
Abstract
Abstract
Introduction:
Although breastfeeding is associated with improving numerous health outcomes for the child, its role in reducing childhood obesity is contested. Despite this controversy, both the CDC and the US Department of Health and Human Services promote breastfeeding as one of the strategies for reducing childhood obesity. Rural Appalachia has one of the highest rates of childhood obesity and low rates of breastfeeding, compared to rest of the nation. The aim of this study was to examine the association between breastfeeding and childhood obesity at 11 years in the rural Appalachian state of West Virginia (WV).
Methods:
The study used linked data from two cross-sectional data sets to examine this relationship longitudinally in fifth-grade WV children. The main outcome variable was BMI adjusted percent (BMI%) and the main exposure was defined as occurrence of breastfeeding. Mean BMI% of children who were not breastfed was significantly higher, compared to children who were breastfed.
Results:
The result of the multiple regression analysis showed that breastfeeding significantly predicted BMI% of children after controlling for maternal education, health insurance, family history of hypercholesterolemia and diabetes, child's asthma status, and birth weight of the infant.
Conclusions:
Our results are consistent with other studies that have shown a significant, but small, inverse association between breastfeeding and childhood obesity. Findings from this study suggest the need to improve breastfeeding rates in the rural Appalachian state of WV as one of the potential strategies to prevent obesity during childhood and adolescence.
Introduction
In the United States, approximately one third of children and adolescents ages 2–19 are overweight or obese. 1 Obesity prevalence is higher in rural regions of the United States, compared to urban areas. 2 West Virginia (WV), a predominantly rural Appalachian state, has one of the highest rates of obesity in the nation.3,4 Childhood obesity has been linked to several health conditions, such as high blood pressure and cholesterol, type 2 diabetes (T2D), psychosocial problems, and an increased likelihood of tracking from childhood into adulthood. 5 The alarmingly high rates of childhood obesity, and the numerous health risks associated with it, marks this as one of the most important public health concerns and challenges. 6
Whereas several strategies have been recommended to reduce obesity, the CDC and the US Department of Health and Human Services promote breastfeeding as an early strategy for reducing later childhood obesity. 7 Recent research suggests that breastfeeding significantly predicts positive health outcomes for both the mother and the child, including reducing childhood obesity.8–10 Two recent meta-analyses found a 15% decrease (adjusted odds ratio [AOR]=0.85; 95% confidence interval [CI], 0.74–0.99) and a 22% decrease (AOR=0.78; 95% CI, 0.74–0.81) in the odds of childhood overweight and obesity comparing breastfed with nonbreastfed infants.11,12 Some individual studies have demonstrated an even higher relative risk reduction (ranging from 25% to 35%) in childhood obesity comparing children who were breastfed versus not breastfed.13,14 However, the association between breastfeeding and obesity is inconsistent across studies.11–17 Some studies have found this association only with overweight (BMI between 85th and 94th percentile) children, but not with obese (≥95th percentile) children, 15 whereas other studies have shown no association between breastfeeding and childhood obesity.16,17
Regardless of the link between childhood obesity and breastfeeding, current guidelines by the American Academy of Pediatrics suggest 6 months of exclusive breastfeeding to achieve the best possible health outcomes for the child. 18 However, data from the 2011 National Immunization Survey suggest that only 18.8% of mothers in the United States and 12.2% of mothers in WV exclusively breastfeed during the first 6 months. The percentage of mothers who initiate breastfeeding postpartum is also much lower in WV (59.3%), compared to the national average of 79.2%.19,20 Lower breastfeeding rates, along with higher obesity rates, are similarly found throughout rural Appalachia. 21
Given lower breastfeeding rates and higher obesity rates, as compared to the national average, it is important to examine the association between childhood obesity and breastfeeding in the rural Appalachian state of WV. Specifically, the aim of this study was to examine differences in BMI adjusted percent (BMI%) of fifth-grade WV children who were breastfed versus not breastfed during infancy. This study hypothesized, consistent with research in other regions of the United States, that nonbreastfed children will have higher BMI% compared to their peers.
