
Abstract
Abstract
Background:
The American Academy of Pediatrics (AAP) recommends a staged approach to pediatric weight management, starting with helping families to make targeted dietary and activity changes. This pilot study evaluated the preliminary efficacy of a pediatric practice-based referral program to support parents in helping their overweight/obese children improve their weight-related behaviors and BMI.
Methods:
A nonrandomized intervention study with contemporaneous control was used. Parents and their children ages 8–12 with BMI ≥85th percentile (N = 37) were recruited from a pediatric practice serving a low-income, multiethnic population. Providers delivered brief intervention and referred families to six weekly FITLINE telephone counseling sessions with a nutritionist who guided parents in helping their child make AAP-recommended changes. Child BMI and parent survey of child diet and physical activity were completed at baseline and 3 months. Medical record data from 44 children matched for age and BMI were collected.
Results:
Mean change in BMI from baseline to 3-month follow-up was −0.49 BMI units (standard deviation [SD], 0.95; p = 0.007) for the FITLINE group and 0.35 BMI units (SD, 0.96; p = 0.02) for the control group. Adjusting for baseline BMI, age, and sex, children in the FITLINE condition reduced BMI significantly more than children in the control condition (mean difference = −0.89; p = 0.0003). Significant improvements in many dietary and sedentary behaviors also were noted.
Conclusions:
The FITLINE program reduced short-term BMI and improved dietary and sedentary behaviors. A randomized, controlled trial is warranted to assess the program's efficacy and potential to serve as a model for reducing obesity in pediatric practice.
Introduction
Over one third of preadolescent children in the United States (36%) are currently overweight or obese (BMI ≥85th percentile for age and sex). 1 The American Academy of Pediatrics (AAP) recommends a staged approach to the management of pediatric overweight and obesity,2,3 starting with stage 1, Prevention Plus, encouraging families to make targeted healthy lifestyle choices related to eating and activity. The pediatric primary care setting can serve as an important role in addressing childhood overweight and obesity in the United States, given that most children ages 5–14 (72–79%) are observed for well-child visits each year. 4 Initial studies suggest the potential of pediatric office-based strategies.5–13 However, promising interventions require multiple sessions with the clinician,7–13 who report lacking sufficient time or training to deliver effective weight counseling.14,15 The AAP also identifies centralized referral centers as a key part of a comprehensive plan for the treatment of pediatric obesity2,3; however, both pediatricians and families, particularly low-income families at highest risk of pediatric obesity, have limited access to these services.16–18
In response, we developed the FITLINE pediatric practice-based referral program. The FITLINE is a parent-centered intervention delivered by centrally located nutritionists to guide parents in making AAP-recommended lifestyle changes. The aim of this article is to report the outcomes from a pilot study evaluating the efficacy of the FITLINE program in improving BMI and weight-related lifestyle behaviors among children who are overweight or obese ages 8–12 observed in pediatric primary care practice.
Methods
Study Design, Setting, and Participants
A nonrandomized intervention study with contemporaneous control was used. Thirty seven parents and their children ages 8–12 with a BMI ≥85th percentile for age and sex were recruited over an 8-month period in 2013 from an academic pediatric primary care practice in Central Massachusetts affiliated with the University of Massachusetts Health Care system that primarily serves a low-income, multiethnic population. If a family had more than one eligible child, the oldest child was invited to participate. From the contemporaneous control group, medical records were reviewed to identify children (n = 44) from the same primary pediatric practice matched for age and BMI observed over the same time period with the same eligibility criteria.
Recruitment and Informed Consent
Potentially eligible children (8–12 years old, overweight or obese per medical record from their most recent visit and not meeting the exclusion criteria above) with an upcoming well or acute care clinic visit were identified through the practices' existing scheduling and medical record systems. The pediatrician received an e-mail about their patient being potentially eligible, and the clinic staff placed the one-page description of the study with the patient's visit materials. During the clinic visit, the pediatrician provided the parent and child the one-page description of the study; if interested, the pediatrician had a referral form faxed to the project director, who then mailed the consent form and a baseline survey to the participant. The project director then called to explain the study, obtain informed consent, and conduct the baseline survey. The study was approved by the University of Massachusetts Medical School Institutional Review Board and registered with Clinicaltrials.gov (NCT02085434).
