
Abstract
Abstract
Background:
We describe the development, testing, and analysis of the B.E. S.T.R.O.N.G. program, a comprehensive family-based multidisciplinary child obesity treatment program. The program uses an innovative Internet-based health tracker that was developed by the Children's Wellness Institute (CWI) for data collection, analysis, and storage.
Methods:
Data were obtained on 112 subjects who enrolled in the B.E. S.T.R.O.N.G. program in several healthcare institutions during the 2013–2014 academic year. There were 74 females and 38 males. The mean age was 9.75 ± 2.21 years. There were 89 white, 14 African American, 3 Hispanic, and 6 listed as other. Height and weight data were collected during the first, fourth, and seventh week. Diet and exercise data were collected in a HIPAA-compliant manner each week for seven weeks, using the health tracker, and transmitted electronically for statistical analysis and storage.
Results:
Subjects involved in the program demonstrated significant weight loss, averaging 3.8% reduction in BMI from their starting point. Weight loss in these subjects was associated with significant and measurable changes in diet, physical activity, and screen time. Participants in the B.E. S.T.R.O.N.G. program increased fruit and vegetable consumption to more than five daily servings and also demonstrated significant increases in the consumption of grains and protein foods. Furthermore, they maintained screen time at less than one hour per day, and increased all forms of physical activity to exceed one hour daily.
Conclusions:
The Internet-based health tracker demonstrated the effectiveness of the B.E. S.T.R.O.N.G. program, delivered by several healthcare institutions, in treating childhood obesity.
Introduction
Childhood obesity currently affects 17% of all children ages 3–20 and is the most prevalent nutritional disorder in the United States. 1 It is also one of the costliest. 2 Children and adolescents who are overweight or obese have demonstrably higher annual medical costs than children whose weights are normal. The increased costs are due primarily to increased expenditures in outpatient treatments, prescription drug use, and emergency room visits.3,4 Annually, the average total health expenses for a child treated for obesity under Medicaid is $6,730, while the average health cost for all children covered by Medicaid is $2,446. 2 Comparable increased costs are seen for children with private insurance. 2 If left untreated, childhood obesity can lead to serious and expensive medical problems later in life, including heart disease and type 2 diabetes.5,6 Because of the huge financial burdens posed by this disorder, treatment of child obesity is now a covered benefit, mandated by the Affordable Care Act to be provided through insurers (www.healthcare.gov/preventive-care-benefits/children/).
Over the past few years many programs have emerged to deal with the problem of childhood obesity. 7 These programs are conducted by public health departments, community organizations, and hospitals and healthcare systems throughout the country. Most focus on the family as the agent of change, and their goals are to promote healthier eating, increase physical activity, and reduce screen time, and at the same time, promote healthy self-esteem.8,9 While many of these programs report success in terms of patient attendance or weight measurement, few report data relating to changes in behavior that may have contributed to weight loss and weight maintainence.10–12 Such data include several key behaviors that have been shown to contribute to obesity in children: namely, reduced physical activity, increased beverage consumption, increased screen time, and increased portion size. Such findings would be useful in delivering cost-effective methods to reduce health risk and promote healthcare savings. Many childhood obesity treatment programs are community based and have been frequently run without the help of research staff or support. It was the need for a low-cost, automated data collection method coupled with the availability of mobile technology that led to the initial development of the online health tracker reported here.
Tate et al. have recently described the potential role for mobile-Health (mHealth) technology in the prevention and treatment of childhood obesity, citing that “mHealth systems offer state-of-the-art approaches to intervention design, delivery, and diffusion of treatment and prevention efforts. Benefits include cost effectiveness, potential for real-time data collection, feedback capability, minimized participant burden, relevance to multiple types of populations, and increased dissemination capability.” 13
Many programs directed at obesity treatment for adults including Weight-watchers.com and myfitnesspal.com have been using mHealth technology (www.weightwatchers.com; www.myfitnesspal.com). To date, there have been no reports of the use of such trackers in group programs for childhood obesity.
In response to the obesity epidemic, the American Academy of Pediatrics (AAP) published its recommendations for medical nutrition therapy for obese children. For those children whose BMIs are at or above the 95th percentile, the AAP recommends a multidisciplinary program that includes family-focused counseling and meetings. 14 Topics that should be included in these programs are shown in Table 1.
Topics for a Comprehensive Child Obesity Treatment Program
The topics listed are the components that the AAP recommends for a comprehensive program designed to treat childhood obesity. 14
A critical component of the AAP recommendations is the use of self-monitoring logs, which are useful for participants in reinforcing the skills needed to lose and maintain weight. Analysis of such data would help to identify factors that contribute to the efficacy of such programs; however, the cost of analysis is often prohibitively expensive. Having the participant enter their own data, which is collected and stored securely and can be transmitted for immediate statistical analysis, serves two important purposes: the first, to assure that the data are collected securely and analyzed with no additional program costs; and the second, to analyze the data in real time, which provides some immediate feedback to the participant.
