
Abstract
Abstract
Background:
Picky eating and food neophobia are common during childhood. Childhood eating behaviors are often predictive of adult eating behaviors.
Objectives:
Determine if childhood picky eating or food neophobia is associated with childhood weight status, or with becoming underweight, overweight, or obese later in childhood.
Data Sources:
We identified relevant studies from searches of PubMed, PsycINFO, and NEOHAL, as well as citations from identified studies.
Study Eligibility Criteria and Participants:
Inclusion criteria were original research articles examining a relationship between picky eating and/or food neophobia with childhood weight status. We summarized definitions and prevalence of picky eating or food neophobia and association with weight status.
Study Appraisal:
Two independent investigators assessed bias and confounding using the Agency for Healthcare Research and Quality's RTI Item Bank.
Results:
Forty-one studies met inclusion criteria. Picky eating was defined inconsistently, and a large variation in prevalence was found (5.8%–59%). Food neophobia was consistently defined as an unwillingness to try new foods, with a prevalence between 40% and 60%. No association existed between childhood weight status and food neophobia, and results were unclear for picky eating.
Limitations:
Risk of bias and confounding were moderate. Parental report was commonly used to assess picky eating, height, and weight and parental weight, feeding styles, and community characteristics were infrequently considered.
Conclusions and Implications:
Heterogeneous definitions used for picky eating led to a wide range of reported prevalence and an unclear relationship with weight. Consistent definitions and an improved understanding of such a relationship could help clinicians provide appropriate anticipatory guidance.
Introduction
Parents commonly express concern that their children are poor eaters. As a feature of normal development, most children experience a reduction in appetite 1 and a decreased rate of growth2,3 between 2 and 6 years of age. Food preferences are typically established during toddlerhood, although toddlers' preferences for certain foods may vary significantly on a weekly or even a daily basis. 4 Young children may need to try a novel food as many as 15 times before they will accept it as a component of their normal diet. 5 Picky or fussy eating is often defined as eating a limited variety of foods. As the terms are often used interchangeably, we will use the term picky eating to also refer to fussy eating, food fussiness, and selective eating throughout this article.4,6 Food neophobia, the fear/hesitation of eating new or novel foods, is often considered to be one specific component of picky eating. 4 Given that picky eating and food neophobia are conceptualized based on a spectrum of behaviors 6 and nearly all children experience picky eating or food neophobia to some degree, 7 it is not well understood to what extent these behaviors affect weight status later in life.
It is well established that childhood eating behaviors predict adult eating behaviors,8,9 and children who are overweight or obese are more likely to be overweight or obese in adulthood compared to their normal weight counterparts. 10 Some evidence suggests that picky eaters who do not consume sufficient calories may become underweight.11,12 However, parents may also compensate for children's pickiness by pressuring their child to eat or by offering foods their children may find more acceptable, such as calorie-dense foods, which may inadvertently increase the risk for obesity.
While there are reports of picky eating and food neophobia in the obesity literature, 13 it remains unknown whether picky eating during childhood plays a role in determining weight trajectory or future weight status. This systematic review seeks to determine if the presence of picky eating or food neophobia behaviors during childhood is associated with childhood weight status or with becoming underweight, overweight, or obese later in childhood or adolescence. We hypothesize that children reported to be picky eaters are at a higher risk for becoming overweight or obese as older children and adolescents, likely due to a preference for calorie-dense foods and decreased intake of fruits and vegetables. In addition, we describe the various definitions and reported prevalence of picky eating and food neophobia.
Methods
This systematic review was conducted and reported as per the guidelines from PRISMA (preferred reporting items for systematic reviews and meta-analyses) (see Supplementary Table S1 available online at www.liebertpub.com/chi). 14 The protocol for this review was registered with PROSPERO (registration number CRD42015027830), the international prospective register for systematic reviews (www.crd.york.ac.uk/PROSPERO).
Search Strategy
We chose studies by searching electronic databases and article reference lists. We searched PubMed, PsycINFO, and NEOHAL without study design, article type, or publication status restrictions. Studies were included if published in English from January 1, 1990, through November 2, 2015, and if studies reported results on children (aged birth–18 years). We searched databases for the terms picky eating, food neophobia, food fussiness, fussy eating, or selective eating, and these terms were cross searched with the terms weight, overweight, underweight, body weight, and obesity. The last search was completed on November 2, 2015. The details of search terms used are available in Table 1.
