
Abstract
Abstract
Background:
This is a retrospective cohort study to evaluate a novel group medical visit (GMV) program using an empowerment curriculum as treatment for pediatric obesity in a federally qualified community health center.
Methods:
Biometric and self-reported data were reviewed from 417 overweight or obese children ages 5–18 attending the pediatric obesity empowerment model GMV program (POEM-GMV) at least twice during a 3-year period. Variables were evaluated using paired means t-test. Pearson's correlation test was used to evaluate variables and the BMI z-score. Subanalysis by gender was performed.
Results:
The average participant was 10.48 ± 2.53 years old and participated for 301 ± 287 days. BMI z-score reduced from 2.99 ± 0.96 to 2.88 ± 0.88 (p < 0.0001). Overall, 62.6% of participants had improved weight outcome. Statistically significant improvement was noted in stress, exercise, beverage consumption, fast food intake, television viewing, and bedtime. Stress and beverage consumption had the highest correlation with BMI z-score. By sex, 71.4% of boys (n = 196; p < 0.0001) and 54.8% (n = 221; p < 0.014) of girls realized a reduction in BMI z-score, 61.2% (p < 0.001) of boys and 47.1% (p = 0.097) of girls had a reduction in their percent overweight.
Conclusions:
POEM-GMV may be a useful approach in the treatment of pediatric obesity in an underserved community. There were statistically significantly improved outcomes in obesity, especially for boys. Significant improvement was observed in many lifestyle factors associated with obesity. Weight loss most closely correlated with reduced stress levels and sugary beverage consumption. Additional studies are needed to further evaluate the efficacy of POEM-GMV.
Introduction
The motivation for this study is to evaluate the pediatric obesity empowerment model group medical visit (POEM-GMV) program being used to treat obesity and overweight at a federally qualified community health center (CHC). From the beginning of the program in 2001, there has been anecdotal and visible evidence that this model is a viable and effective treatment program for obesity in children. There are not many programs like this, which are as large, or have been as sustaining in poor communities. This article presents a 3-year retrospective cohort of consecutive children who participated in the POEM-GMV program with evaluation to answer the question of efficacy. Though the primary outcome is weight change, these data can also be seen as a viability study. Subgroup analysis is provided to give hints as to behaviors and sex differences that emerged as significant. These data can be used to help guide future directions for improvement and evaluation of treatment for children with obesity in poor communities.
Obesity in the pediatric population has been defined by the CDC as a “BMI at or above the 95th percentile for children of the same age and sex” based on the 2000 CDC Growth Charts. 1 Obesity is a known risk factor for many health problems, including type II diabetes and cardiovascular disease. Between 1999 and 2010, the overall prevalence of obesity in children and adolescents has remained steady at 16.9%, 2 and the Healthy People 2020 state a goal of reducing the overall prevalence to 14.5% by 2020. 3 Obesity in lower-income preschool children (2- to 4-year-olds) had been increasing over the period of this study, with 1 in 7 found to be obese. Hispanic children are over-represented in this group: 18.5% of Latino children are obese compared to 14.6% of all low-income children. 4 In addition, Latino male youths may be particularly prone to obesity-related morbidities, making this population more vulnerable. 5
The Alternative Medicine Program at Greater Lawrence Family Health Center (GLFHC) serves a poor, predominantly Latino community. The poverty level in this community is twice that of the national average, with 28.6% living below the poverty line, 6 and pediatric obesity is a significant issue with 46.6% of students in grades 1, 4, 7, or 10 in Lawrence classified as overweight or obese. 7 The POEM-GMV is a novel approach to address the pediatric obesity crisis in our community. It is based on the hypothesis that, particularly in a disadvantaged population, empowering participants, rather than simply educating, will lead to healthier behaviors and a reduction in weight. This empowerment and self-direction is facilitated through the use of a group model that provides support and features participatory decision making. The primary aim of this retrospective cohort study is to assess the impact of the POEM-GMV intervention on the weight of participants. The secondary aims of this study include evaluating the relationship of sex, lifestyle, social, biometric, and empowerment factors to change in weight.