Methods
The study used data from two projects, the WV Birth Score Project and the Coronary Artery Risk Detection in Appalachian Communities (CARDIAC) Project. The WV Birth Score Project is an infant risk-screening instrument that was initiated in 1985. Trained healthcare professionals collect data on every newborn born in the state of WV within 24–48 hours or preceding discharge, with the goal of identifying infants who are at a high risk of poor health outcomes or mortality in the first year of life in order to provide referrals to primary care management. 22 In this study, data collected on children participating in the Birth Score Project born between January 1999 and October 2002 were merged with data collected by the CARDIAC Project in years 2011–2012. The CARDIAC Project collects data on fifth-grade children in schools across all 55 counties in WV with the goal of identifying children at risk of cardiovascular disease. Further details of the data collection procedure are described elsewhere. 23 The West Virginia University Institutional Review Board approved the study and the merged analysis. The current study linked the two data sets based on the child's identification number and included only those observations where data were available from both projects.
Measures
Dependent variable
The main outcome variable was defined as the BMI% of the children above the ideal BMI for their age and gender. Trained area coordinators, nurses, and health science students measured the children's height and weight using the SECA Road Rod stadiometer (78″/200 cm) and the SECA 840 Personal Digital Scale, respectively (Seca Corp, Hanover, MD). 24 CDC EpiInfo software (v. 3.5) was used to calculate BMI, height, and weight percentiles adjusted for children's age and gender, and BMI z-scores were based on these percentiles. From US CDC 2000 growth charts, 25 children's sex-/age-specific median was calculated and subsequently the percentage difference from median BMI (BMI% 24 ) was calculated using 100*log BMI/median BMI. BMI% has shown to be an effective measure of adiposity change in growing children. 26
Independent variable
Exposure was defined as occurrence of breastfeeding. Information related to breastfeeding was obtained using the CARDIAC questionnaire retrospectively when the child was in fifth grade by parental/caregiver recall. The question stated, “Was your child breastfed?”, and answer options included “yes,” “no,” and “don't know.”
Covariates
Sociodemographics
Sociodemographic variables included maternal and child's age, race/ethnicity/sex of the infant, maternal education, and health insurance status. Maternal age at the time of infant's birth was recoded as a continuous variable. Given that WV's population is predominately white (94%), the race of the infant was self-reported by the mother and was dichotomized as “white” and “other” for this analysis. 27 The sex of the child was recorded at birth. The age of the child at fifth grade was recoded as a continuous variable and was self-reported by parents/caregivers. Maternal education has also been shown to be a strong predictor of a child's weight and also a predictor of a mother's breastfeeding practices. 28 The maternal education at time of birth included the number of years of education received and ranged from 1 to 17. Maternal health insurance at the time of birth was categorized as a binary variable (Medicaid and non-Medicaid). A recent study concluded that key demographic characteristics, such as race and socioeconomic status (SES), play an important role in the mother's decision and duration to breastfeed her child. 29
Family history of risk factors
Parental overweight is a strong predictor of childhood obesity. 30 The study did not have data on parental weight but included family history of diabetes and family history of hypercholesterolemia (HCS), owing to the genetic predisposition of these variables and their association with obesity.31,32
Other infant, maternal, and child characteristics
Also included in the analysis were other potential confounders that have been linked to childhood obesity (outcome only) or both to breastfeeding and childhood obesity, including infant's birth weight in grams, maternal smoking status (yes/no), and child's asthma status (yes/no).11,33 Whereas several studies have suggested that obesity is a risk factor of asthma, 33 others have argued that sedentary lifestyle and physical inactivity in asthmatic individuals could result in increased weight gain. 34 There is also decreased risk of asthma in children who are breastfed versus formula fed. 9 Literature suggests that intent to breastfeed is a strong predictor of actual breastfeeding practices in the postpartum period, and thus this variable was also examined. 35 The variable was binary with the following response options: “breastfeed” and “bottle or both.”
Statistical Analysis
All statistical analysis was conducted in SAS software (version 9.3; SAS Institute Inc., Cary, NC). An independent sample t-test was used to initially determine if there was a statistically significant difference in the unadjusted mean BMI% of WV children who were breastfed during infancy versus those not breastfed, and the magnitude of this association was calculated using Cohen's d effect size. Multiple regression analysis was then used to assess the adjusted relationships after controlling for covariates. Only covariates significant in the Spearman's correlation analysis were used in the multiple regression models. The significant covariates included: infant birth weight in grams; maternal education status as 1–17 years of education; maternal insurance status (Medicaid and non-Medicaid); family history of diabetes (yes/no); family history of HCS (yes/no); child asthma status (yes/no); and intent to breastfeed (breastfeed/both). Covariates that were not significant and were excluded were: maternal age; maternal smoking status; and child's age, race, and gender. We also excluded the intent to breastfeed variable from the full model because of multicollinearity between the intent to breastfeed and actual breastfeeding variables (r=0.64; p<0.0001).