In this paper we describe the development and testing of a comprehensive family-based multidisciplinary program, which uses an innovative Internet-based health tracker that provides immediate feedback to participating families and program staff. The tracker allows for rapid and comprehensive analysis of the data from multiple participants in a HIPAA-compliant manner for use in outcome reporting. Data can be collected from multiple sites and easily be segregated for analysis and dissemination.
Methods
In 2012, the Children's Wellness Institute (CWI) put together a team that included a board-certified pediatric endocrinologist, nutritionists, fitness instructors, and health educators to develop a state-of-the-art family-based childhood obesity curriculum. The curriculum was based on the recommendations of the AAP, and incorporated the topics shown in Table 1. The result was the • B Eat Breakfast every day, Be active, use your Brain (by using the tracker) • E Eat Smart, Exercise Every day • S Strength, Serving Sizes, Support • T Limit TV, Total nutrients • R Respect yourself, smart Restaurant eating, Relax and stretch • O Eating on special Occasions, One hour of exercise every day • N No juice, No junk food, getting rid of a Negative body image • G Gratitude for friends, family and for myself
The concepts and content of the B.E. S.T.R.O.N.G. program were designed to meet or exceed the requirements of the AAP for structured medical nutrition therapy for obese children.
10
These include the following:
• Written meal plans with emphasis on the importance of family meal times, limiting eating out, consuming a healthy breakfast, and preparing meals at home. Encouragement of dairy and water consumption and limited juice intake. The meal plans are calculated based on the RDA for age and sex for children, which are published on the USDA website, Supertracker.gov (www.supertracker.usda.gov), and provided to students on week 2 of the program. • Written exercise plans: Weekly exercise sessions focus on aerobics, muscle strengthening, and flexibility. The program encourages participation in the President's Active Lifestyle Award Challenge (PALA). • Behavior modification goals: Teaching participants to set goals for exercise and nutrition and how to achieve them; limiting TV and computer screen time; teaching parents how to encourage healthy behaviors. • Frequent visits with registered dietitian (RD) and coordination of care with primary care physician. • Outcome assessment and analysis with the health tracker, which provides an easy-to-use online data collection interface.
The CWI licenses the B.E. S.T.R.O.N.G. curriculum and associated materials as a turnkey program to several business entities. These business entities include community-based health organizations, insurance companies, and hospitals around the country that have expressed an interest in dealing with childhood obesity and have identified a market within their service area that would benefit from this service program. Licensees and participants access all deliverables electronically by way of the website for use online or downloadable for print. Program participation is considered exempt from institutional review boards at the licensing facilities. Licensees have to meet certain staffing requirements in order to implement the program as well as demonstrate that they have adequate facilities to conduct the classes. The staff requirements for the B.E. S.T.R.O.N.G. program include site coordinator (SC), physical activity instructor (PAI), registered dietitian (RD), and mental health professional (MHP).
Student Enrollment
Students qualify for the program based on their age (6–14 years) and if their healthcare providers or primary care physicians identify them as having a BMI greater than the 95th percentile. Each licensee determines further student qualifications as they pertain to insurance coverage or eligibility for other payment sources.
Class Structure
Classes meet for 90 minutes, one time per week for a period of eight weeks at a central location. The SC maintains the schedules, enrolls participants, and keeps in contact with the families during the week and ensures their return to class. At the beginning of each class the RD conducts a 15-minute cooking demonstration and teaches a nutrition lesson. Following this, the PAI supervises a 30-minute physical activity session. The MHP conducts discussion groups based on topics listed above. Lessons are taught from the comprehensive curriculum via the workbooks. Students are instructed to identify goals for nutrition, activity, and behaviors, and to record daily food intake and physical activity using the health tracker.
The curriculum is comprised of a workbook written for a fourth-grade reading level intended for children ages 6–14 years, and an Internet-based health tracker developed specifically for this program. The workbook and all associated training materials have been designed by an award-winning graphic team, and are accessible by participants in printed form, as well as electronically on computers or smartphones. A sample of a health tracker page is shown in Figure 1.
Screenshot of the Internet-based health tracker employed in the B.E. S.T.R.O.N.G. program. This example shows the daily Food Group Choices, which are clicked for each day and transmitted at the end of each week.
Materials suitable for reading at the fourth-grade level have been widely used by us and others in a family-based program, because they allow both collaborative work with parents for the younger child and independent work for children older than 10 years of age (www.highmarkfoundation.org/aboutus/news/2012/03-19-2012.shtml). For children younger than 10, the joint participation of parent and child in the program allows the parent to work with the child using the workbook and the tracker. Children at or above grade four can do many of the exercises and read the material from the workbook independently. Because the program requires parent participation, both the child and the parent are familiar with the material. This common knowledge is helpful in reinforcing the behavioral changes that are part of the program.