Literature Review
Pediatric obesity is a growing problem in the United States. An estimated 16.9% of children between the ages of 2 and 19 are obese. 8 Definitions of pediatric obesity differ, but include either being above the 95th percentile for BMI (weight for height), having a weight for height z-score above 2, or being 120% of ideal weight for height. As children age, sedentary lifestyle, 9 decreased physical activity, 10 increased consumption of sugar-sweetened beverages, 11 and television (TV) watching >8 hours weekly at age 3 12 are associated with an increased risk of childhood obesity. Hispanic and African American children are especially vulnerable to developing obesity because of the higher prevalence of known early risk factors to developing childhood obesity, including gestational diabetes in the mother, rapid weight gain from birth to age 6 months, lack of exclusive breastfeeding, early introduction of solids, TV in the bedroom at age 4, drinking sugary sweetened beverages at age 2, sleeping less than 12 hours daily at age 2, and fast food consumption at age 3. 13 The associated complications of childhood obesity are numerous. Most troubling, obese children have an increased risk of overall mortality as adults, 14 as well as increased risk of cardiovascular events specifically. 15 In addition to long-term effects, obese children have higher rates of musculoskeletal complications, 16 depression, anger, and fatigue. 17 Treatments for pediatric obesity have showed varying levels of effect, similar to management of adult obesity, but include intensive lifestyle interventions targeting diet, physical activity, counseling, and behavior modifications. Medications and bariatric surgery have a role for morbidly obese adolescents who have failed intensive lifestyle programs. 18
Methods
Intervention
The POEM is based on what we have termed an “empowerment model.” We hypothesize that children who are engaged, not simply educated, in a group setting will have greater self-efficacy, social cohesion, and will have improved health behaviors and increased weight loss. More simply, we define empowerment as “the ability to try new things.” Participatory decision making is a key component of the group visit given that each group will decide what activities and projects they will do to improve their own health. Education on healthier lifestyles is incorporated into the weekly group activities. Participants receive individual physician visits (IPVs) every 4–6 weeks as an opportunity for private evaluation, assessment, and counseling.
The weekly group visits begin with a “check-in” period of approximately 5–20 minutes of open-ended questions and discussion to build trust and community among participants. This is followed by 20–30 minutes of a physician- or staff-led activity where participants learn new skills and try new things. Activities are chosen by participants and vary greatly from week to week. This is followed by 20–30 minutes of work toward an empowerment project, which is a longer-term activity chosen by the participants that can last for several weeks or months until a goal is accomplished. See Table 1 for examples of activities and projects. The goal of each 75-minute session is to build relationships within the group, experience success with new activities, and encourage healthy lifestyle education in a manner that engages and empowers the participants. Children older than 8 years are offered transportation after school and the programs are without their caregivers. Children under 8 years old participated in the same curriculum, but met in a family group with parents or guardians present.
Typical POEM-GMV Activities and Projects Employed 2009–2011
POEM-GMV, pediatric obesity empowerment model group medical visit.
GMV participants have an IPV on a regular basis with one meeting on their first visit and every 4–6 weeks thereafter. At the IPV, the medical assistant assesses height, weight, and a variety of self reported lifestyle metrics. These are then available for review with the clinician during the IPV. The IPV is brief (5–10 minutes), where motivational techniques are used and individual counseling occurs. The main questions asked are similar to these: “How do you think you are doing?” and “What do you think you can do to be healthier or happier?” This line of questioning is designed to elicit a specific lifestyle change suggested by the participant. These lifestyle change goals are noted by the clinician to be re-evaluated at subsequent IPVs.
Patients
Subjects were determined by a search of our electronic medical records (EMRs) for patients with visits to the POEM-GMV program in the 3-year study period. Participants were referred to the program by their primary care providers, and needed to be existing patients from GLFHC. Inclusion criteria for the study group included being overweight (in the 85th or higher percentile for their age 19 ), age between 5 and 18 years old at the start and completion of the study period, and at least two IPVs in the program.