A general linear model was used to test the primary hypothesis in order to adjust for covariates. The regression F statistic was used to determine the overall significance of the regression model and a corresponding p value of ≤0.05 was considered significant. The ability of each independent variable to predict the outcome variable was also assessed for significance at alpha ≤0.05 by examining the parameter estimates and their corresponding t-test values. The squared multiple correlation coefficients, R2 and adjusted R2, were interpreted as the effect size of the regression model. The study also performed the regression analysis with (full model) and without (covariate model) the main predictor variable (i.e., breastfeeding). The change in R2 was then calculated to determine the unique amount of variance shared between breastfeeding and BMI%.
Results
A total of 5929 subjects were available for analysis with the merged data. Fifty-eight percent of newborns in the Birth Score Project had data in the CARDIAC data set in fifth grade. From the Birth Score Project data, 94% infants were categorized as white, and the maternal age at time of delivery was 25.8 years (standard deviation [SD],±5.7). The average birth weight was 3239.9 g (SD,±535.6). Approximately 48% of the women said they intended to breastfeed at birth. Consistent with the Birth Score Project demographics, from the CARDIAC data, 41% of women subsequently said they breastfed their infant. Mean age of children in fifth grade was 11.0 years (SD,±0.5). Nearly 30% children had family history of HCS, 53% had a family history of diabetes, and 16% had asthma. Mean BMI% of fifth graders was 18.7% (SD,±22.7).
Mean BMI% of WV children who were breastfed versus those who were not breastfed was statistically significant (t(5790)=5.54; p<0.0001; d=0.15). Mean BMI% of children who were not breastfed was 20.03% (95% CI, 19.24–20.82) and those who were breastfed were 16.68% (95% CI, 15.81–17.55), and the mean difference was 3.35% (95% CI, 2.16–4.54; Fig. 1).