As part of the curriculum, students and parents are taught to use the Android and iOS compatible health tracker to keep a daily record of their intake of grain foods, fruits, vegetables, and dairy and protein foods, as well as minutes of exercise and screen time. For students who did not have access to the Internet or smartphones, the sites were provided with tablets to use for data entry at the beginning of each weekly class. The technology allows the daily collection of student data with their full knowledge and compliance. The data collected for week 1 are obtained during the week following the first class. Sites are unable to provide trackers to children prior to the first class; thus participants have in fact received some intervention before they actually start reporting their data.
Data collection requires minimal time on the part of program staff. Additionally, the tracker is linked to a statistical analysis site, which permits rapid analysis of data from multiple participants (Qualtrics LLC, Provo, UT). At the time of enrollment, the students are provided with an ID, comprised of the student's initials, year of birth, gender, race/ethnicity, and site code, under which to enter their tracker data. The HIPAA-compliant electronic health tracker provides complete transparency of student progress to students, families, licensees, and agencies requiring outcome reports. The reported data for one participant using the online tracker is shown in Table 2.
Weekly Health Tracker Data for One Subject
The numbers represent the BMI calculated from the height and weight for an individual subject reported at the class visit, the averages for daily servings of each food group consumed, and minutes per day of each activity, calculated from the data collected in the health tracker during one week by that subject.
Data Analysis
The data were collected from individual students, who were identified by a coded ID number that designated site, year of birth, gender, and race/ethnicity. The data were stored by a statistical analysis vendor for subsequent analysis (Qualtrics, LLC, Provo, UT).
Data collected during the eight-week B.E. S.T.R.O.N.G. program were used for comparison to baseline data obtained at week 1. Descriptive data reported included the ages, gender, and race/ethnicity of participants. The means and standard deviations were calculated for all measures; and statistical analyses were performed using t-tests, with significance accepted at a level of p < 0.05. The primary endpoints that were tested include weight and BMI, which were obtained at weeks 1, 4, and 7 of the program, and compared using paired t-tests. Additionally, we examined the significance of specific behavior changes, using paired t-tests. These included the differences in diet, including reported food group consumption, changes in daily minutes devoted to screen time, and changes in minutes devoted to physical activity, defined as moderate physical activity, strength building activity, and stretching activity.
Results
During the period 2013–2014, CWI licensed the B.E. S.T.R.O.N.G. program to five entities around the country. The data were collected from three licensing healthcare facilities that enrolled a total of 118 students.
Data Analysis
Complete data were obtained on 112 subjects who enrolled during the 2013–2014 academic year. There were 74 females and 38 males. The mean age was 9.75 ± 2.21 years. There were 89 white, 14 African American, 3 Hispanic, and 6 listed as other.
Height and weight data were collected during the first, fourth, and seventh week; data were available on 112 subjects at week 1, 74 subjects at week 4, and 61 subjects at week 7. The reporting rate for this program was 66% at week 4 and 54% at week 7. Participants were asked to record diet and exercise data each week for seven weeks, using the health tracker. All data were collected in a HIPAA-compliant manner and transmitted electronically to a third-party vendor for statistical analysis and storage. 19
Changes in Weight and BMI
Participants showed significant changes in weight and BMI during the course of the B.E. S.T.R.O.N.G. program. As seen in Figure 2, there was a significant change in weight during the eight-week program. At week 1 the mean weight was 131.8 ± 55.3 lb; by week 4 the mean weight for all subjects was 128.0 ± 46.5 lb (p < 0.010) versus week 1, representing an average weight loss of 4 lb, or nearly 1 lb per week. At week 7 the mean weight was 125.9 ± 52.9 lb (p < 0.015) compared to week 1, representing an additional average weight loss of 2 lb during this same period. Overall, weight loss was 3.8% over the seven-week program. The mean BMI for participants was similarly reduced during the seven-week program: at week 1 the BMI was 28.4 ± 6.37 kg/m2. At week 4 the mean BMI had fallen to 27.8 ± 5.71 kg/m2 (p < 0.010), and at week 7 the mean BMI was 27.1 ± 7.01 kg/m2 (p < 0.015) by paired t-analysis versus week 1. The data reflect a reduction in BMI by 1.1 kg/m2 over the seven weeks, which represents a change in BMI of −3.8%.