Intervention: The FITLINE Program
The FITLINE program included practice and parent components. The pediatric practice-based component consisted of reviewing the medical records of children with upcoming clinic visits to identify children with BMIs in the overweight and obese range and prompting providers to intervene by referring interested parents to the FITLINE. Thereafter, providers received feedback from the FITLINE nutritionist on the family's progress so that they could either support maintenance of improvements gained or refer for additional intervention if needed (see Fig. 1).
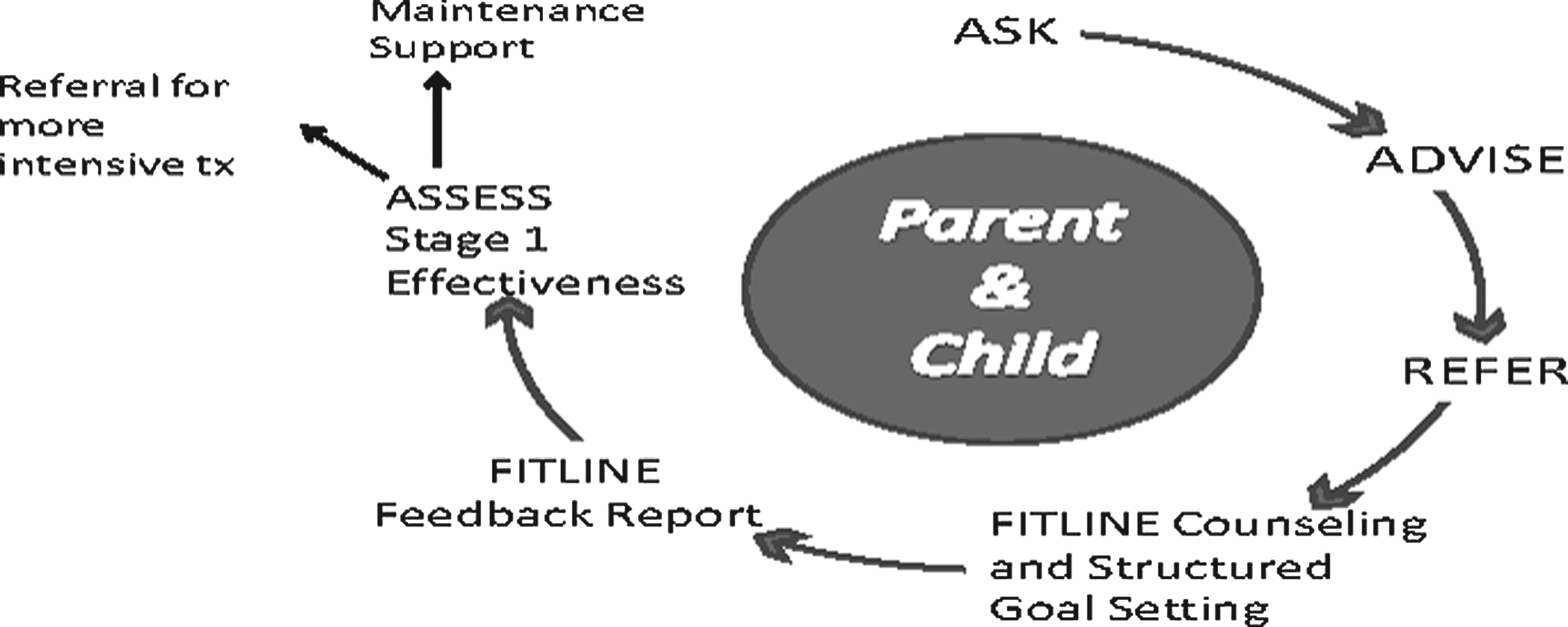
Integrating referral to a centralized counseling program into pediatric practice.
