
Abstract
Abstract
Background:
Maternal prepregnancy obesity (BMI ≥30 kg/m2) and excessive gestational weight gain (GWG) have shown a strong positive association with a higher BMI and risk of obesity in the offspring. The aim of this study is to estimate the effect of a GWG restriction program for obese pregnant women on the children's BMI at 5 years of age and weight-for-length/height (WL/H) development from 2 months of age until 5 years of age.
Methods:
This was a follow-up study of 302 children (137 children in an intervention group and 165 children in a control group) whose mothers participated in a weight gain restriction program during pregnancy.
Results:
BMI at five years of age did not differ between girls and boys in the intervention and control group. The degree of maternal GWG, <7 kg or ≥7 kg, did not affect the offspring's WL/H. Compared with Swedish reference data, just over half of the children in both the intervention and control group had a BMI within the average range, whereas slightly more than one-third of the children had a higher BMI.
Conclusion:
Despite a comprehensive gestational intervention program for obese women containing individual weekly visits and opportunity to participate in aqua aerobic classes, there were no differences between BMI or weight development among the offspring at 5 years of age in the intervention and control group.
Introduction
Obesity (BMI ≥30 kg/m2) in pregnancy poses a high risk for complications during pregnancy and childbirth (e.g., gestational diabetes mellitus, caesarean delivery, and macrosomia).1–3 Excessive gestational weight gain (GWG) may further worsen the situation for both the mother and the neonate.4,5 Maternal prepregnancy obesity and excessive GWG have shown a strong positive association with a higher BMI and risk of obesity in the offspring.6–9 Also, childhood obesity may result in adverse outcomes later in life.9–11
In studies carried out in Finland, the effect of an intervention undertaken during pregnancy or in early postpartum on the offspring's weight gain during the first four years of life was examined.12–14 The intervention given during pregnancy was not effective in slowing children's weight gain until 4 years of age, whereas the intervention given postpartum showed a slower increase of standardized z-score of weight-for-length/height (ZWL/H) and standardized z-score of BMI (ZBMI) for children in the intervention group compared with a control group.
We have in previous studies shown that an intervention program designed to restrict the GWG to <7 kg was effective among obese pregnant women.15–17 The women in the intervention group gained less weight during pregnancy and had a lower weight at the follow-up assessments two and six years after childbirth, compared with the women in the control group. The aim of this study was to estimate the effect of a GWG restriction program for obese pregnant women on the children's BMI at 5 years of age and weight-for-length/height (WL/H) development from 2 months of age until 5 years of age.
Methods
The study groups comprise children of obese pregnant women who participated in an intervention study during 2004–2006 at the antenatal care clinic (ANC) in Linköping. A control group of obese pregnant women was recruited from the ANCs in two nearby cities. The original study and the follow-up studies are described elsewhere and summarized briefly below.15–17 The intervention program consisted of individual weekly visits during pregnancy and every six months during the first two years after childbirth, with a specially trained midwife aiming to change behaviors regarding nutrition and physical activity. The participants were also invited to join aqua aerobic classes especially designed for obese women. A total of 155 women (67.4%) completed the intervention program. The control group consisted of 193 pregnant obese women who followed the routine program at the ANCs. All women were recruited and included in the study in early pregnancy, i.e., before gestational week 15.
In Sweden all families are offered preventive health care for their children throughout childhood and youth. The preventive health care program is free of charge and reaches almost 100% of all children. 18 At the child welfare center (CWC) and the pupil health care center, children are advised to attend the regular health program (weight- and length/height development, physical health, immunizations, cognitive and linguistic development).
Subjects
A description of the population in the original and follow-up studies is displayed in Figure 1. Mothers (n = 343) from the original study were sent a letter with information about the follow-up of their children. Parents of 138 children agreed to participate in the follow-up study and 166 from the control group. In the former group one child was excluded because of genetic disorder (Down syndrome). Parents of nine children refrained from participation. Thus 137 children (89.0%) from the intervention group took part in the follow-up study. In the latter group one child was excluded because of disability (delayed physical and mental development) and one woman could not be reached. Nineteen parents refrained from participation, thus 165 children (85.5%) from the control group participated in the follow-up study.