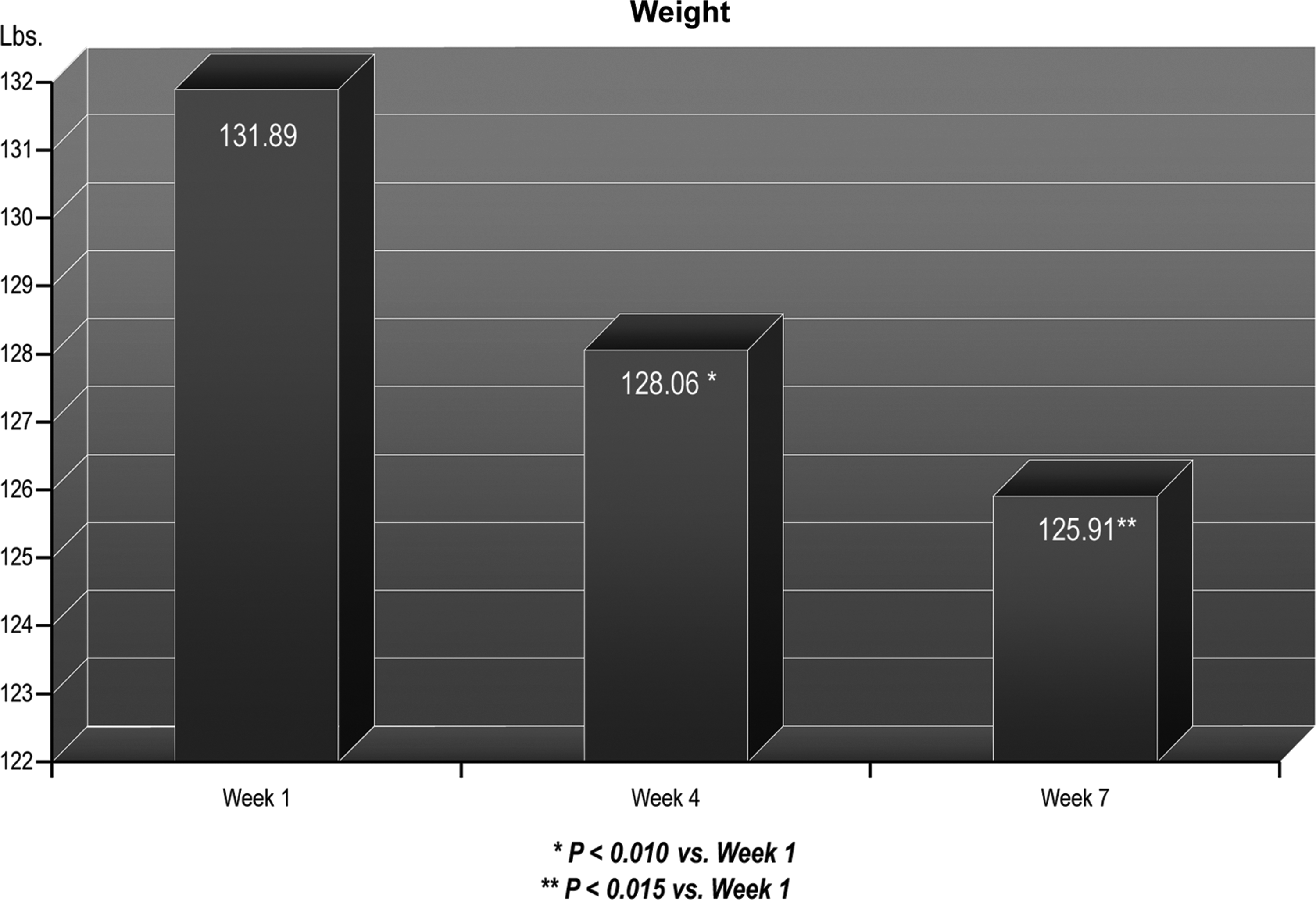
Data represent the mean BMI values for all participants at week 1, week 4, and week 7 of the B.E. S.T.R.O.N.G. program.
Changes in Eating Behavior
Food diary data were reported on 85 subjects from week 1, 56 subjects at week 4, and 41 subjects at week 7, and are reported in the aggregate, as shown in Figure 3. Subjects showed significant changes in their reported consumption of grains, fruits, vegetables, and protein foods during their participation in the B.E. S.T.R.O.N.G. program.