Measures
The available EMR data variables were height, weight, age, sex, date of IPV, and duration in POEM-GMV. Additional data were self-reported and part of the standard-of-care questions used for the program. Though not designed to answer a specific research question, these additional data could be roughly broken down into lifestyle, social, and empowerment factors. Lifestyle factors included: hours of TV watched per week; number of sugary beverages/juice consumed a day; days with rigorous exercise per week; number of days a week with three meals a day; restaurant meals per week; junk food servings per day; servings of fruits and vegetables per day; bedtime; and time of last food at night. Social factors included: number of family members considered overweight; number of people in household; perceived happiness; and perceived stress.
The final grouping of data comes from questions our providers had found helpful; based on experience in the community, we call these “empowerment factors.” Empowerment factors were assessed by asking these questions: “Have you changed anything in your life this month?”; “Have you tried any new foods this month?”; “Have you made any new friends this month?”; “How many people really know you well?”; “How many people like you the way you are?”; and “How often do you feel like a part of this group?” Self-reported happiness, stress, and many of the empowerment factors were rated on a 3-point scale (none of the time = 0; some of the time = 1; and all of the time = 2).
Weight was assessed and will be presented in three ways. BMI was used to look for absolute changes in weight relative to height. Percent overweight (%OW) was used as a normalized value to take into account expected weight and height for age and gender. It is calculated as [(current weight – 85th percentile predicted weight for age, gender, height)/current weight]. BMI z-scores were used to compare BMI changes in the study group to the expected BMI changes of the population at large. These “control group” comparison z-scores were based on large national data sets and were calculated using the World Health Organization algorithm. 20
Data Collection
The data for this study were extracted from the EMRs of consecutive pediatric patients who were referred to POEM-GMV for treatment of obesity by a physician at GLFHC. EMR templates were developed and data recorded for the 3 years between September 1, 2008 and September 1, 2011. After September 2011, there was a change to a new EMR system, which did not allow for further data extraction. Preceding September 2008, there was no EMR template from which to extract data.
Statistical Analyses
All data were reported as baseline and final measurements using the most appropriate units. In some instances, percentages were used in place of absolute values. These variables were then compared and noted for change. A two-tailed paired t-test of means was applied for the biometric data as well as the lifestyle, social, and empowerment factors. A p value of less than 0.05 was considered statistically significant.
Regression analysis was performed on continuous data variables for correlation with BMI z-score, with an absolute r value greater than 0.2 considered significant and reported. Based on our pilot study data (not shown), to achieve a power of 0.90 and a significance of 0.05 for 5% weight change in BMI, the number of subjects required was n = 151. Through the pilot study, it was predicted that boys and girls groups may have significant differences in outcome and reported measures. Therefore, a subanalysis for these same factors mentioned above based on sex was conducted.
Ethics
The University of Massachusetts Medical School Institutional Review Board deemed this study to be exempt.
Results
There were 687 participants referred to POEM-GMV; of these, 584 visited the program at least one time. A total of 417 children came to at least two IPVs during the 3-year study period and are evaluated below as the study group (see Fig. 1).