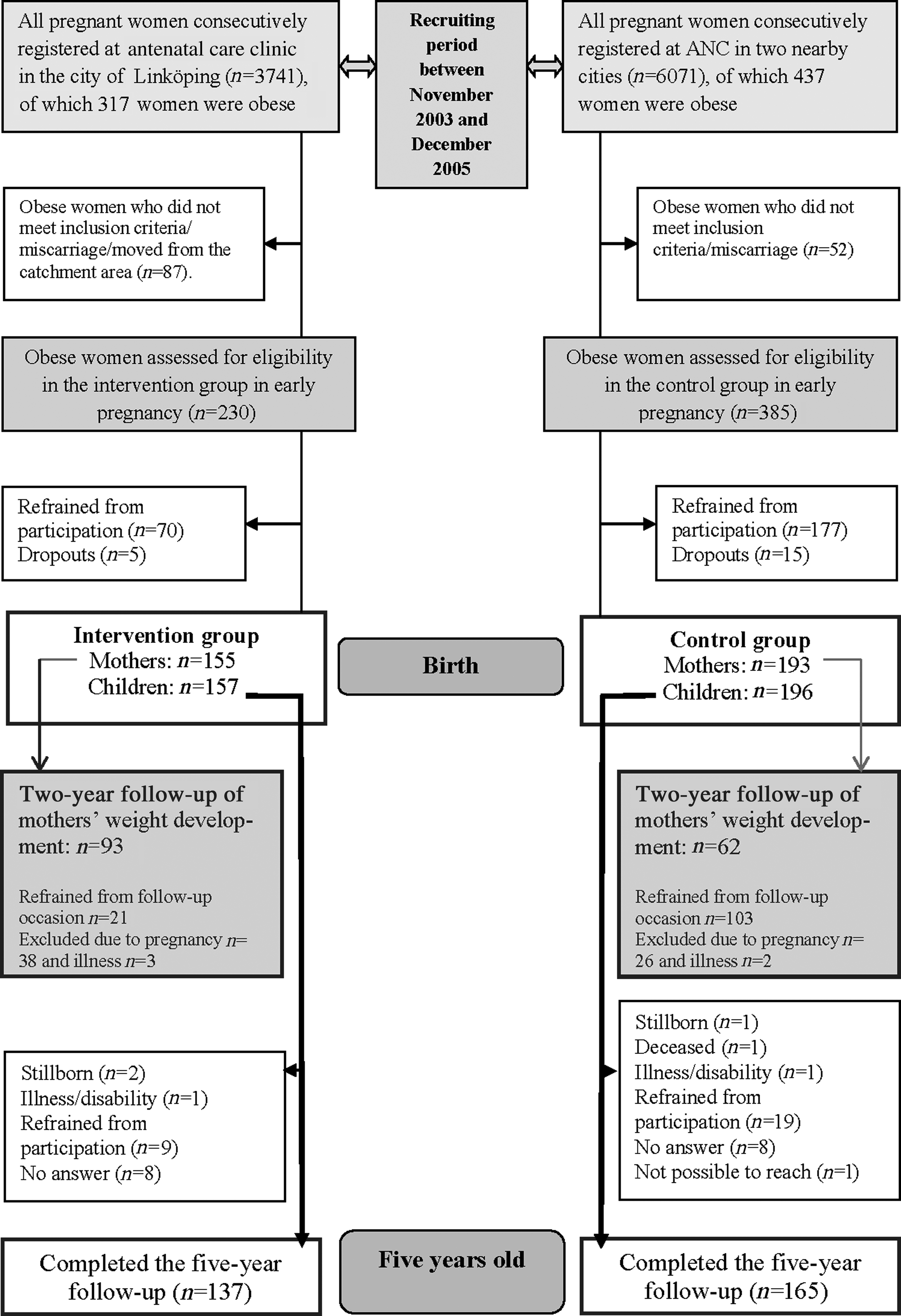
Description of the population in the original and follow-up studies.