Search Strategy
Eligibility Criteria
A single investigator (C.L.B.) compiled search results, screened titles and abstracts, and removed duplicates to identify studies relevant to the objectives of this review. Abstracts were not included if studies evaluated the following: nonhuman subjects, adult subjects exclusively, only children with developmental delays or autism, taste acuity, eating disorders (such as anorexia nervosa or bulimia nervosa), digestibility, or prenatal exposures. Two authors (C.L.B. and G.M.C.) then independently reviewed the full manuscripts of the remaining articles. Studies were included if they examined children's weight and its relationship to picky eating or food neophobia. A third author (J.A.S.) resolved any discrepancies. The study selection process is presented in Figure 1.
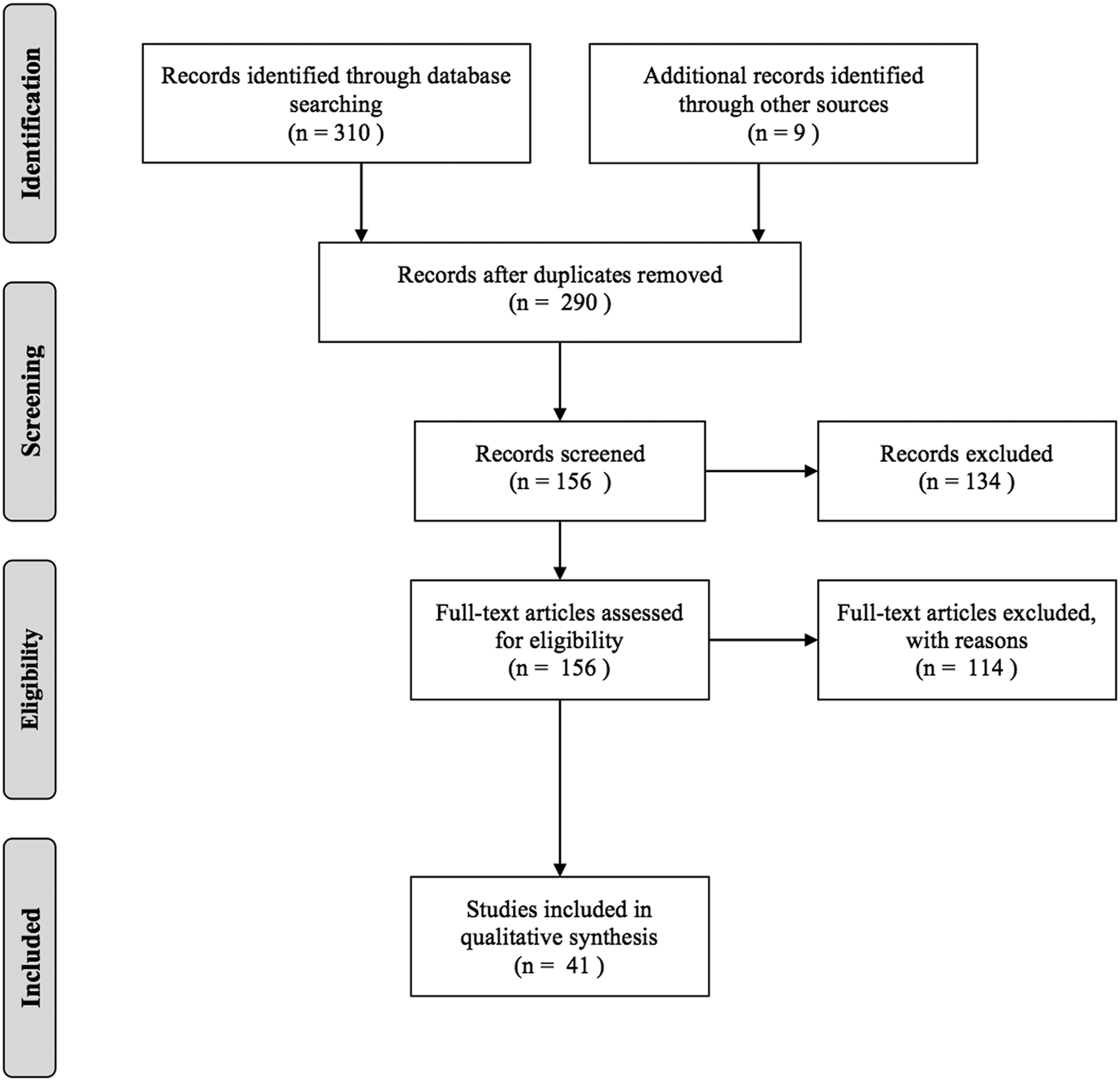
Systematic review search results.