The parent support component was designed to provide an easily accessible resource to help families make AAP-recommended stage 1 lifestyle changes. Parents received six weekly 30-minute FITLINE telephone counseling calls delivered by a registered dietician who provided guidance in helping their child make targeted lifestyle changes (see Table 1). Calls were scheduled at a time convenient for the parent, including nights and weekends, with one of the three nutritionists assigned to the same family for consistency. During the calls, the nutritionist used motivational interviewing to teach proven parenting techniques and strategies, and provided practical tips and resources tailored to the unique needs, culture, and lifestyle of each family, facilitated by a booklet presented in a clear, simple format for a low-literacy population (see Table 2 for FITLINE strategies).
FITLINE Session Protocol Targeting the American Academy of Pediatrics (AAP) Stage 1 Prevention Plus Recommended Priority Behaviors for Children with BMI ≥85th Percentile
Social Cognitive Theory (SCT) Constructs and Related FITLINE Strategies
The conceptual model and theoretical framework of the FITLINE program is based on the AAP recommendations (motivational interviewing, goal setting, positive reinforcement, and monitoring) 19 and is grounded in Bandura's social cognitive theory (SCT). 20 SCT posits that people learn by receiving instruction and guidance on how to engage in a behavior, observing or hearing of the actions and outcomes of others' behavior, and verbal persuasion, encouragement, and support. 21 SCT states behavior change involves a number of key constructs, described in Table 2 along with related FITLINE strategies.
Measures
Child BMI and parent survey of child diet and physical activity (PA) were completed at baseline and 3 months postbaseline for families in the FITLINE condition only. Weight and height for all children in the FITLINE condition were measured for all children by one person, the project director, using standard methodology. BMI was calculated from weight (kg)/height squared (in meters). Demographics and weight-related self-management behaviors were assessed using phone surveys completed by parents, administered by the project director. Surveys and BMI assessments were completed before initiation of FITLINE intervention calls at baseline. At baseline, the survey assessed demographics (age, sex, and race of both parent and child; employment status, level of education, relationship to the child, and marital status of parent). At baseline and 3 months later, the parent survey included a 12-item survey from the Youth Risk Behavior Surveillance survey assessing the number of days in the past week their child engaged in key dietary behaviors (e.g., eating breakfast, fast food or restaurant meal, and dinner with family) and PA behaviors (e.g., play sports, watch television [TV], or play video/computer games). 22 Also assessed was the number of days in the past week their child ate five fruit or vegetables, and drank water, fruit juice, and punch/sweet tea/soda/sports drinks.
Medical record data from a contemporaneous control of 44 children observed in the same primary pediatric practice over the same time period (January through September 2013) were collected. These children were matched for age and BMI and had height and weight measurements taken twice within a 3-month period.
All participating providers took part in a group debriefing session to assess their satisfaction with the program, ease of implementing the pediatric practice-based component of the intervention including provider prompts, introducing lifestyle changes and the FITLINE program, and referral process.