Data Collection
Data were manually extracted from the records by the main author (IMC): weight and height at 2, 6, 12, and 18 months of age and at 4 and 5 years of age. Information about illness, disability, parental smoking habits, and breastfeeding were also obtained. Maternal and children's background characteristics were obtained from antenatal, delivery, and neonatal records.
Statistics
All analyses were performed using SPSS 22.0 (IBM, Armonk, NY). Statistical significance was defined as (two-sided) p ≤ 0.05. Before analyzing the weight changes, the assumption of these variables being normally distributed was validated using the Kolmogorov-Smirnov test. This assumption was not confirmed. The Mann Whitney U-test was therefore used as the method of analysis on all continuous variables. Group differences were estimated by using the Pearson's chi-square test and Fischer's exact test on categorical variables. To make a more comprehensive assessment of group differences, linear regressions were performed with BMI at 5 years of age as dependent variables. The size of the child was analyzed using weight and length/height. The value was converted to WL/H and its standard score (z-score) was used. The child's BMI at 5 years of age was analyzed with respect to BMI reference values, expressed in mean and standard deviation, for Swedish children. 19
Ethics
All parents have given informed consent. The study was approved by the regional ethical review board in Linköping, Sweden (Dnr 2010/400-31).
Results
Maternal and children's characteristics are displayed in Table 1. A greater percentage of children in the intervention group had been breastfed at some time during infancy than those in the control group (p = 0.013). For the participants in this follow-up there was also a significant difference in GWG (p > 0.001 and p = 0.005).
Maternal and Children's Characteristics in the Intervention and Control Group a
All values are given as frequencies unless otherwise stated.
Missing data are not included in the analyses.
Age at childbirth.
Mann-Whitney U test.
BMI in early pregnancy.
Pearson's chi-square test.
Fischer's exact test.
Only women with simplex pregnancies are included. Weight registered in the same week as the delivery. If this value was missing, the weight was measured 1 or 2 weeks before the delivery.
The children's BMI and ZBMI at 5 years of age and also in relation to maternal GWG are displayed in Table 2. There were no differences between girls and boys in the intervention and control groups, except among boys whose mothers gained <7 kg during the pregnancy. Boys in the intervention group had a lower BMI than boys in the control group (p = 0.039). However, the significant difference disappeared after adjusting for sociodemographic factors and breastfeeding (p = 0.407). The children's BMI was also analyzed with respect to national reference data. Slightly more than half of the children in both the intervention and control group had BMI that fell within the average range, whereas just over one-third of the children had higher BMI (Table 3).
BMI and ZBMI for Girls and Boys in the Intervention and Control Group
Mann Whitney U-test.
Only women with simplex pregnancies are included. Weight registered in the same week as the delivery. If this value was missing, the weight was measured 1 or 2 weeks before the delivery.
After adjusting for sociodemographic factors and breastfeeding, p = 0.407.
Distributions of BMI Values among Girls and Boys in the Intervention and Control Group at 5 Years of Age According to BMI Reference Values (Mean and SD) for Swedish Children
Chi-square test.
The distributions of standardized scores of WL/H among boys and girls belonging to the intervention and control group, from 2 months of age until 5 years of age, are displayed in Figure 2. There were no differences in ZWL/H development among boys and girls in the two groups.

Distribution of standardized scores of weight-for-length/height from 2 months of age until 5 years of age among boys and girls in the intervention and control group.
Discussion
In this follow-up study we found that by comparison with Swedish reference data more than one-third of the children, irrespective of gender or group, had a BMI indicating overweight or obesity. The prevalence of overweight and obesity among 4-year-old Swedish children in two different Swedish districts was in year 2014 10.6% and 2.2%, respectively. 20 We found no difference between the children in the intervention and control groups in BMI at 5 years of age or in WL/H development during the first five years of life in relation to GWG of the mother.
We found no crucial differences concerning BMI and development of WL/H during the first five years of life between the children in the intervention and control group. But for the women, the intervention had a positive effect on GWG and their own weight development six years after participation in a weight gain restriction program.15,17 We expected that the mother's change to healthier lifestyle habits during pregnancy would have influenced her child's weight development during childhood; however this was not evident in this study.