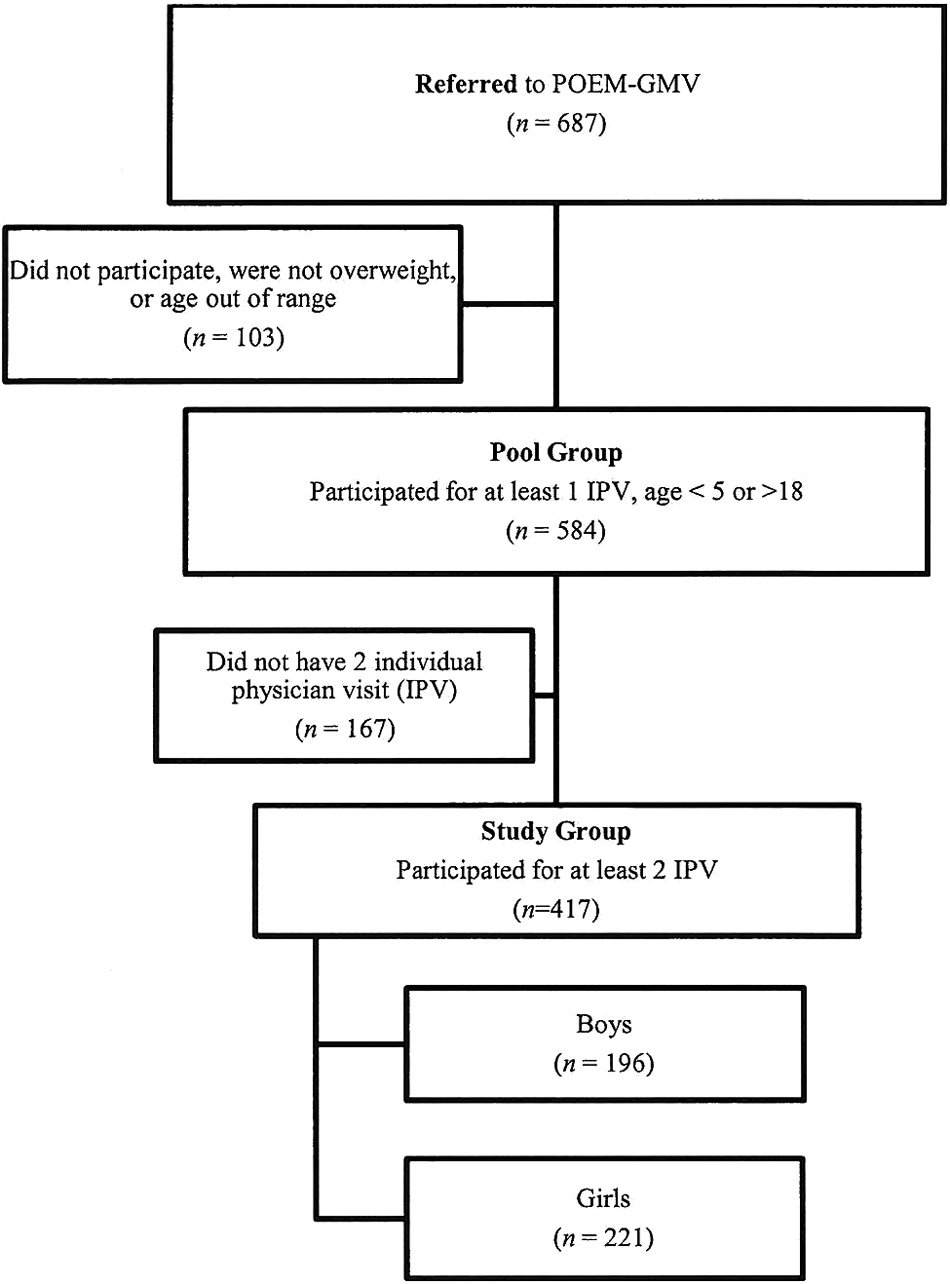
Flowchart for study enrollment.
Study Group
Average age at the first visit was 10.48 ± 2.53 years. Overall, 53.0% of participants were female. The average time in the program was 301 ± 278 days. The average BMI at the start of the program was 27.6 ± 5.48 and at the conclusion was 28.4 ± 5.66 (p < 0.0001), where 143 (34.4%) participants had reduction of their BMI. Average BMI z-score at the start of the program was 2.99 ± 0.96 and at the conclusion was 2.88 ± 0.88 (p < 0.0001), where 62.6% of participants had improved weight outcome. Average %OW at the start of the program was 25.3%OW and at the end was 24.9%OW, where 53.7% of participants had improved weight. The 0.4%OW reduction approached, but did not achieve, statistical significance (p = 0.06).