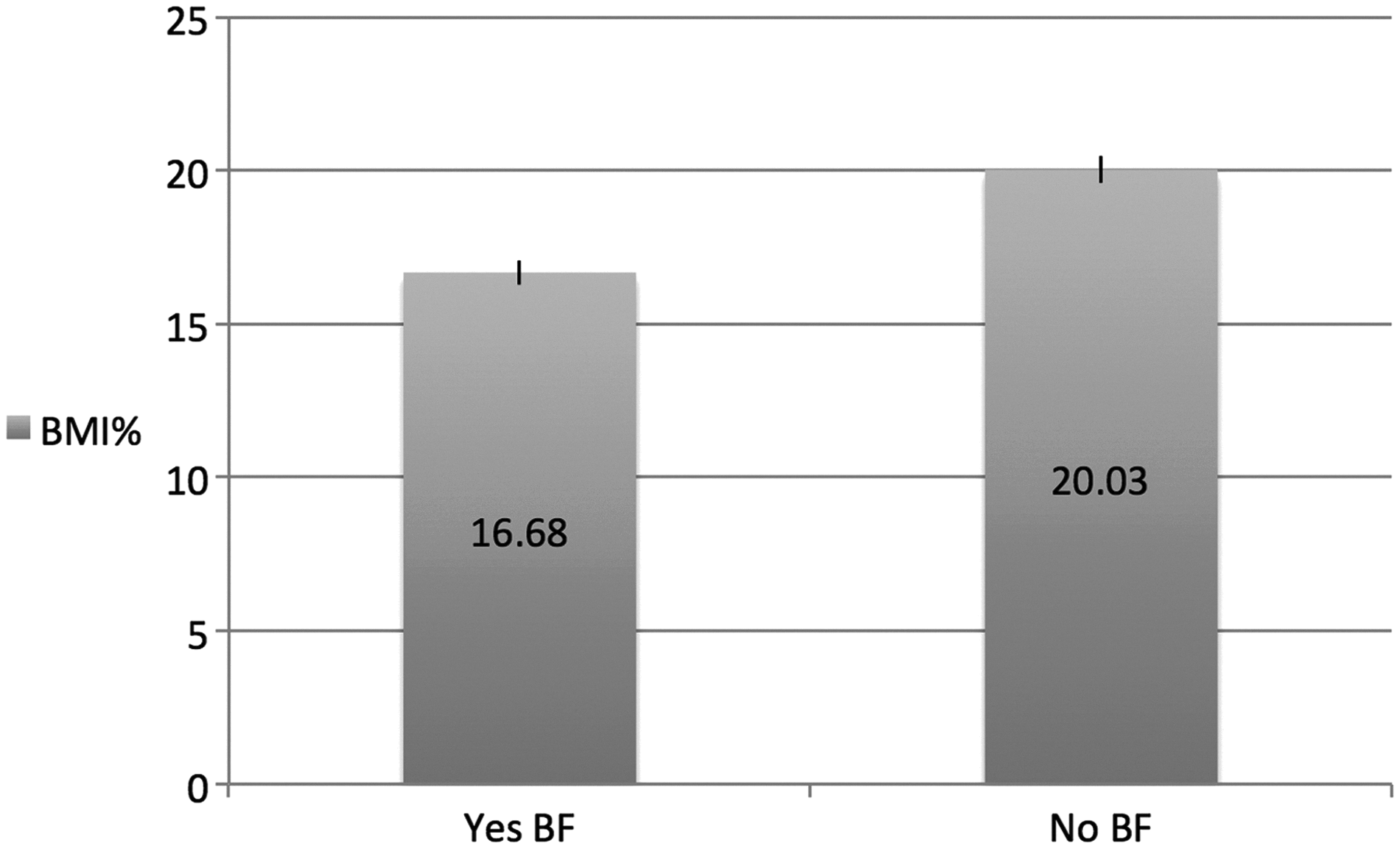
The result of the independent samples t-test showed a statistically significant difference in mean BMI adjusted percent of WV children who were breastfed vs. not breastfed (p<0.0001), using data from 1999 to 2002 from the Birth-Score project merged with 2011–2012 data from the CARDIAC Project (N=5929). X-axis: mean BMI adjusted percent (BMI%). Y-axis: breastfeeding (yes vs. no).
The result of the multiple regression analysis showed that breastfeeding was significantly and inversely associated with BMI% of children with inclusion of covariates in the model (F(8, 4844)=38.88; p<0.0001; adjusted R2=0.0519). Covariates including maternal education, insurance status, family history of HCS and diabetes, child's asthma status, and birth weight of the infant were statistically significant in predicting variance in BMI% of the child (Table 1). The change in R2 when including the breastfed variable was 0.24%, which demonstrates that a small amount of unique variance is shared between breastfeeding and BMI% of the child after covariate inclusion.
Results of the Multiple Regression Analysis for All the Variables in the Model to Predict BMI Adjusted Percent (BMI%) of Fifth-Grade WV Children
Only covariates that were significant in the Spearman's correlation were used in the multiple regression analysis. Covariates included infant birth weight in grams, maternal education status as 1–17 years of education, maternal health insurance status at time of delivery (non-Medicaid vs. Medicaid), family history of diabetes (yes vs. no), family history of hypercholesterolemia (yes vs. no), and child's asthma status (yes vs. no). Covariates that were not significant and were excluded were maternal age, maternal smoking status, child's age, race, and gender.
WV, West Virginia; CI, confidence interval.