Statistical Analysis
Changes in BMI from baseline to 3-month follow-up within each study condition were assessed using paired t-tests. A general linear model was used to compare study groups regarding change in BMI, adjusting for baseline BMI, age, and sex. Parallel analyses were conducted for BMI z-score (BMIz). Bhapkar's test for marginal homogeneity 23 was used to assess changes in diet and activity in the FITLINE intervention group. Analyses did not adjust for follow-up time, because it was similar for both groups (p = 0.356). Data were collected and managed using REDCap electronic data capture tools hosted at the University of Massachusetts Medical School. 24
Results
Recruitment and Referral Feasibility
During the 8-month recruitment period, there were 1184 eight- to twelve-year-olds scheduled for a clinic appointment to see their provider during the 7-month recruitment period (February 2013–August 2013); these were discrete patients (i.e., if they were observed twice during that time period, they were only counted once). Of the 1184, based on a review of the medical records, 415 were BMI eligible (35%), and, of those, 100 (24%) were ineligible for the following reasons: attention deficit hyperactivity disorder (ADHD) medication (11%), Spanish speaking (7%), intellectual or physical disability (4%), and seeing a nutritionist (2%). An additional 64 (15%) failed to show up for their clinic visit. Of the 251 patients who were eligible and attended their clinic visit, 71 (28%) were referred by their provider to the FITLINE. Providers noted that they had a number of key reasons why they did not refer families to the FITLINE program and study: the child was not the clinician's patient; the child was close to 85th percentile and engaged in healthy lifestyle behaviors; the parent reported a lack of motivation to make lifestyle changes; or the parent declined assistance/noted they were too busy to participate. Of those families who were referred by the provider, over half (37; 52%) were able to be reached and agreed to participate in the study. See Figure 2 for the Consolidated Standards of Reporting Trials (CONSORT) flow diagram.

CONSORT flow diagram. ADHD, attention deficit hyperactivity disorder; CONSORT, Consolidated Standards of Reporting Trials.
Baseline Participant Characteristics
Mean age of the 37 children participating in the FITLINE study was 9.6 years (standard deviation [SD], 1.5). Mean BMI was 26.8 (SD, 3.0). The sample was 37.8% female, drawn from a clinic that was predominantly low income, and representing the diverse racial/ethnic mix of Central Massachusetts: 18 white; 11 Hispanic; 5 black; and 3 multiracial. Seventy-eight percent of parents were overweight or obese based on self-reported height and weight. There were no statistically significant differences between FITLINE participants and the contemporaneous control group at baseline in child's sex or BMI, only in age (contemporaneous controls were a mean of 10.6 years old; p < 0.001).
Study Retention
Three months after study enrollment, 36 of the 37 enrolled children returned to the clinic for height and weight measurements (97% study retention), and all 37 parents completed the phone survey (100% study retention).
Change in BMI, BMI Z-Score, and BMI Percentile
Mean change in BMI from baseline to 3-month follow-up was −0.49 BMI units (SD, 0.95; p = 0.004 for the FITLINE group and 0.35 BMI units (SD, 0.96; p = 0.02) for the control group. The adjusted between-group difference in BMI change was statistically significant (–0.89; p = 0.0003), indicating that children in the FITLINE condition were 0.85 BMI units lower than children in the control condition at 3-month follow-up (see Table 3; Fig. 3). Results for BMIz were similar, with a mean decrease of −0.099 (SD, 0.101; p < 0.0001) for FITLINE versus a mean increase of 0.004 (SD, 0.094; p = 0.8032) for controls and an adjusted between-group difference of −0.101 (p < 0.0001; see Table 3). Results also were similar for BMI percentile, with a mean decrease of −0.58 (SD, 0.84; p = 0.0002) for FITLINE versus a mean increase of 0.05 (0.54; p = 0.5566) for controls and an adjusted between group difference of −0.68 (p < 0.0001; see Table 3).