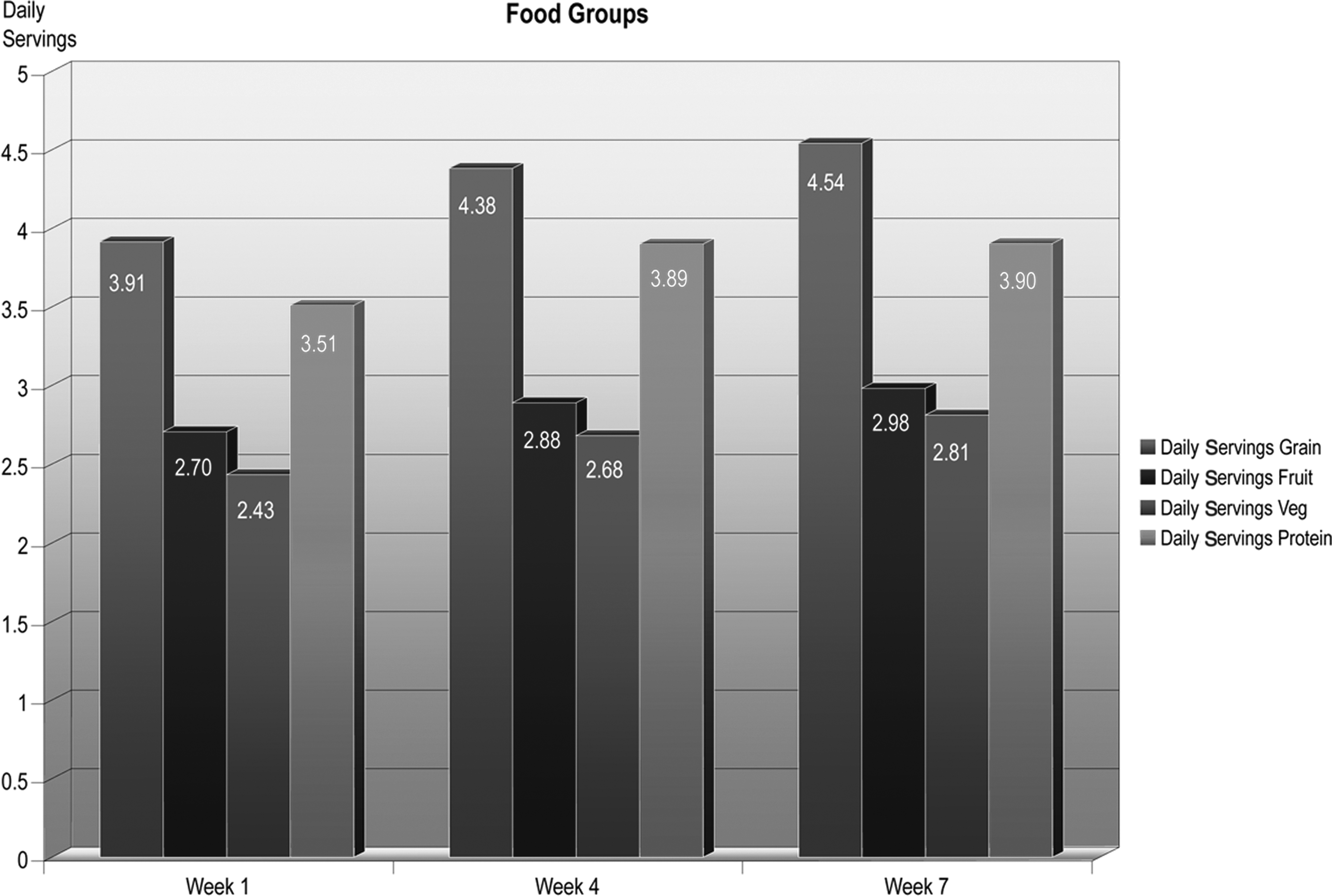
Data represent the mean daily servings from the Grains, Fruits, Vegetables, and Protein groups obtained from the Internet-based health tracker for all participants at week 1, week 4, and week 7 of the B.E. S.T.R.O.N.G. program.
The daily consumption of grains increased from 3.9 ± 1.7 servings at week 1 to 4.6 ± 1.6 servings at week 7 (p < 0.005), representing an increase of 18%. Daily fruit consumption increased from 2.6 ± 1.1 servings at week 1 to 2.9 ± 1.0 servings at week 4 (p < 0.050), and 3.0 ± 1.2 servings at week 7, although the difference was not statistically significant at week 7. Participants showed increased vegetable consumption, from 2.50 ± 0.88 servings to 2.80 ± 1.07 servings per day at week 4 (p < 0.050) and 2.8 ± 1.2 daily servings at week 7, although again, the difference was not statistically significant at week 7.
The consumption of protein foods increased significantly for subjects during the B.E. S.T.R.O.N.G. program, from 3.5 ± 1.30 daily servings at week 1 to 3.9 ± 1.35 daily servings at week 4 (p < 0.050). At week 7, protein servings remained significantly higher compared to week 1, at 3.9 ± 1.25 daily servings (p < 0.10), which represented an increase of 8.3%. The daily servings of dairy foods was 2.9 ± 0.70 and did not change significantly when reported at week 4 and week 7.