Program effects on lifestyle, social, and empowerment factors for this group can be seen in Table 2. Lifestyle factors with a statistically significant change (p < 0.05) over the study period were: decreases in beverage consumption; fast food; junk food; and TV hours viewed per week; increases in exercise; and earlier time of sleep. The only social factor with a statistically significant change was a decrease in perceived stress. Empowerment factors associated with a significant change were: increases in perceived ability to make changes in life; feeling part of the group; decreases in number of new friends; and healthy changes.
Study Group Results: Pre and Post Mean Variable Comparison
Paired t-test, comparing included versus excluded subjects.
None of the time = 0, some of the time = 1, all of the time = 2.
Never = 0, once = 1, more than once = 2.
Yes = 1, no = 0.
Regression Analyses
No factors attained an r value >0.2. The factors with the strongest correlation with weight gain using the positive change in BMI z-score were: change in stress level (r = 0.193); change in beverage consumption (r = 0.190); and change in junk food consumption (r = 0.158).
Subanalysis by Gender
There were 196 boy and 221 girl participants. Boys had an initial BMI of 27.84 ± 4.87 and final BMI of 28.47 ± 5.37 (p < 0.0001), an initial BMI z-score of 3.21 ±0.97 and final BMI z-score of 3.02 ± 0.93 (p < 0.0001), and an initial %OW of 26.79% ±10.64 and a final %OW of 25.65% ±11.92 (p < 0.001). Girls had an initial BMI of 27.4 ± 5.97 and final BMI of 28.32 ± 5.91 (p < 0.0001), an initial BMI z-score of 2.79 ± 0.91 and final BMI z-score of 2.75 ± 0.83 (p = 0.014), and an initial %OW of 24.00% ±11.54 and a final %OW of 24.27% ±11.74 (p = 0.097). By the end of the study period, 71.4% of boys and 54.8% of girls realized a reduction in BMI z-score, 61.2% of boys and 47.1% of girls had a reduction in %OW, and 39.8% of boys and 32.1% of girls had a reduction in absolute BMI (Fig. 2).
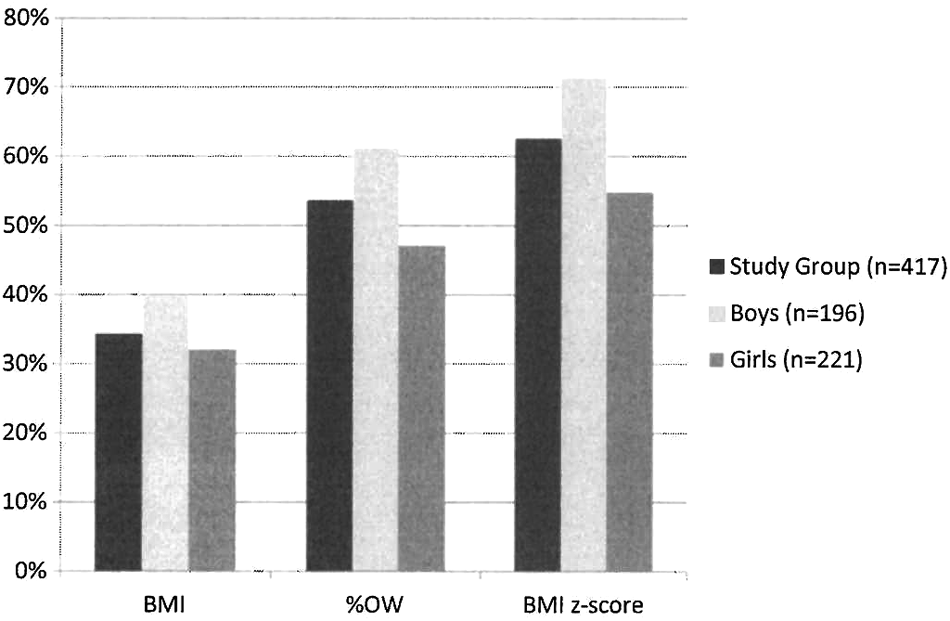
Percent of POEM-GMV participants who lost weight comparing absolute (BMI), normalized (%OW), and comparative measures (BMI z-score). POEM-GMV, pediatric obesity empowerment model group medical visit; %OW, percent overweight.
