
Abstract
Abstract
Background:
Novel interventions within child care settings are needed for childhood obesity prevention. The aim of this study was to determine the impact of a short-term nutrition education pilot intervention on preschool-age children's snack food choices.
Methods:
Children ages 3–5 years (n = 49) from one child care setting participated in a short-term nutrition education intervention (nine 30-minute interactive lessons) taught over a 2-week period. Pre-post assessments included snack knowledge and snack preference questionnaires and an observed snack selection trial to allow children to choose between a healthy and unhealthy snack choice similar to the current food environment. Children's height and weight were measured and BMI z-scores calculated. Parental reports of demographics and child's food preferences were also collected at baseline.
Results:
Children significantly improved their preference of healthier snacks (p = 0.03) and the ability to distinguish them (p = 0.03) from other snacks. However, they did not significantly improve (p > 0.05) their snack choice between a healthy and unhealthy choice immediately after the short-term nutrition education program. Children who were younger (p = 0.003) or who had higher nutrition knowledge scores (p = 0.002) were more likely to select the healthy snack after the intervention.
Conclusions:
This study provides evidence that a short-term nutrition education program improves preschool children's knowledge about healthy snacks, but does not translate to immediate healthier snack selections for all children. Future research should investigate the optimal duration of a nutrition education program in a child care setting and other external influences (parents, policy) most influential on snack choice and eventual obesity risk.
Introduction
Childhood obesity is a public health issue currently affecting approximately 23.8% of children ages 2–5 years. 1 Children who are overweight or obese as preschoolers are more likely to be overweight or obese as adults and have increased risk of chronic disease.2,3 The propensity toward becoming obese often occurs early in life as feeding patterns, dietary habits, behavioral habits, and parental feeding practices are established. 4 Over the past two decades, the consumption of foods with added sugars, solid fats, and sodium within diets of children ages 2–6 years has increased. 5 Dietary consumption of excess sugar-sweetened beverages and/or foods with higher dietary fat have been associated with higher body weight in young children.6,7 In contrast, the consumption of fruit and vegetables (FVs) has been associated with the prevention of cardiovascular disease in adults8–10 and with lower body weight in children.6,7 However, though younger children are more likely to meet recommendations for FV intake, compared to older children, the choices consumed most frequently within those food groups are often fruit juice and French fries, respectively, which may contribute additional calories through added sugar and fat.11–13
Because food preferences are still forming throughout the first 5 years of life, 14 eating behaviors are an important area of attention. Repeated exposure to healthy foods during this key developmental window is critical to enhance the familiarity of foods, such as FVs, and increase intake.15,16 As children grow older, the likelihood of spending time away from home increases. Approximately one third of children under the age of 5 years are cared for by a nonrelative 17 and therefore consume meals and snacks away from home under the supervision of others. A child care setting, such as a preschool, is often the first place that children are introduced to behaviors that differ from those they are familiar with at home; therefore, it becomes an ideal place to introduce new and healthy foods. 16 However, it is estimated that children in child care are consuming only one third of a serving of fruit and one quarter of a serving of vegetables per day. 18 The quality and choices of snack food options provided within child care settings may be a contributor to this inadequacy. Snacks within child care centers are frequently comprised of sweet and salty foods compared to infrequent inclusion of foods, such as FVs. 19 Children's snacks in general tend to be high in added sugar and overall calories.20,21 Providing a variety of FV snack choices in a child care setting has previously resulted in increased intake in preschool children. 22 Therefore, educational outreach to child care centers as well as to children regarding choosing healthy snacks is needed.
Previous studies with young children have provided evidence that nutrition education is effective in changing knowledge and preference for foods such as FVs.23,24 But, many of the interventions are several months or more in length23–25 and may not be sustainable by preschool classroom staff because of limited resources. Further, the impact of nutrition education interventions on observed immediate actual food choices of young children is often not evaluated 24 or is self-reported by parents.23,25,26
Novel approaches and early interventions that are time- and cost-effective are needed to prevent childhood obesity. A short-term nutrition education intervention directed toward preschool-age children and focused on snack food choices in a child care setting may be a potential strategy for decreasing risk of obesity in young children. Although the most powerful level of influence on a preschooler's snack choices is unknown, a child care setting offers an ideal place to examine the strength of these possible influences.