Changes in Screen Time and Physical Activity
Students were instructed to record the number of minutes per day devoted to screen time, including computer, video games, and television viewing. At week 1, as shown in Figure 4, subjects who participated in the B.E. S.T.R.O.N.G. program reported a mean of 40.2 ± 9.65 minutes per day of screen time a week. Over the eight-week B.E. S.T.R.O.N.G. program, the time devoted to screen time was gradually reduced; by week 4 screen time fell to 37.2 ± 10.72 minutes per day (p < 0.1) and at week 7 reported screen time fell further, to 35.2 ± 11.33 minutes per day, although the difference was not statistically significant. Nonetheless, the trend toward an overall reduction in screen time of 12.5% was noted in participants of the B.E. S.T.R.O.N.G. program.
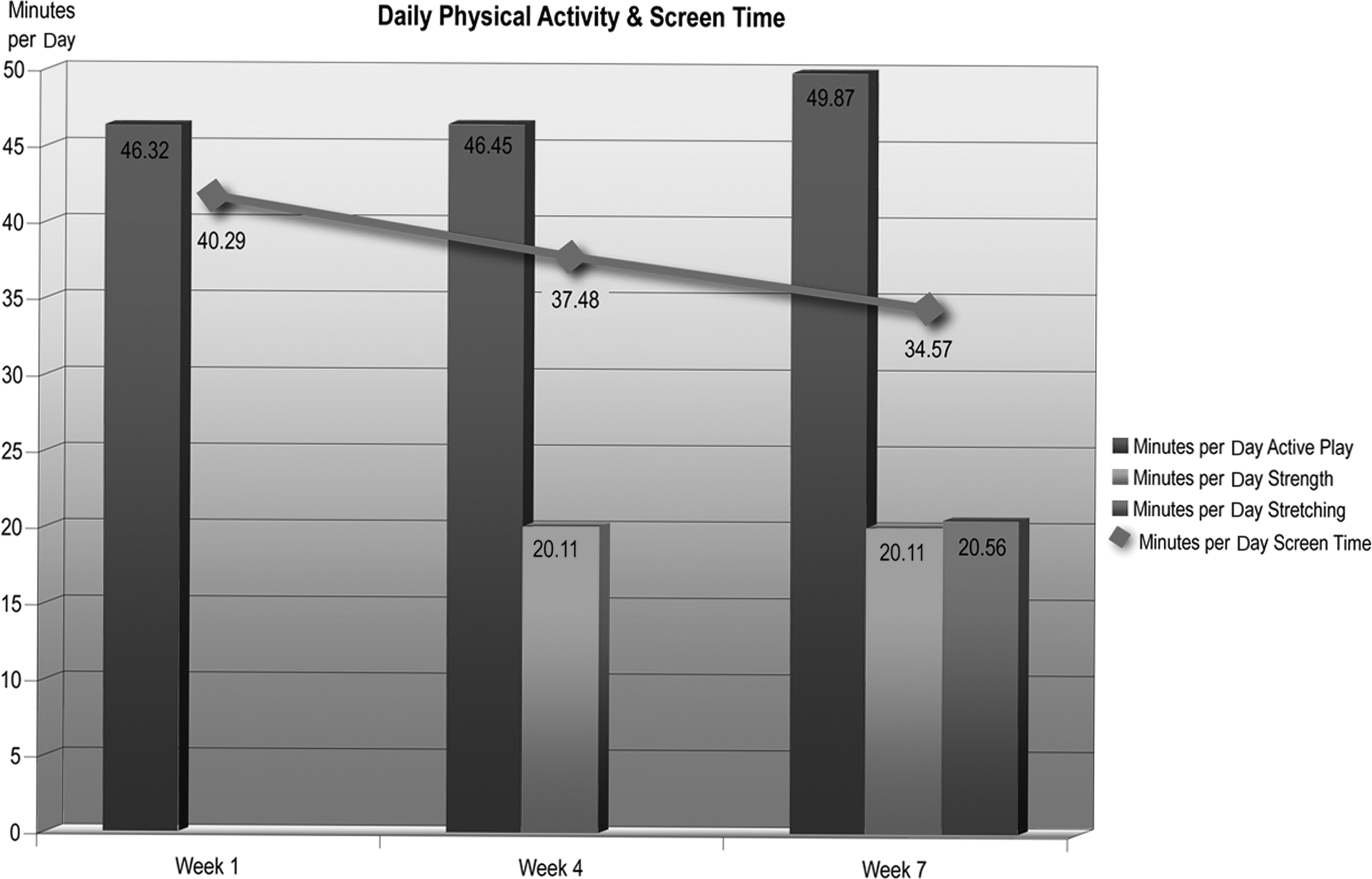
The green bars represent the mean number of daily minutes devoted to moderate physical activity recorded in the Internet-based health tracker and reported at weeks 1, 4, and 7 for all subjects. The tan bars represent the mean number of daily minutes devoted to strength-building activities, reported at weeks 4 and 7 for all subjects. The purple bar represents the mean daily minutes devoted to flexibility activities reported at week 7 for all subjects. The red symbols represent the mean daily minutes devoted to screen time reported at weeks 1, 4, and 7 for all subjects.