Data Extraction
Data extraction was performed by two authors (C.L.B. and G.M.C.), and the following information was extracted: study design, age of subjects, sample size, definition of picky eating, prevalence of picky eating or food neophobia, method of prevalence measurement, method of obtaining anthropometrics, and relationship of picky eating or food neophobia to weight.
Subgroup Examination
Given that picky eating is a common feature of early childhood and this developmental period typically is characterized by a brief reduction in BMI, it is necessary to distinguish results of studies, including toddlers and young children from those including older children. Doing so may help determine if a decrease in BMI associated with picky eating is actually attributable to normal fluctuations in child weight status. Therefore, we examined separately studies containing children aged six or older from studies containing children younger than 6 years old. In addition, we qualitatively considered relationships by study type (longitudinal, cross sectional, or case–control); parental report vs. measured height or weight; questionnaire type; and picky eating severity.
Study-Quality Assessment
Two investigators (C.L.B. and E.B.V.) independently determined risk of bias and confounding. As all included studies in this review were observational, bias was assessed using the Agency for Healthcare Research and Quality's RTI Item Bank to Assess Risk of Bias and Confounding. 15 In addition, bias that may affect the cumulative evidence was considered. Studies used inconsistent definitions of picky eating with quite a variable prevalence. This limited the ability to combine weight status outcome data for meta-analysis.
Results
The electronic database search yielded 310 results. Nine additional abstracts were obtained through reviewing reference lists. Duplicates were removed and 290 abstracts were screened. Based on a priori exclusion criteria, 134 abstracts were excluded, and the remaining 156 full-text articles were assessed for eligibility. Of these, 41 met inclusion criteria and were included in the review (Fig. 1).
Study Characteristics
Characteristics of the 41 studies included in analysis are summarized in Table 2. Of the studies included in analysis, all were observational; 31 were cross-sectional, 9 were longitudinal, and 1 was case–control. Participant age ranged from 4 months to 17 years. Sample size varied from 32 to 4987.
Characteristics and Main Findings of Included Studies
BMIz, body mass index z-score; CEBQ, Child Eating Behavior Questionnaire; CFNS, Child Food Neophobia Scale; CFQ, Child Feeding Questionnaire; CPEBQ, Chinese Preschoolers' Eating Behavior Questionnaire; EBQ, Eating Behavior Questionnaire; FF, food fussiness; FN, food neophobia; ORI-CEBI, Oregon Research Institute Child Eating Behavior Inventory; PE, picky eating; SD, standard deviation; SFQ, Stanford Feeding Questionnaire; WFA, weight for age; WFL, weight for length.
Definitions and Prevalence of Picky Eating and Food Neophobia
All studies relied on parental report to determine the presence of picky eating and food neophobia, although one study used referral to a feeding clinic (based on parental report of picky eating behaviors) to define case inclusion 12 and another study also tested food acceptance by giving children yogurt with a variety of textures, colors, and tastes. 16 Studies determined the presence of picky eating through the following methods: directly asking parents if their children were picky eaters,17–24 administering questionnaires,11,13,16,19,20,25–52 and referral of children to a specialty feeding clinic for picky eating behaviors. 12 Standardized questionnaires that were used to evaluate picky eating included the Child Eating Behavior Questionnaire (CEBQ), Child Feeding Questionnaire (CFQ), Stanford Feeding Questionnaire (SFQ), Eating Behavior Questionnaire (EBQ), Picky Eating Scale modified from Pelchat and Pliner, Oregon Research Institute Child Eating Behavior Inventory (ORI-CEBI), and Chinese Preschoolers' Eating Behavior Questionnaire (CPEBQ).
Questionnaires asked an array of questions to assess picky eating behaviors, including eating a limited variety of foods, preparing foods in a specific way, slow eating, and low enjoyment of food. The two most commonly used questionnaires were the CEBQ (n = 16) and the CFQ (n = 4). The CEBQ contains a food fussiness subscale, which assesses a child's dietary variety, difficulty pleasing with meals, and refusal of new foods. Studies using the CFQ examined three questions relating to pickiness: diet consisting of only a few foods, child unwilling to eat many foods that the family eats, and child is fussy or picky about what he/she eats. Those studies utilizing nonstandardized questionnaires of picky eating relied on parents to report common signs of picky eating (i.e., eating different meals from the rest of the family, refusing to eat certain foods, refusing to try new foods) to determine if children were picky. All studies that examined food neophobia (n = 7) did so using the Child Food Neophobia Scale (CFNS), a measure assessing a child's willingness to try new foods.