Regression analysis by sex found only two positively correlated variables (r > 0.2), with BMI z-score. They were change in stress r = 0.28 and change in beverage consumption (r = 0.23) in the boy groups. No strong correlations with BMI z-score were observed in girls for stress (r = 0.13) or beverage consumption (r = −0.05). Boys and girls started the program with similar levels of stress, with average scores of 0.76 ± 0.60 and 0.78 ± 0.65, respectively. Boys' scores reduced by 35% to 0.49 ± 0.59 (p < 0.001) and girls' scores reduced by 13% to 0.66 ± 0.60 (p = 0.029). Girls drank 2.13 ± 1.74 beverages per day at the start and only 1.45 ± 1.14 (p < 0.0001) sugary beverages at the end, compared to boys who drank 2.46 ± 1.86 beverages per day at the start and only 1.78 ± 1.42 (p < 0.0001) sugary beverages at the end.
We evaluated the change in height of the boys and the girls, given that it was proposed that the groups might grow at different rates. Boys grew, on average, 2.18 inches over the course of the study period, compared to girls who grew 1.64 inches. This is a significant difference between groups, but we found that height change had no correlation and was not a statistically significant factor in relation to BMI, %OW, or BMI z-score in either group. There were no other variables that had an r value >0.2 for the boys group and no variables with significant correlation for the girls.
Discussion
Empowerment theory is a social theory that recognizes the disenfranchisement of the poor 21 as an independent risk factor for excess mortality 22 and seeks to engage participants in the decision-making processes regarding their health choices. The desired result is increased healthy behaviors, improved health outcomes, and a reduction in health disparities in the community.23,24
Empowerment theory is a key element in the GMVs at GLFHC. The first GMVs at GLFHC were in 1997 for adults with diabetes. These initial groups were designed for the treatment of loneliness, which was later documented as a serious problem in our community in terms of emergency room utilization and cost. 25 These GMVs demonstrated that not only did participants have less depression and loneliness, but they also lost weight and had better glycemic control.26,27 This model was thus seen as a complementary delivery method and treatment for those with diabetes and heart disease.
There is a growing body of evidence of success using GMVs, particularly in treating type 1 diabetes and asthma in children.28–31 They can be an efficient option for physician-limited environments where CHCs are often located. 32 The GMV model that we employ most closely resembles the “drop-in group medical appointment” model owing to the participants' ability to “drop-in” to meetings at their discretion. One big difference, however, in the POEM-GMV is the continuity of participant, projects, and participation, which allows for individual cohesion in addition to IPVs at each session.
The POEM-GMV is a novel empowerment-based approach to the treatment of pediatric obesity. Empowerment models have shown higher rates of childhood vaccination, improved water sanitation techniques, and improvement in cardiovascular risk factors compared to programs with traditional vertical, nonparticipatory interventions. 33 However, empowerment models up until this point have not yet been studied in addressing pediatric obesity.
In children, psychosocial stress is associated with increased obesity, 34 likely related to chronic upregulation of the hypothalamic–pituitary–adrenal axis. 35 Pediatric obesity itself is associated with increased stigmatization, which causes stress.36,37 This notion is supported by our findings where boys had the highest stress reduction and most improved outcomes. Perhaps this is the most likely mechanism for the changes noted.
Part of the success of empowerment-based models can be attributed to social support theory, which demonstrates that social networks can help mediate social stressors and result in improvements in health behaviors. 38 In adults, social support approaches have shown improved outcomes for weight loss. 39 It is not surprising then that, in this study, stress reduction was strongly associated with weight loss, particularly in boys. There was significant reduction in the %OW and BMI z-score, with the only modifiable factors that correlated with weight loss being decreased sugary beverage, junk food consumption, and self-perceived stress. The combination of stress and sugary beverages as factors associated with weight change is consistent with the current literature. 40
Curiously, the emphasis of our program is not on reduction in sugary beverage consumption, but on empowerment through trying new things and learning how to build relationships. In this study, we measured empowerment by how often participants tried new things, and though this measure improved dramatically, empowerment itself was not significantly associated with weight loss. Certainly, being empowered may be a key factor in making real-life changes, but the results of this study do not support this using our surrogate variables for empowerment.