Participants in the B.E. S.T.R.O.N.G. program also were asked to track daily physical activity in minutes per day. These data were analyzed in the aggregate and reflect the mean values in minutes per day at each week. The amount of time devoted to active play, defined as moderate continuous physical activity, increased from 46.3 ± 12.95 minutes daily at week 1 to 49.9 ± 14.86 minutes daily at week 7, as shown in Figure 4. Over the course of the B.E. S.T.R.O.N.G. program, participants were taught strength training and stretching activities, which they were also asked to record. When these activities are included, the total amount of time devoted to daily physical activity increased from 46.30 ± 12.95 minutes per day of active play at week 1 to 90.56 ± 7.15 minutes per day of physical activity, including active play, stretching, and strength training, at week 7. As seen in Figure 4, the amount of time devoted to all forms of physical activity as reported by participants nearly doubled over the seven weeks.
Conclusions
The purpose of this study was twofold:
• To determine the effectiveness of an eight-week family-based child obesity program, based on guidelines of the AAP.
14
• To test the feasibility of an Internet-based health tracker designed to be compatible with the curriculum for use in the collection of data from participants for immediate analysis.
This study demonstrates that the B.E. S.T.R.O.N.G. program curriculum, developed in accordance with the guidelines of the AAP, provided effective nutrition education and behavior modification, leading to weight loss and improved diet and physical activity in children who are obese and from diverse communities. Subjects involved in the program demonstrated significant weight loss, averaging 3.8% reduction in BMI from their starting point. These findings are comparable to other community-based programs.7–10,15
Why Was This Program Effective?
Using the AAP guidelines, we used a family-based model in which groups of 10 or more children and their parents met on a weekly basis for group lessons and discussion about specific topics related to diet, exercise, and behavior.
The use of a family-centered approach to child obesity is based on the assumption that the family provides the major social learning environment, through behavior modeling, which in turn determines the child's eating habits.11,12 Studies have shown that 80% of the time a child will eat following adult models eating; and their food preferences are influenced by the exposure to foods in the home. 16 Family-based programs are often more successful in the treatment of childhood obesity than are school-based programs, not only because they engage both the parent and the child in nutrition education, but they also permit behavior modification techniques, both for the child in terms of setting limits on behavior and for parents in terms of learning to function as effective agents of change.17,18
In addition to demonstrating the efficacy of a child obesity treatment program based on the AAP guidelines, the overarching purpose of this paper was to report on the adaptation of an inexpensive widely available software for use as a means of data collection and reporting for a children's weight loss program.
We believe that we were successful in proving the premise of this paper, that the adaptation of this data collecting software works as an effective health tracker because (1) the software program collected and stored diet and activity data in real time from individual participants; and (2) it provided statistical analyses of the data, again in real time, allowing immediate feedback to the participant and/or other involved parties. Using this methodology, we were able to demonstrate weight loss and report changes in behavior of the group.
The health tracker provided immediate feedback to participating families and program staff. The tracker also allowed rapid and comprehensive analysis of the data from multiple participants attending the programs held at several healthcare delivery sites. With the Internet-based tracker, the racial/ethnic characteristics of the participants were identified using a HIPAA-compliant collecting system. A significant critique of previous studies is the lack of data related to the ethnic/racial makeup of the participants. 19
Subjects reported diet and exercise behavior as part of their participation in the program. Using the health tracker data analyses, it was possible to show that weight loss in these subjects was associated with significant reported changes in diet, significant increases in physical activity, as well as reduced screen time. The measured changes that occurred during this program included the following:
• Increases in consumption of grain and protein foods. • Increases in fruit and vegetable consumption, exceeding the five per day recommendations of public health programs (www.letsgo.org/wp-content/uploads/lets-go-2013-final-singlesb.pdf). • Increases in physical activity, exceeding 60 minutes per day. • Limited screen time at less than two hours per day.
The observation that participants increased their consumption of protein and grain foods was surprising and not previously reported, but was in keeping with the curriculum, which emphasized food with low caloric density and higher nutrient value.
Will the Reduction in Obesity Persist?
The likelihood that changes in obesity will persist is strengthened by the use of a family-centered teaching model. Successful diet modification requires parental understanding, support, and compliance with the changes to be made. 11 As in other forms of family therapy, the family-based model used in the B.E. S.T.R.O.N.G. program focuses on both the child and the parent; the long-term effects are that both are aware and educated about the specific concerns of diet and physical activity. They can hold one another accountable. The students have achieved success and the parents have demonstrated that they can function effectively as agents of change. The likelihood of success is greater in this learning situation than has been observed in strictly school-based programs where parents have no role in the process.17,18 However, there is a need for the social environment to change as well. After a participant has completed this program and learned a specific set of behaviors related to healthier food consumption and increasing physical activity, continuing these behaviors is more likely to occur in an environment where these behaviors are valued. The likelihood that these changes will persist is further supported by the following observation.
