female Adolescent Maturation study. 19 A surrogate (parent) supervised and led the completion of the log, with active participation by the child, as instructed on the log. Staff was trained to guide parents in the completion of logs and to probe them for clarification upon receipt of the log. Information was collected on the log about the food and beverages consumed and activities performed the Friday and Saturday preceding each visit; logs were analyzed with the Pacific Tracker (version 2; PacTrac2) software. 8 Weighted averages of foods and activities were calculated across the 2 days of records, where a weight of 5 was given to Friday (as one of five weekdays) and a weight of 2 was given to Saturday (as one of two weekend days).
The Healthy Eating Index 2005 (HEI) was calculated from the first day's diet, according to methods developed by the Center for Nutrition Policy and Promotion. 20 Twelve individual components of HEI (HEI 1–12) were calculated: HEI1: total fruit, including 100% juice; HEI 2: whole fruit, not including juice; HEI 3: total vegetables; HEI 4: dark green and orange vegetables; HEI 5: total grain; HEI 6: whole grain; HEI 7: milk; HEI 8: meat and beans; HEI 9: oils; HEI 10: saturated fat; HEI 11: sodium; and HEI 12: calories from solid fats, alcoholic beverages, and added sugars. The calculation of whether the child achieved the recommended level of FV intake (five or more servings of FV per day) and PA (60 or more minutes a day of MVPA per day) was based on the weighted average levels. Two-day food and activity logs were collected for all five visits (baseline and 3, 6, 9, and 15 months).
Statistical Analysis
Statistical analyses were completed using Statistical Analysis System (SAS) for Windows software (version 9.3; SAS Institute Inc., Cary, NC). Baseline participant characteristics were compared by either the chi-square test or t-test. Mixed regression models21,22 of the outcome variables were used to examine the trial effects while controlling for the correlation structure of the repeated measures and adjusting for child's sex, age, and ethnicity to account for possible differences in the composition of the children attending each visit. However, the results (not presented) were similar when not adjusted for these demographic factors.
To test our primary hypothesis that PacDASH intervention would result in changes in body size and BP through changes in FV intake and PA level, we compared the group differences at the last measurement (end of the trial at 9 months for BP and end of maintenance at 15 months for all other outcomes). We also tested for differences between groups at any visit, in a global test to determine when a possible change occurred. Both tests were assessed by contrasts within the mixed model. The test of treatment effect was a test for the interaction between randomization condition and time, parameterized as indicator variables for 3, 6, 9, and 15 months for all outcome variables, except for BP, of which the interaction was parameterized as indicator variables for 3, 6, and 9 months. The p values for the primary test of the hypothesis were given for tests for the interaction between randomization group and the endpoint time indicator against zero (a test with 1 degree of freedom [df]), whereas the p values for the global test were given for the interaction between randomization group and the four time-point indicators (4 df) or three time-point indicators for BP (3 df).
Mixed linear regression models were used for the continuous outcomes of the diastolic (DBP) and systolic BP (SBP) percentile outcomes, BMI percentile and z-score, and the continuous behavioral measures for daily FV consumption and minutes per day of PA. The assumptions of the model were met. An F test for interaction was used to test for trial efficacy. Mixed logistic regression models were used for the dichotomous outcomes of BMI category (healthy vs. overweight and obese) as well as whether the child met national recommendations for FV consumption and moderate and/or vigorous types of PAs; predicted probabilities were computed and a score test for interaction was used to test trial efficacy.
To test the mediating effect of diet or PA on the treatment effect of the outcomes, Baron and Kenny's 23 criteria for the establishment of mediation were followed. A series of mixed linear regression models were conducted to test whether detected effects of the treatment on outcomes were mediated by achieving the recommended level of FV consumption or of MVPA. For mediation to be inferred, the association originally found between the predictor (represented by the interaction between randomization condition and time) and the outcome variables had to be decreased or eliminated after the mediators (diet or PA) were added into the model. 22
All analyses were initially based on all available data points and then rerun on an at-risk group, defined either as those not meeting national recommendations at baseline for PA (60 minutes daily of moderate or vigorous types of activities) or FV intake (five servings daily), or as overweight or obese.