Another interesting finding was the difference in outcome between boys and girls groups. This was similar to results in our pilot study, although not commonly observed in the literature given that girls typically lose more weight than boys in meta-analyses of pediatric weight loss interventions.41,42 In our subanalysis, a reduction in stress and decreased consumption of sugary beverages was associated with the largest difference in outcome between the two sexes. This study provides further support that reducing stress in pediatric populations results in greater weight outcomes. These results support the initial hypothesis that the POEM-GMV may be effective in disadvantaged groups. The mechanism is certainly unclear as to any specific factor other than stress and sugary beverages. Perhaps it is the sum of all parts with the utilization of participatory group decision making to increase social cohesion. This may provide a link to help reduce stress and, ultimately, improve healthy behaviors.
There are likely many hypotheses for the differences in stress levels and weight change noted between the boys and girls that we can surmise based on common sense and clinical experience. The most likely, however, is that because each group chooses its own activities, there can be a large variety of experiences and exposures to healthy lifestyles from group to group. Though not a rule, one observed difference between boys and girls groups was the nature of the activities selected. Boy groups were far more likely to choose sports or rigorous exercise as their activity each week. Girls had a higher propensity to do public service programs or the arts, such as theater. Though girl groups did exercise at times, they generally leaned away from competition, and the exercises of choice were usually yoga or dancing. This difference in activities based on group sex has been subsequently addressed in our current programming by hiring male and female exercise instructors to do a mandatory 15 minutes of exercise with each group regardless of sex at every visit.
Future research is needed to confirm these findings of weight reduction and evaluate the findings of sex differences in outcome. Specifically, a four-arm study comparing a control group, weekly exercise group, weekly exercise group with individual physician visits, and weekly POEM group would help clarify efficacy. In these studies, it would also be beneficial to use more standard measures other than self-report. Short form questionnaires about stress, dietary diaries, and follow-up participation data would be particularly useful. These measures would help quantify and verify the associations found in our data with beverage consumption, stress, and other lifestyle factors.
Limitations
This project is not a randomized, controlled trial and thus selection bias may be present. There is no control group to control for confounding factors that may have occurred outside the scope of this program. This limits our ability to report with confidence our findings given that the group was, in many ways, self (or parent) selected for participation through doctor referrals. There was also a lot of variation in participation rates owing to the nature of the population we serve in our CHC. This may have created bias toward inclusion of children from more-stable families. Given that many of the lifestyle, social, and empowerment factors are self-reported, they are particularly subject to bias. Another limitation is that the activities varied significantly from group to group (i.e., while one group was actively exercising or gardening, another was doing more-sedentary work, such as writing a book or making a movie). Additionally, this study was conducted in a poor, predominantly Latino community. Therefore, it is not clear whether these results would translate similarly to other communities with differing demographics.
Conclusions
The POEM-GMV may have a role in treatment for pediatric obesity in federally qualified CHCs in underserved communities. Weight change in this program was statistically significantly overall using BMI z-scores and %OW, particularly in the treatment of obesity in boys (p < 0.001). There was statistically significant improvement in many self-reported lifestyle, social, and empowerment factors, such as exercise, sugary beverage consumption, hour of sleep, hours of TV viewed, how often participants try new things, and stress. The strongest correlation with weight improvement was observed with stress and beverage consumption in boys.
Footnotes
Acknowledgments
This publication was made possible by a grant from the New Balance Foundation. The authors are also grateful to the participants of the POEM-GMV program, their parents, and the staff of GLFHC. Many summer intern students from Tufts University School of Medicine also contributed to this project. In memory of Evan Dube for his random acts of kindness.
Author Disclosure Statement
No competing financial interests exist.