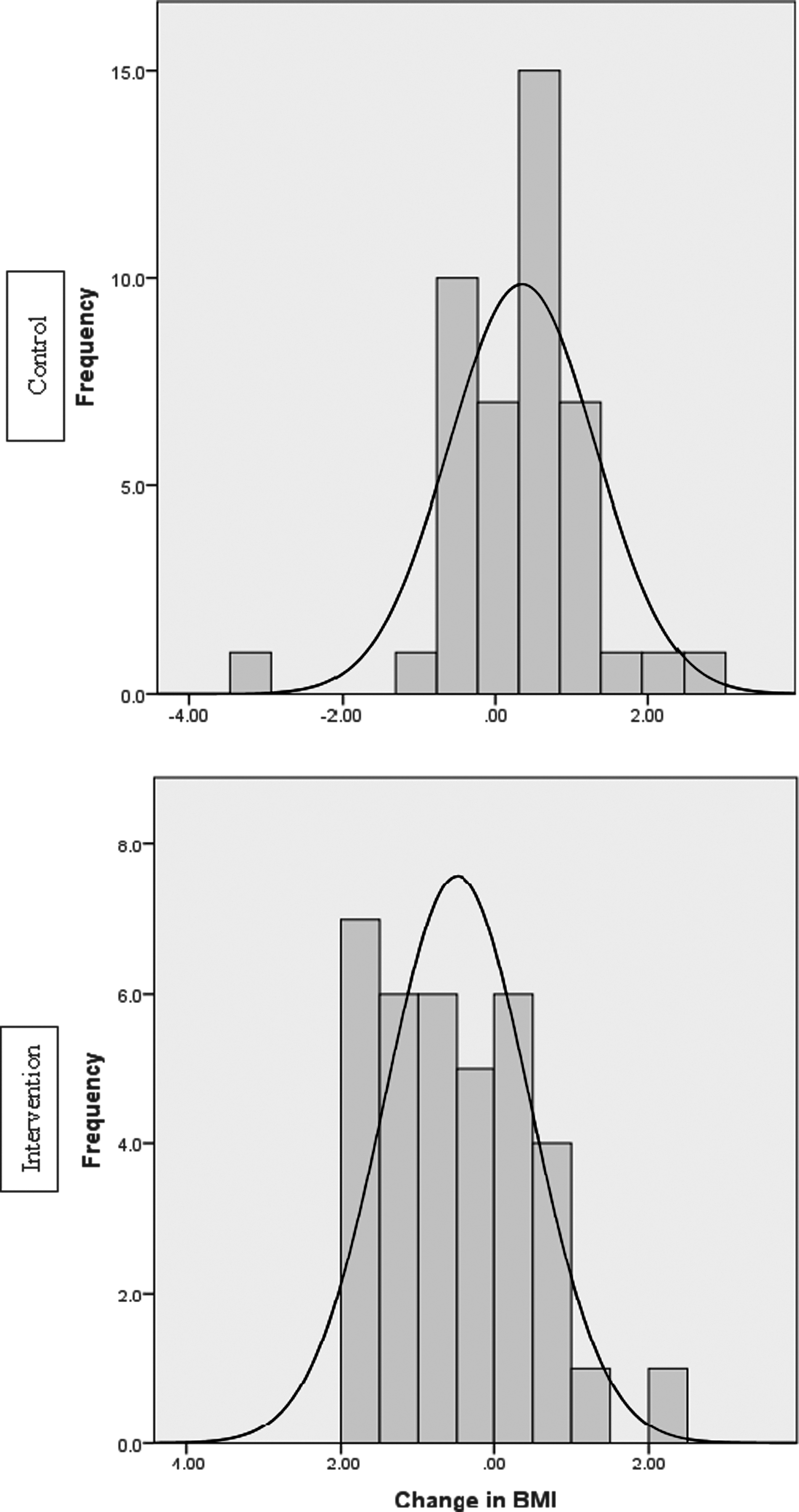
Distribution of change in BMI by condition.
BMI, BMI Z-Score, and BMI Percentile Change in FITLINE Intervention (N = 36) vs. Contemporaneous Control (N = 44) at 3-Month Follow-Up
SD, standard deviation; CI, confidence interval.
Changes in Diet and Activity (FITLINE Condition Only)
There were significant changes from baseline to follow-up in many of the parent-reported child dietary and activity weight-related behaviors in the FITLINE condition, including reductions in fast food/restaurant meals, desserts, juice, higher-fat milk, and sedentary behavior, as well as increases in consumption of fruit and vegetables (see Table 4). In addition, there were marginally statistically significant reductions in recreational computer use and hours of TV watched (p < 0.10).
Changes in Diet and Activity from Baseline to 3-Month Follow-Up (FITLINE Intervention Group, N = 37)
Bhapkar's test for marginal homogeneity, an extension of the McNemar test for 3+ response categories.
TV, television.