Results
Participant Characteristics at Baseline
Children were drawn from 826 children assessed in the electronic database for eligibility from KP; 741 children were excluded for not meeting inclusion criteria (n=215), declining participation (n=372), and not attending their scheduled appointments or not able to be contacted (n=154). The majority of the 85 participants were female (62%). Mean age was approximately 7 years (Table 2). Ethnicity was largely Asian (44%) or NHPI (28%). The majority of parents had postsecondary education (71%) and almost half (46%) had an annual household income of US$60,000 or greater. The chi-square test for sex and ethnic distribution and t-tests for child's mean age revealed no significant differences between the two study groups at baseline (Table 2).
Baseline Characteristics, 5–8 Years, PacDASH Study by Randomization Group (n=85)
Blood pressure missing from 2 participants from control group. Percentile according to Novotny and colleagues. 11
HEI: Healthy Eating Index, for 2005 Dietary Guidelines. 12 Only HEI 9 and HEI total score significant.
PacDASH, Pacific Kids Dietary Approaches to Stop Hypertension (DASH) for Health; NHPI, Native Hawaiian or Pacific Islander; Z, z-score; SBP, systolic blood pressure; DBPPCT, diastolic blood pressure percentile; MVPA, moderate or vigorous physical activity; min/day, minutes per day; FV, fruit and vegetable; SD, standard deviation.
Body Size and Composition at Baseline (n=85)
Mean BMI z-score (Z) was 1.3±0.7 standard deviations (SDs; Table 2). Mean BMI percentile among study subjects was 85.9±14.4. Children were classified as 36% healthy (but above the 50th percentile), 26% overweight, and 38% obese, a reflection of the recruitment strategy to target the upper end of the BMI distribution. Total body skinfold thickness (sum of triceps, biceps, iliac, calf, and subscapular skinfold thicknesses) averaged 78.8±31.9 mm. Waist circumference averaged 59.9±6.7 cm. Mean DBP was at the 47th percentile, compared to reference data, 11 and mean SBP was at the 33rd percentile. One child was prehypertensive and 2 children were hypertensive. The chi-square test for BMI category distribution and the t-tests for mean BMI Z, BMI percentile, total body skinfold thickness, waist circumference, and DBP and SBP revealed no significant differences between the two study groups at baseline (Table 2).
Physical Activity and Diet (n=85) at Baseline
Weighted daily average minutes per day of moderate or vigorous types of activities (MVPA) was 179.3±114.7. Daily FV servings averaged at 3.9±2.2. HEI total score (out of 90) averaged at 59.4±10.2. The only significant differences between the two groups were found for HEI total score and HEI 9 (oil consumption), with the treatment group having higher scores (p=0.01; Table 2).
Treatment Effect
There was no significant effect of the PacDASH intervention on change in BMI Z score, SBP, waist circumference, total body fat by skinfolds, PA level, or total HEI score (p>0.05; Table 3) or for BMI category, or for percentage of participants meeting national recommendations of FV intake or MVPA.
Covariate Adjusted Means a of Outcome Variables for the Treatment and Control Group Over Visit Time among All Study Subjects (N=85)
Mixed linear model adjusted for sex, age, and ethnicity.
Global F test; treatment effect at each follow-up visit zero.
Means, last visit.
Variable not measured.
Healthy Eating Index, score from 90. 11
Meet recommendation: 60 minutes moderate/vigorous activities (PAMEET); five servings fruit/vegetables (FVMEET); healthy weight, overweight/obese (BMI category).
DBP, diastolic blood pressure; SBP, systolic blood pressure; FV, fruits and vegetables; MVPA, moderate or vigorous physical activities; HEI, Healthy Eating Index; SE, standard error; N/A, not applicable.