The primary aim of this study was to determine whether a short-term nutrition education program can favorably influence preschoolers' snack choices in a child care setting. The secondary aim was to determine what child characteristics (gender, age, BMI z-score, ethnicity, race, preferences, and knowledge) are associated with choosing a healthy snack over an unhealthy snack. It was hypothesized that children who are educated about healthy snack choices will improve their ability to identify healthy versus unhealthy snacks and will be more likely to choose, and to eat, the healthier snack when given the choice between a healthy and a less healthy snack. Further, it was hypothesized that children who were female, older, with a healthy BMI z-score, non-Hispanic, white, and/or had higher knowledge or preference scores would be more likely to choose the healthy snack.
Methods
Study Design
A traditional pre/post intervention design was used at one main preschool site during the summer through fall of 2013 for this pilot study. Each individual child (ages 3–5 years) within a classroom (10–20 children per classroom) served as his or her control. The nutrition education program intervention (nine 30-minute interactive lessons) was taught by one registered dietitian every day over a 2-week period to each classroom.
Participants and Recruitment
The study was approved by the University of Connecticut–Storrs Institutional Review Board for Human Subjects. Research assistants recruited children from preschool families during pick-up hours and information sessions at the preschool using study recruitment flyers. Informed (written) consent was obtained by at least one parent/guardian for each child participating in the project before any data collection. Minimum sample size of n = 40 children (effect size = between 0.5 and 0.6; alpha = 0.05, power = 0.8) was determined based on using a paired t-test to measure changes in the children's snack food choice after the nutrition education intervention. To allow for attrition and missing data, a total of 70 children were enrolled in the project (Fig. 1). If parents did not provide consent (n = 3), children were invited to participate in the education program, but no data were collected.
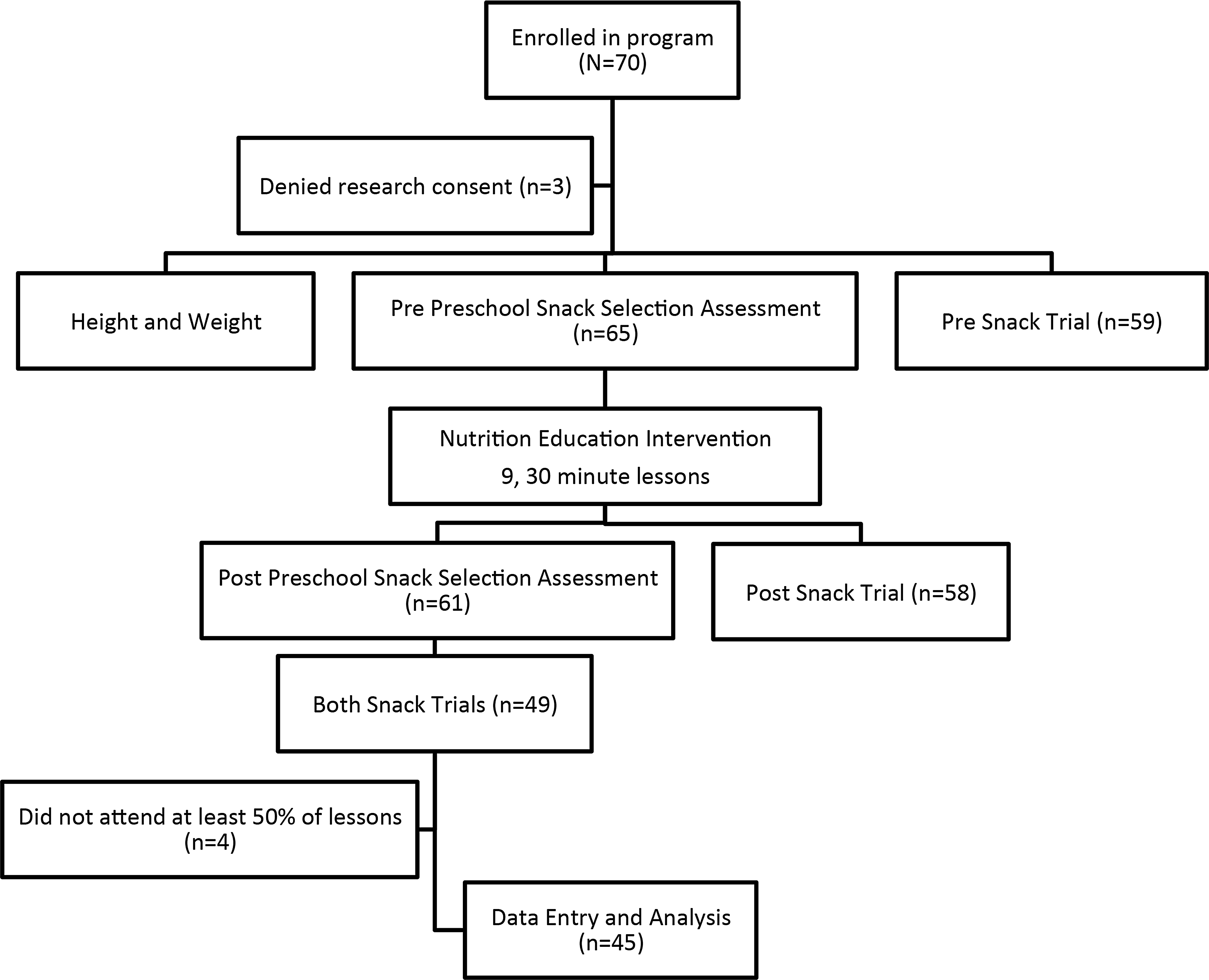
Study design and enrollment of participants.