Whereas the original study had a high level of statistical power to detect difference in maternal GWG, this follow-up study could not, despite a high rate of participation, reach the same level. Significantly more participants might have been needed to demonstrate a difference. One can also speculate about whether a continued comprehensive intervention program at the CWC designed to support the newly formed family in establishing new habits would give a different result.
Furthermore, from another point of view, it may be desirable to examine if genetic as well as epigenetic factors transmitted from the parents to the offspring might be involved at the moment of conception. In a recent study on fruit flies it was shown that paternal sugar intake elicits obesity in offspring. 21 The interpretation of the findings from this fruit fly study was that the epigenetic memory is created very early in fruit flies, probably at the moment of conception. This insight indicates that one should consider the need for prepregnancy counselling for obese women as well as men. Also, findings in a clinical study emphasize the importance of maintaining a healthy weight during the reproductive years. 22 The results also showed that a greater maternal prepregnancy weight was associated with obesity among the children. The mothers GWG, i.e., < 7 kg / ≥ 7 kg, had no impact on the BMI of the offspring in our study. This result is in contrast to findings in the British study, 22 which found that offspring of women with GWG above the Institute of Medicine (IOM) recommended level 23 were more likely to have a greater BMI. The same study also showed that any maternal weight gain during the first 14 gestational weeks was associated with increased obesity in offspring, whereas only maternal GWG >500 g/w between gestational week 14 and 36 was associated with obesity in offspring.
Mustila and coauthors in Finland have in two studies encompassing women in different BMI classes investigated the effect of gestational and postpartum lifestyle counselling on the offspring's weight gain.12,14 In the first four-year follow-up study they demonstrated that among the offspring in the intervention group and the control group there was no difference in the increase of ZBMI or ZWL/H until the age of 4 years. 12 This result differs from the result in the second four-year follow-up study among mothers with infants at the age of 2–10 months who participated in an intervention postpartum. 14 The increase of ZBMI and ZWL/H between 2 and 4 years of age was slower among the offspring in the postpartum intervention group than in the control group. 14 In a recent Danish follow-up study of a gestational intervention program for obese women, no ZBMI differences at 3 years of age were detected between the intervention and control groups. 24 These results from studies designed as a gestational lifestyle counselling program are in line with our results. On the other hand the results from the Danish study 24 intended to give postnatal lifestyle counselling differ from our findings. The women in the intervention group in the present study were offered, in addition to the gestational intervention program, an individual visit every six months during the first two years after childbirth in order to discuss behavior regarding nutrition and physical activity.
An association between maternal BMI and/or GWG and the BMI of offspring have been investigated in some large cohort studies.25–27 A Norwegian study found a positive association between both maternal prepregnancy BMI and GWG and the mean BMI of the offspring at 3 years of age. 25 Similar results are reported in a European study that investigated ante-, peri-, and postnatal risk factors on risk of obesity in children at 4 and 8 years of age. 26 GWG >25 kg posed after adjustment a twofold risk of obesity for the offspring. A German study encompassing data of mother-child dyads showed an association between abdominal adiposity among 6-year-old children with prepregnancy obese mothers and continuous GWG. 27 On the other hand, when GWG was used as a categorical variable, i.e., 5–9 kg according to the GWG recommendation of the IOM for obese women, no association was found.
There are weaknesses as well as strengths in this study. It is possible that a longer follow-up period could indicate more distinct differences in weight and BMI trends. Another weakness is the lack of randomization of the original intervention study. The strength in this case control study was that we had a participation rate of more than 85% in both study groups. To our knowledge this study is one of few that concerns results from a follow-up of BMI and weight development among offspring of mothers attending a GWG restriction program.
In conclusion, despite a comprehensive gestational intervention program, no differences in BMI or weight development at 5 years of age were observed among the offspring. Prevention against obesity is still an important task. CWCs, family planning centers, and preconception counsellors need to focus on information about the importance of a healthy lifestyle in order to prevent obesity.
Footnotes
Acknowledgments
This study was supported by grants from The Health Research Council of the Southeast of Sweden and the County Council of Östergötland.
Author Disclosure Statement
None of the authors report any conflict of interest or specific funding.