Parent Feedback Regarding the FITLINE Counseling Intervention
Eighty-one percent of families completed all six FITLINE phone calls. In one-on-one interviews after participation in the FITLINE, parents reported most liking: (1) personalized feedback and concrete, practical recommendations that the nutritionist helped tailor to their child, and family's unique needs and culture; (2) setting goals and homework assignments; (3) feeling listened to by the nutritionist, reflecting the tailored, patient-centered counseling approach used; and (4) the convenience and flexibility of receiving intervention by telephone versus in-person visits.
Parents unanimously reported they were able to put into action strategies discussed with their FITLINE nutritionist. Examples included using the Hunger Scale to help their child identify satiety and reduce portion sizes, reducing calories by switching to lower-fat options, offering healthier meal and snack choices, making opportunities for PA, and reducing screen time. Parents reported high receptivity to the pediatric provider referring them to the FITLINE.
Pediatric Provider Feedback/Acceptability of the Intervention
Pediatricians reported that the patient identification, provider prompts, and referral process went smoothly in clinics, that they were easily able to introduce the issue of lifestyle change and FITLINE program, and that they appreciated having an easily accessible resource for their families. The providers reinforced the need for the weekly support provided by the FITLINE counseling, which they noted they are unable to provide in the clinic.
Discussion
In the present study, children in the FITLINE intervention condition were 0.89 BMI units, 0.101 BMIz units, and 0.68 BMI percentile units lower than children in the contemporaneous control condition at 3-month follow-up, adjusting for baseline BMI, age, and sex. BMI reduction in similarly aged children has been shown to improve markers of both glucose metabolism and lipid metabolism dysregulation, which are pathophysiological drivers of obesity-related morbidity and mortality, relative to stable overweight peers.25,26
To understand which lifestyle elements may have driven the reduction in BMI, diet and activity variables were measured through parent surveys. Key dietary changes noted in the FITLINE children were reduced intake of meals outside the home, desserts, fruit juice, and increased consumption of fruits and vegetables. The latter finding is consistent with a recent study of parents of 3- to 5-year-old children in Australia that found four weekly 30-minute calls was associated with greater fruit and vegetable consumption. 27 There also were changes in sedentary behavior, specifically reduced screen time. Thus, the success of the FITLINE intervention is likely attributable to multifaceted lifestyle changes, rather than changes in a single variable.
The success in achieving multiple lifestyle changes is likely a result of targeting of the FITLINE to parents. Previous research has shown that parent-centered interventions are more effective for children than child-centered interventions.28,29 In a new review from the AAP Committee on Nutrition by Daniels and Hassink, 30 the case is strongly made that family-based interventions are more effective than child-only interventions, with parents playing a major role. Therefore, the FITLINE was built on the premise that parent-centered interventions for children under age 12 are more successful because, equipped with sufficient education and tools, parents can influence a large proportion of their child's day through healthy foods in the home and meal and snack preparation.
The value of the FITLINE is predicated on the ability to encourage and motivate parents to participate in the program by a two-step process: recruitment and engagement of parents to complete the program. For recruitment, the AAP recommends the pediatrician's office as a critical venue to screen for overweight and obesity and to initiate the treatment process. 2 Over half (52%) of parents who were invited to participate in the study and take part in the FITLINE telephone counseling calls by their pediatrician were receptive to participating, affirming the recommendation to initiate treatment in the pediatrician's office. Future research should identify reasons for nonadherence among the 48% who did not agree to participate and accept the referral. Therefore, assuring pediatricians that referral to the FITLINE is well received by parents and worthwhile for their patient populations is a crucial component of the recruitment step. Our poststudy debriefing showed universal satisfaction among participating pediatricians, who found the FITLINE counseling calls both easy to participate in and worthwhile. This is further supported by other studies in which pediatricians have affirmed the need for routine counseling for parents of children who are overweight and obese, and their lack of time and resources to meet this need. 18 There is now precedent for a joint role of pediatricians and ancillary support, such as nutritionists and registered dieticians (RDs). For example, Resnicow and colleagues 31 recently described a pediatrician/RD intervention conducted across 42 practice sites in which motivational interviewing was successfully delivered to parents of children who were overweight, resulting in lower BMI compared to parents receiving usual care of counseling from a pediatrician along.