Study Intervention
The study intervention included one unit (“Eat Smart”) from a previously tested, larger-scale, interdisciplinary childhood obesity prevention program. 27 Based on the obesogenic ecological model that recognizes influences of the home and surrounding environments (i.e., schools) on a child's risk for obesity, the intervention included materials for children, teachers, and parents. Content focused on teaching and empowering children about distinguishing between healthy and unhealthy snack foods. Healthy snack foods, labeled “Go” foods, were identified as foods that help keep one's heart, muscles, and bones strong, whereas unhealthy snack foods, labeled “Whoa” foods, were identified to not help keep one's heart, muscles, and bones strong. 24 A total of nine 30-minute lessons were taught by a registered dietitian 4–5 days a week over 2 weeks. Classroom extension materials were provided to each teacher. Newsletters with supporting activities were sent home to parents as reinforcements. Attendance was taken daily for each child.
Measures and Data Collection Procedures
Assessments were conducted with the children at pre and post by one trained graduate assistant. Children's ability to identify certain snack foods (α = 0.76) and indicate their knowledge (α = 0.87) and preference (α = 0.88) for certain snacks was assessed using the Preschool Snack Selection (PSS) tool, which was previously tested in a similar preschool population. 24 The PSS includes snack food picture cards of the foods that were taught in the education program.
Some measures were conducted at baseline only and included the following. Children were weighed and measured with a digital scale (Seca 869) and stadiometer (Seca 217) using standard techniques. 28 Whereas weight loss was not an expected outcome of the study, BMI was calculated and used to calculate BMI z-scores 29 for analysis investigating other variable relationships. Parents completed demographic and snack preference questionnaires. The snack preference questionnaire was adopted from the Preschool Adapted Liking Survey as a method to assess liking preferences for certain foods as reported by the parent. 30 It was modified to include foods (α = 0.70) specific to the nutrition education intervention.
Snack choice was assessed through direct observation during snack trials scheduled immediately before and immediately after the full nutrition education intervention. The purpose was to replicate the potential scenario in which a child was given a choice between a healthy and unhealthy snack food, such as in the current US food environment. Snack trials occurred during normal snack times in the afternoon for the children. Food allergies were noted before any snacks were chosen or provided. Children were queued outside the classroom and, when instructed, individually entered the classroom and were offered a choice between two snack options portioned in identical soufflé cups: (1) grapes cut into halves (approximately half a cup) or (2) two small chocolate chip cookies. Each choice provided a similar volume of food. Children were unable to view other children's snack choices using this method. Once a snack was chosen, each child would then be seated to consume their snack. Each child's snack choice and amount consumed were recorded by one of two observers on a snack trial recording form.
Grapes and cookies were selected as the snack choice options to represent the “healthy” and “unhealthy” options, respectively. These snacks were chosen because they were previously provided by the preschool before the program as routine snack choices and featured in the nutrition education intervention. Food allergies and novelty were not concerns. Both snacks were sweet foods, and individual preferences as reported by each child's parent were rated high. On a scale from 0 to 7, the mean (standard deviation; SD) preference score was 5.9 (1.1) for cookies and 6.0 (1.0) for grapes.
Statistical Analysis
Data analysis was conducted using SPSS software (version 21.0, 2012; IBM, Armonk, NY). Statistical level of significance was set at p < 0.05. Children with missing data from pre or post snack trials or who attended four lessons or fewer were excluded from analysis. Nonparametric tests were used for the majority of the analyses because of the limited sample size.