Discussion
The results indicated that the mean BMI% was significantly lower among children (age 11 years) who were breastfed, compared to children who were not breastfed, by a significant difference of nearly 3.4%. Additionally, the regression model showed that, compared to children who were not breastfed at infancy, there was a 2.5% decrease in the BMI% of children who were breastfed even after controlling for covariates. However, the change in R2 showed that breastfeeding accounted for less than 0.25% of unique variance in BMI% of children. Our results are consistent with other studies that have shown a significant, but small, inverse association between breastfeeding and childhood obesity. 30
Several covariates were not included in this study owing to lack of bivariate association, despite previous research suggesting the importance of inclusion. For example, previous research has observed this association mostly among non-Hispanic whites and not among other racial/ethnic groups. 36 However, this study did not find race/ethnicity to be a significant factor in the bivariate analysis and thus did not include this variable in the regression model. This may be because WV has a predominately white population (94%) consistent with Appalachian characteristics. 27 Moreover, our study did not find significant bivariate correlations between the main outcome of interest (BMI%) and maternal smoking status, maternal age, and child's age and sex and therefore did not include these covariates in the regression model. Weng and colleagues also found no association between maternal age, as well as the child's race/ethnicity and childhood obesity. 11 However, two systematic reviews found significant associations between maternal smoking during pregnancy and obesity in children.11,30 This null finding within our data was surprising, given that WV has one of the highest rates of smoking during pregnancy. 37
Significant covariates included in the study also bear some interpretation. The results suggest that with increasing years of maternal education at time of the child's birth, there was a decrease in the child's BMI%. Previous research has noted that maternal education is related to breastfeeding initiation and continuation, in addition to the child's weight. 38 The study used maternal health insurance status for maternal SES and found that children whose mother had Medicaid versus non-Medicaid health insurance at the time of birth had significantly higher BMI%. Data show that maternal SES plays an important role in the mother's decision and duration to breastfeed her child. 29 In addition, high infant birth weight has also shown to be risk factors for childhood overweight. 11 Our study also showed that there was a significant increase in the child's BMI% with increasing birth weight. Although family history of overweight and obesity has a strong association with obesity in children, this information was not available in either of the two data sets. However, controlling for family history of HCS and diabetes showed that children who had a family history of these illnesses had significantly higher BMI%. Asthma is also another potential confounder related to both exposure and outcome and was thus controlled for in this analysis.9,33,34 The study found that children who had asthma had a significant increase in BMI%, compared to children without asthma. 35
Our results are in concordance with other studies that have indicated a significant association between breastfeeding and the reduced risk of weight gain in children and adolescents after controlling for potential confounding variables.13,30,36 However, some of the limitations of the study include lack of information on important confounders, such as parental overweight or obesity status, child's physical activity, and dietary behaviors. 30 Information on actual breastfeeding was obtained retrospectively and thus is subject to recall bias and also to social desirability bias, given that women who believed that they should have breastfed were probably different from those that did not think breastfeeding was important. The measure also did not inquire about the duration or exclusivity of breastfeeding, or timing of solid food introduction, which may be important components when examining this association.12,39,40 In addition, the results from the regression analysis showed that although the predictors accounted for nearly 5% of the variance in BMI%, breastfeeding uniquely accounted for less than 1% of the variance. However, the small effect size of breastfeeding and childhood obesity is consistent with other studies. 30
Some of the strengths of the study included the ability to examine this association longitudinally using linked data from two cross-sectional studies. Moreover, the main outcome variable (BMI%) was calculated by measuring height and weight by trained healthcare professionals. The study used BMI% to overcome the ceiling effects in the tails of the normal distribution observed in other adiposity measures, owing to the fact that obesity in children is observed mainly by an increase of BMI distribution in the upper percentiles.24,26 This is particularly important given that breastfeeding may shift only the upper tail of the BMI distribution to the left and not the whole distribution. 41 To our knowledge, no study has examined the association between breastfeeding and childhood obesity taking into account the percentage difference between BMI and median BMI of children.
The numerous benefits of breastfeeding for both the mother and the child have been well documented in developed countries as well as in the United States.8,42 The Appalachia region of the United States has one of the highest rates of childhood obesity and the lowest breastfeeding rates in the nation. For example, the CDC Survey of Maternity Practices in Infant Nutrition and Care (mPINC) provide data on the extent to which evidence-based hospital practices and policies help mothers achieve their breastfeeding goals. WV had one of the lowest mPINC scores in the nation (higher score shows higher prevalence of maternity care practices that are supportive of breastfeeding). 43 Although the effect size of this study was small, considering the magnitude of the childhood obesity crisis, this finding suggests the need to improve breastfeeding rates in rural Appalachia as one of the strategies to prevent obesity during childhood and adolescence.
Conclusions
In conclusion, this study showed that breastfeeding is protective against childhood obesity among fifth-grade school children in the state of WV. Our study adds to the argument of encouraging breastfeeding as one of the potential preventative measures in reducing childhood obesity prevalence.
Footnotes
Acknowledgments
The West Virginia Birth Score Program is funded under an agreement with the West Virginia Department of Health and Human Resources, Bureau for Public Health, Office of Maternal, Child and Family Health. The CARDIAC project is funded by the West Virginia Bureau of Public Health. The authors thank the children and families who have participated in the CARDIAC Project and the Birth Score Project
Author Disclosure Statement
No competing financial interests exist.