Recruitment of parents must be complemented by parent completion of the FITLINE telephone counseling calls. Motivating busy parents to invest several hours into the FITLINE telephone counseling calls requires satisfaction with the topics covered as well as with their interactions with the nutritionists. Key factors of the FITLINE counseling calls scored well with parents, including receiving personalized feedback and concrete, practical recommendations, goal setting, nutritionist empathy, and the convenience and flexibility of receiving the intervention from the same nutritionist by telephone versus in-person visits. Further, 81% of parents completed all six phone calls, validating parents' self-reported satisfaction, because they were willing to invest the time into completing the program.
Study Limitations
The study population was small and drawn from one pediatric practice in Central Massachusetts. However, low-income and minority children, who are typically defined as high risk, 32 were over-represented and hence a strength of this study. Heights and weights were taken for intervention and control children during the same time periods, on the same scale, and BMIs were comparable at baseline. Participants serving as controls were not chosen randomly, and it is not known what the circumstances were that led children in the comparison condition to have two measured weights within a 3-month window, although the same exclusion criteria for FITLINE children applied to children in the control condition. In addition, the intervention group may have been more motivated given that they were invited and willing to participate in the study, whereas the control group was a contemporaneous control taken from medical records, which is a potential source of bias. Additional limitations, although not directly related to the main outcome of BMI, were the use of parent report for child's weight-related behaviors, and the inability to assess these behaviors in the contemporaneous control condition, making it difficult to know the extent to which changes may have been related to demand characteristics of participating in the intervention. Also, data were only collected for 3 months and non-English-speaking families were not included, limiting the ability to speak to longer-term outcomes and to the generalizability of the intervention in these families. Last, only 30% of eligible patients were referred. The low rate can be partially attributed to acute care appointments with nonprimary providers. Strengths of the study included the high proportion of participating parents completing all six sessions of the counseling intervention, high levels of parent and provider acceptability of the program, and exceptional retention of families in the trial.
Future Research
Given the positive findings in the pilot study, the FITLINE program warrants further investigation in a larger, longitudinal, randomized, controlled, multisite trial with a rigorous control condition. Data should be collected over 18 months, and multiple sites are needed to eliminate potential environmental confounders. Though parent participation rates are in line with clinic-based studies, two thirds of eligible families were not referred to the FITLINE counseling program; future research should explore changes to the practice component of the FITLINE program that will increase referral rates to the FITLINE counseling to improve the reach of this promising program.
Conclusions
Youth obesity is an epidemic with significant potential health, economic, and financial consequences.33–35 A portfolio of resources for parents of children who are overweight and obese—environmental and social changes, as well as online, telephone, and face-to-face support—will be required to combat pediatric obesity. Telephone-based interventions have been proven cost-effective in treating another intractable condition: smoking; thus, this medium warrants further investigation for tackling youth obesity. The success of the pilot of the FITLINE merits further investigation in a large-scale, randomized, controlled clinical trial to assess its efficacy. With provisions within the Affordable Care Act committed to prevention, strong evidence from such a randomized, controlled trial would provide support for making this type of counseling reimbursable for families. Should the intervention be proven effective, it would represent a major boost in the prevention and treatment of obesity in youth, leveraging existing AAP support for pediatric obesity referrals, telehealth infrastructure, and benefit plans that include coverage and payment for the assessment, evaluation, and treatment of pediatric obesity. 30
Footnotes
Acknowledgments
The authors gratefully acknowledge the pediatric providers and staff who took part in this study. Their deepest appreciation also goes to the families who graciously agreed to participate in this study and to share their comments and suggestions to further refine the FITLINE program.
Author Disclosure Statement
No competing financial interests exist.