McNemar's chi-square test was used to compare children's snack choices before and after the intervention. The Wilcoxon's rank-sum test was used to determine whether children's knowledge of, and preferences for, healthy snack choices improved after the intervention. Additional analyses were performed to determine whether child characteristics, such as age, gender, ethnicity, race, BMI z-score, and snack preference scores, were associated with snack choices after the intervention. Independent two-sample t-tests were to determine whether children's postsnack choices varied with respect to age or BMI z-score. Fisher's exact test was conducted to determine whether children's postsnack choices varied with respect to gender, race, or ethnicity. The Wilcoxon-Mann-Whitney's test was conducted to determine whether the snack knowledge and preference assessment scores differed between children that chose grapes versus those who chose cookies.
Results
Based on completion of the intervention and all assessments including the snack trials, a total of sample of 45 children was used for analysis. Demographic information, such as education level, race/ethnicity, and number of children, was self-reported by the parents of participating children (Table 1). Though family income status was not directly assessed, at least half of the families within the study were low income as indicated by the eligibility of the child care center to receive USDA Child and Adult Food Care Program benefits. After the short-term intervention, children scored significantly higher on their ability to identify the healthier of two snacks, as well as verbally stating a higher preference for the healthier of two snack options (Table 2). However, the majority of children did not significantly change or improve their snack choice (Table 3).
Demographic and Weight Status Information of Preschool-Age Children Participants
SD, standard deviation.
Comparison between Pre- and Poststudy Mean Sum Scores for Preschool Snack Selection Assessment
Wilcoxon's signed rank sum.
SD, standard deviation.
Comparison of Preschoolers' Snack Selections at Pre- Versus Postintervention
McNemar's chi square (χ2): p > 0.05.
Further analysis was conducted in order to determine whether children who opted for cookies at post-test versus those children who opted for grapes at post-test differed by certain characteristics. On average, children who were younger were more likely to choose the healthy snack choice (grapes) after the intervention (Table 4). Children who chose grapes post-test also had higher increases in knowledge of healthy versus unhealthy snack foods (Table 4).
Differences in Characteristics of Preschoolers Who Choose a Healthy Snack Versus an Unhealthy Snack after a Nutrition Education Program
Independent two-sample t-test (age, BMI z-score); Wilcoxon-Mann-Whitney (knowledge snack score, preference snack score); and Fisher's exact test (gender, race, ethnicity).
SD, standard deviation.
Discussion
The short-term (2-week) nutrition education pilot intervention in the present study resulted in improved knowledge and self-reported preferences for healthy snacks by preschool age children in a child care setting. This is promising and consistent with improvements in nutrition knowledge and preferences resulting from other nutrition education programs for young children.24–26 However, the present study did not result in immediate snack choice improvements after the program. Interventions targeting dietary behavior change in preschool-age children may require a minimum amount of time before changes in food choices are observed, and this could range from at least 1 month to several years.25,31,32 Though positive results were noted after several weeks or months on preschool's nutrition knowledge or dietary intake from other program interventions,25,33 this length of time may not be feasible or realistic within a child care site because of limited resources.
There are other possible explanations for why an immediate improvement in snack choice was not observed. For instance, in a study with children ages 5–12 years, the children ranked taste as the number one reason for snack choice followed by health. 34 However, both of the snack choices in the present study were similar in sweetness and rated similar in preference. Yet, when given the option to choose foods, children in another study more frequently opted for the unhealthy choices, similar to the present study, even though they verbally understood the difference in healthfulness. 34 Though we were not able to formally capture qualitative data, there were anecdotal reports from children in the present study about knowing that the grapes were the healthy choice, but opting for the cookies during the postsnack trial. Further, in a study with children ages 9–11 years, when the children were asked to rate a beverage with the label “healthy,” they rated it lower and less likely to request it in the future. 35 It is unknown whether using the term “healthy” as it relates to snack choices with preschoolers can promote a negative result, such as a lower likelihood of choosing and consuming a healthy snack.
Competitiveness of foods is also a potential explanation for why fewer children opted for the healthy snack. In a study with older school-age children, it was found that if only FVs were available, children ate healthier; however, if these healthier food options were competing with less healthy foods, such as chips and ice cream, students chose the unhealthy foods, ultimately undermining the effects of the healthier school meal. 36 This highlights the importance of providing a healthy food environment, but does not address the fact that children will be faced with a variety of options in the current obesogenic environment. The current study tested a realistic condition where similarly sweet, but opposing nutritional quality, snack choices were offered and snack choice and consumption by preschool-age children observed. Previous studies including preschool-age children have primarily focused on improving available food choices at home or in a child care environment and relied on self-reported dietary changes by parents, rather than investigating the impact of nutrition education on independent food choices of preschoolers when presented with healthy versus unhealthy options.