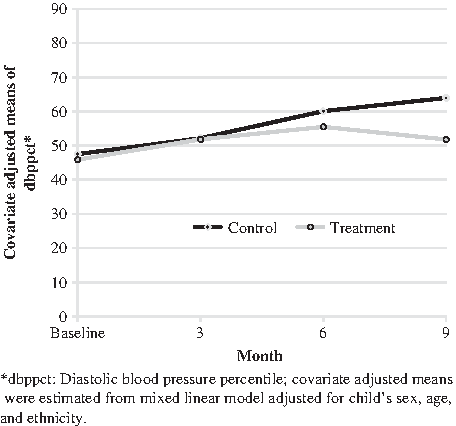
DBP percentile increased over time in both study groups, but to a greater degree in the control group. At 9 months, DBP percentile was 12.2 points lower in the treatment group than the control group (p=0.01; Table 4; Fig. 1). Among the 65 (77%) children who at baseline did not meet national recommendations of 60 minutes a day of MVPA or a minimum of five servings of FV per day (“at-risk”), DBP percentile was lower in the treatment, compared to control, group at 9 months by 21 points, controlling for age, sex, and ethnicity (p<0.001; Table 4). No intervention effect was found among other outcome variables examined in the at-risk group.
Covariate Adjusted Means of DBPPCT From the Models Testing Behavioral Mediation
Adjusted: sex, age, and ethnicity.
Adjusted: sex, age, and ethnicity; 60 min/day of MVPA: 1=yes, 0=no.
Adjusted: sex, age, and ethnicity; five servings/day of FV: 1=yes, 0=no.
A total of 65 participants not meeting the national recommendation of 60 min/day of MVPA and/or five servings/day of FV at baseline.
Global F test that at each follow-up visit, the difference in the means between the two groups is zero.
F test that, at visit 4 (9 months), the mean difference between the two groups is zero.
DBPPCT, diastolic blood pressure percentile; PA, physical activity; FV, fruit and vegetable; MVPA, moderate or vigorous physical activity; SE, standard error.
Behavior
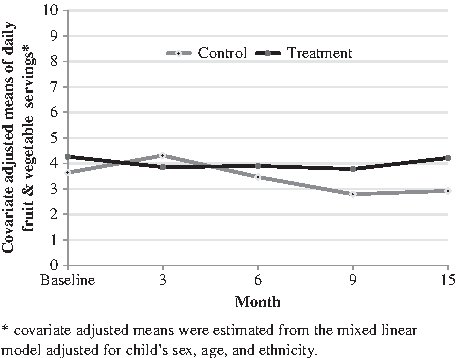
For the intervention group, FV intake remained stable from 3 to 9 months and increased slightly at 15 months. In contrast, there was a decrease in FV intake in the control group from 3 to 15 months. As a result, at 15 months, the mean of FV intake was 1.2 servings higher in the treatment group than the control group (p=0.04; Fig. 2). PA decreased over time in both groups. Whereas PA tended to decrease less in the treatment group, the difference was not significant. Whereas the HEI score was greater at baseline in the treatment group, owing to the oil-intake component of the score, the change in scores was similar between study conditions over time.
Behavioral Mediation of the PacDASH Treatment Effect on Diastolic Blood Pressure Percentile
No mediating effect was found for FV consumption or PA, measured as a continuous variable, on the relationship between the PacDASH treatment and DBP percentile. There was some evidence of a mediating effect for meeting the national recommendations for PA on DBP percentage (Table 4). The difference at 9 months in DBP between groups was reduced by 2 percentage points from 12 to 10 for all participants (n=85) and from 20 to 18 for the 65 at-risk children, controlling for age, sex, and ethnicity. The difference between groups was no longer significant at p=0.05 for the at-risk group.
Missing Data
Because there was attrition of 27% (n=23) of children at 9 months and 31% (n=26) at 15 months, we compared baseline characteristics of children who did and did not provide data at the last visit (9 months for BP or 15 months for anthropometry and behavioral variables). No significant differences were found between children with and without data at 9 months between randomization groups at baseline on child's sex, child's age, parental educational level, family income level, or on meeting national recommendations on PA and FV intake, DBP or SBP percentiles, BMI, or body composition variables. The only difference between groups was that relatively fewer NHPIs returned at 9 months than other children (p=0.03; Fisher's exact test). Baseline characteristics were also generally similar between children with and without data at 15 months. However, relatively fewer NHPIs returned at 15 months also (p=0.005), and the mean age of the children with missing data was older than those with data (p=0.004). As a result, age and ethnicity were controlled in the models to account for the possibly changing composition of children over time.