The B.E. S.T.R.O.N.G. curriculum is based on teaching concepts that were used in Kidshape, a program I directed for nearly 30 years. 20 This program was licensed by the Highmark Foundation from 2007–2012 (www.highmarkfoundation.org/aboutus/news/2012/03-19-2012.shtml). Independent analysis from the Highmark Foundation showed that, “Over one third of participants (35%) maintained their BMI loss at one year, with an average loss of 1.64 kg/m2. For Highmark program participants who lost about this amount (1.56–1.62 kg/m2), a 12-year-old female who grew 1.75 inches gained only 3.3 pounds one year later. An eight-year-old male who grew 2.5 inches gained just under four pounds one year later.”
There are some limitations to these findings. The data are self-reported, but steps have been taken to ensure that children were not over/underreporting. The program requires that a parent or guardian attend with the student participant for all eight classes. Parents receive instruction simultaneously with their student and are required to help them complete the health tracker and to participate with the student in physical activity at least once or twice per week. Most student participants have requested help from the parent or actually require input and/or prompting from the parent to oversee or complete the health tracker during the week, prior to the next class.
These findings are important, because childhood obesity remains an epidemic and is now one of the costliest disorders affecting children.1–4,21,22 Moreover, it appears that overweight that begins in childhood and persists into adulthood is associated with more severe obesity. 4 Because of the huge financial burdens posed by this disorder, treatment of child obesity is now a covered benefit, mandated by the Affordable Care Act to be provided through insurers. 5
Over the past few years, many programs have emerged to deal with the problem of childhood obesity. In her paper, Griffith reviewed 80 such programs, which were submitted to the National Initiative for Children's Healthcare Quality (NICHQ). 23 These programs were conducted by public health departments, hospitals, and healthcare systems throughout the country; half the programs were conducted in hospitals and/or clinics. Most focus on the family as the agent of change, and their goals are to promote healthier eating, increase physical activity and reduce screen time, and maintain or build healthy self-esteem. 7 For most of these programs, however, there are insufficient reportable outcome data related to race, ethnicity, or socioeconomic status. Furthermore, little data exist related to which changes in behavior contribute not only to weight loss but also to weight maintenance. 8 This may be due to the limited staff time and resources available to community-based childhood obesity programs. Data collection and analysis is time and labor intensive. However the lack of data handicaps the individual programs by hindering financial reimbursement from payers and thereby limiting their sustainability. Furthermore, lack of data from the multiple programs offered around the country has hindered the identification and validation of best practices in the treatment of child obesity, particularly in diverse communities.
The present study has shown that the B.E. S.T.R.O.N.G. curriculum was effective in treating childhood obesity, and the associated Internet-based health tracker provided a HIPAA-compliant method for data collection and analysis. This program provides a low cost and effective solution to address the needs of community-based organizations that are attempting to address the problem of childhood obesity. The HIPAA-compliant electronic health tracker provides complete transparency of student progress to students, families, licensees, and agencies to which CWI or their clients must report outcomes.
Future studies using the tracker will be designed to identify the key differences between subjects who failed in their outcomes as compared to those who were successful. There are several questions to be addressed using this health tracker that are important in understanding the behavior of overweight and obese children. For example, it may be possible to identify differences in the behavior of children who lost more weight compared to others who lost less. Similarly, it should be possible to determine if there are measurable differences in behavior (i.e., diet consumption and physical activity) between children who lost weight and those that did not. If these behaviors are promoted early enough in a child's life, we believe they can be maintained throughout their lives.
Additionally, the tracker could be used to explore changes in family behavior that could simultaneously influence parental health. Up to 20% of parents who participate in childhood obesity treatment programs with their children lose weight and demonstrate changes in eating and exercise behavior. 11 The recognition of common behavioral patterns that could result in health improvement for families should lead to better, cost-effective strategies to reduce healthcare costs of the obesity epidemic for both children and adults.
Footnotes
Acknowledgments
We gratefully acknowledge the participation of the following organizations which licensed the B.E. S.T.R.O.N.G. curriculum during the 2013–2014 academic year: Lake Health Wellness Institute, Concord Township, Ohio; Pinnacle Health System, Harrisburg, Pennsylvania; Resolute Health, New Braunfels, Texas; Somerset Community Hospital, Somerset Pennsylvania; and Sutter Health Foundation, Yuba City, California.
Author Disclosure Statement
Dr. Neufeld is the medical director of CWI. She holds an equity share in the company.
Informed Consent
All subjects were registered participants in the B.E. S.T.R.O.N.G. program at their respective institutions. They signed consent forms agreeing to participate in the family-based weight management program and to utilize the health tracker. All of the data were collected and transmitted in accordance with HIPAA regulations.