Although the snack choices in the child care environment were controlled in the current study and peer influences were eliminated, there was limited outreach and education to the parents and no manipulation of the home environment. A previous study found that children increased their consumption of FVs when parents' consumption increased, as well as when the availability of foods in the house was high. 37 But, parents might be inclined to purchase and offer foods that they know their children like, such as cookies, instead of introducing new foods or foods they perceive their children to dislike because parents fear that they will be refused. 38 However, one unmeasured benefit of nutrition education is its potential role in increasing a child's ability to serve as his or her own advocate for healthy snack choices as purchased or provided by parents. This is an important consideration for young children given that they continue to gain more independence in selecting foods, such as in a child care or school environment and within the general obesogenic food environment.
Although there were no differences in snack choices by preschool-age children according to gender, race, BMI z-score, or stated snack preferences, possibly owing to the inability to detect them in a small sample, there were differences in snack choices by child age and nutrition knowledge at postintervention. Whereas our hypothesis stated that older children would be more likely to choose a healthy snack based on the premise that they would be more cognitively apt to process the program concepts, it has been previously reported that as children advance from elementary to middle school, their consumption of fruits, vegetables, breakfast, and milk decreased while soft drink consumption increased. 39 Consistent with this trend, the proportion of children meeting the current recommendations for foods such as FVs decreases as children age. 40 Therefore, age may be a negative factor in food choices and possibly impacted by other influences, such as the environment. Further, nutritional knowledge, although not always a determinant of food choice, is an important step in the process of improving food choices among children. 41 These factors, among others not measured in the current study, may all play a role in a young child's ultimate snack choice decisions.
Strengths of the study include that the project was implemented in one preschool child care site, eliminating variance from differing meal or snack norms, curricula, or teaching differences across sites, and that the intervention and assessments were each conducted by two different researchers to avoid bias or social desirability of the children's answers. The observed snack selection trial protocol helped minimize outside influences of peers or teachers on children's snack choices and tested a realistic environmental setting containing competitive food choices typically lacking in other studies. The short-term duration of the intervention made it feasible, cost-effective, and undisruptive to the regular school schedule. Even though preferences for both snack food choices were rated high and similar for children and that both of the choices were provided as options during the child care's regular snack time, the consumption frequency of these foods, and thereby novelty, was not assessed. Other limitations include the small study sample size, because several children were absent for more than half the intervention and several data points were missing owing to family vacations. Whereas at least 50% of the children were from lower-income families, the homogeneous sample of children from one geographical location also makes it difficult to extrapolate results. The lack of a control group and longer-term follow-up could have prevented detection in snack choice changes as well, but the study aimed to only pilot the intervention especially in regard to observed snack choices by preschoolers immediately after the short-term nutrition education program. Some data were also self-reported information from parents.
Conclusions
Results from this pilot study revealed that despite gains in nutrition knowledge, children were less likely to choose and eat a healthier snack option when offered the choice between a healthy snack and an unhealthy snack immediately after a short-term nutrition education intervention. Because time and resources are often limited in child care settings, future research should investigate the minimal amount of nutrition education exposure needed to influence snack choice behaviors of preschool students when faced with a choice. It is also important to investigate the additional targets or combination of targets (e.g., teachers, family, and food policy environment) needed to significantly change preschoolers' snack decisions, such as to include FVs while considering the cost-effectiveness of interventions. 42 This pilot study recognizes the reality that even when food options, such as snacks, are limited to healthy choices through policy change, children will be faced with competing food options to choose from in other settings. This supports the need for not only policy change, but also frequent and targeted education to help children navigate an obesogenic food environment that contains both healthy and unhealthy snack options.
Footnotes
Acknowledgments
Funding was provided, in part, by the USDA NIFA Hatch Project (#CONS00907) and the USDA Cooperative State Research, Education, and Extension Service Award (2010-85215-20662). The authors thank the staff and families from the Mansfield Discovery Depot for agreeing to be a host site for this project. They also thank Jaime S. Foster, MS, RD, for teaching the intervention lessons and Dooti Roy for assisting with statistical analysis. Further, the authors thank the team of researchers (Madeleine Sigman-Grant, PhD, RD, Anne Lindsay, PhD, and Teresa Byington, PhD) who developed the program curriculum used in part within this study.
Author Disclosure Statement
No competing financial interests exist.