To further evaluate the effect of the ethnic differences, we reran the analysis for the 61 non-NHPI children; the number of NHPI children (n=24) was too small to allow for separate analysis in this group. The pattern of results was similar, with a lower DBP percentile at 9 months for the treatment group than the control group, by 10 points (p=0.07 at 9 months), a higher level of FV consumption in the treatment group (global F test, p=0.04), and no significant differences for BMI, body composition, SBP, and PA.
Thus, we conclude that bias introduced by missing data points did not affect our conclusions.
Discussion
PacDASH was unique in comparison to other lifestyle interventions for children at risk for obesity by addressing the child, parent, and physician, tailoring FV and PA messages for children according to stage of change and self-efficacy, using a DASH eating approach for young children, including use of local Pacific foods in the diet messages, and addressing obesity prevention as well as treatment (healthy, overweight, and obese children), in addition to including understudied Asian-Pacific populations. The DASH eating pattern is the foundation of dietary guidelines for Americans. 5 Using DASH eating patterns also allows for tailoring with local, cultural foods. Therefore, the PacDASH intervention is fundamentally a healthy behavior intervention that can be used both for prevention and treatment of overweight and obesity. 24 Prevention of overweight and obesity is inherently more desirable than weight loss.
The PacDASH trial did not affect overall diet quality measured by HEI, PA level, body fat, waist circumference, BMI, or SBP change, but the trial did increase FV intake and protect children from increased DBP by the end of the intervention, by 12.2 points. Mediation of this protection by increased PA was demonstrated, overall and among those at behavioral risk.
PA has been shown, in two meta-analyses, in children to lead to small decreases in BP, 25 including DBP. 26 These results are similar to those found in the DASH trials among adults, children, and other ethnic groups.4,5 Also, a decrease in diastolic BP was also found with a gardening intervention with overweight children. 27 Obesity is especially related to DBP, apparently increasing left ventricular mass and wall thickness, which have been associated with adverse heart outcomes in adults. 9
Couch and colleagues' 3-month trial with 3-month follow-up of 57 adolescents also showed decrease in BP percentile with a DASH diet, but in the systolic component. A difference in design was that the adolescent participants were hypertensive at baseline. 4 The Couch trial also increased FV intake (and potassium and magnesium), in addition to decreasing dietary fat intake.
FV intake may improve DBP as a result of an increase in potassium, magnesium, folic acid, and unsaturated fat, as well as a decrease in total fat. 27 PA is also generally thought to improve BP by maintaining or decreasing weight. 28
Although a slowing of the increase in DBP with age in children is likely beneficial for health, there is a paucity of evidence about healthy BP levels for children, and there has been some question in the literature about the accuracy of existing reference values for children. 29 Further, there are no reference values specifically for Asian and NHPI children, and the reference values from the CDC that we used did not include Hawaii or many Asian or Pacific Islanders. 15 Indeed, among our multiethnic population of children who have BMIs in the upper end of the reference distribution, we found that SBP values were low, compared with reference values. More work is needed to understand healthy BP values for ethnically diverse children, especially among understudied Asian, NHPI children.
A key limitation to this study is the small sample size and the loss to follow-up, which may compromise the ability to demonstrate statistical significance of the intervention effect. Twenty-three (27%) of the 85 children did not have a 9-month assessment. This attrition could bias the results, although our sensitivity analysis did not indicate this. Though heterogeneity of physician's style of delivering the tailored information might also affect results, this could not be evaluated given that each physician recruited only a few patients. However, we achieved the aim of the study, which was to develop and test an intervention that could be replicated in the clinical setting of KP. All dietary measures are subject to error; yet, food and activity records or logs are standard methods and have been found to provide reasonable accuracy with instruction and probing by trained staff. 30 Nonetheless, this error of measurement likely limits our ability to demonstrate significance of results.
Our intervention effect would likely be enhanced with additional health professional support to children and parents, with longer-term follow-up of children, and with examination of more children at different levels of obesity and hypertension. The intervention likely would have greater effect on those children above the 99th percentile of BMI for age, which was outside the scope of the present study.
Conclusions
The PacDASH behavioral trial prevented decrease of FV intake and slowed the increase of DBP among 5- to 8-year-old multiethnic children of predominantly Asian and Pacific Islander ancestry. The intervention effect was mediated by PA, overall and among behaviorally at-risk children.
Footnotes
Author Disclosure Statement
No competing financial interests exist.