Some studies (n = 4) did not provide a clear definition for picky eating,17–20,22 leaving parents to interpret whether their children were picky eaters based on their own criteria. Of the studies that did include a explicit definition of picky eating, these definitions included the following: “unwillingness to eat familiar foods or try new foods, severe enough to interfere with daily routines to an extent that was problematic to the parent, child, or parent-child relationship” 12 ; whether a child “eats everything” 27 ; “the unwillingness to try many different, already familiar, foods” 13 ; and consuming “an inadequate variety and amount of foods through rejection of foods that are familiar.”23,24 Food neophobia was universally defined as “an unwillingness to eat novel foods.” 13
The prevalence of picky eating varied widely from 5.8% to 59% and the prevalence of food neophobia ranged from 40% to 60%. Table 2 describes an overview of study methods and the reported prevalence of picky eating or food neophobia.
General Findings
Of the 41 studies reviewed, 17 found no association between picky eating or food neophobia and weight status16,17,19,20,25,26,30,34,36,40–42,45,47–49,51; 2 found that picky eating or food neophobia had a positive association with overweight13,39; 5 found a negative association with overweight or obesity27,28,32,46,53; 6 found a positive association with underweight11,12,21,31,35,50; and 11 found a decreased association with BMI or BMI z-score (but did not specify if underweight or decreased risk of overweight)18,22–24,29,33,37,38,43,44,52 (Table 2). These results are depicted in Figure 2.

Association of picky eating or food neophobia with weight: all studies from systematic review (N = 41).
When picky eating and food neophobia are examined separately, results of studies examining picky eating continue to be disparate (Fig. 3). In contrast, of the seven studies examining food neophobia, there is more consistency, with six studies finding no association and one study finding a positive overweight (Fig. 3).
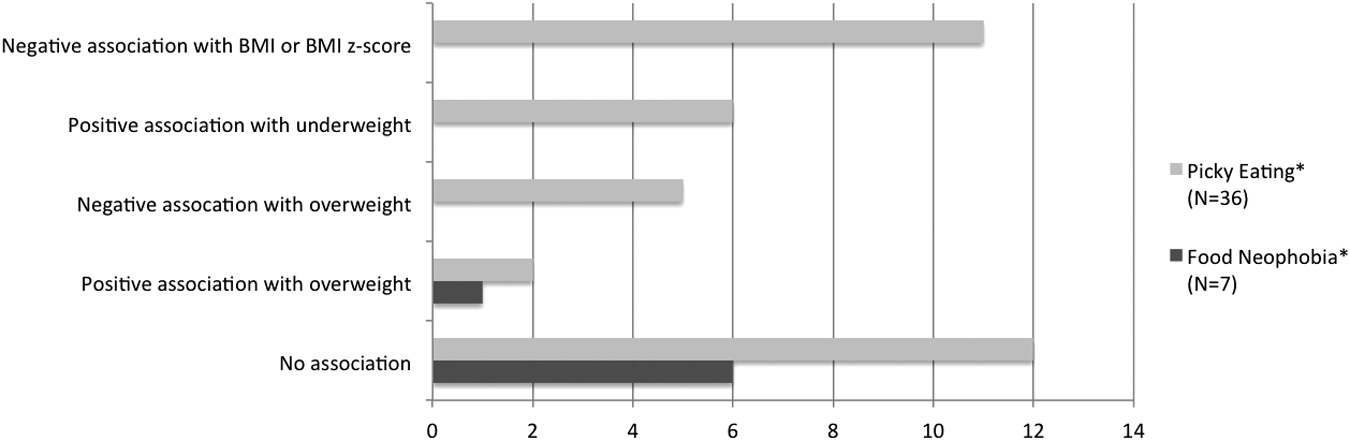
Association of picky eating (N = 36) and food neophobia (N = 7) with weight. *Two studies examined both picky eating and food neophobia.
Twenty of the 41 identified studies reviewed here included children 6 years old or older. Seven of these found no association between picky eating or food neophobia and weight status; two found a positive association with overweight or obesity; five found a negative association with overweight; two found a positive association with underweight, and four found a negative association with BMI or BMI z-score (Fig. 4). Of the 21 studies, including children younger than 6 years of age, 10 of these found no association between picky eating or food neophobia and weight status; 4 found a positive association with underweight, and 7 found a negative association with BMI or BMI z-score (Fig. 4).
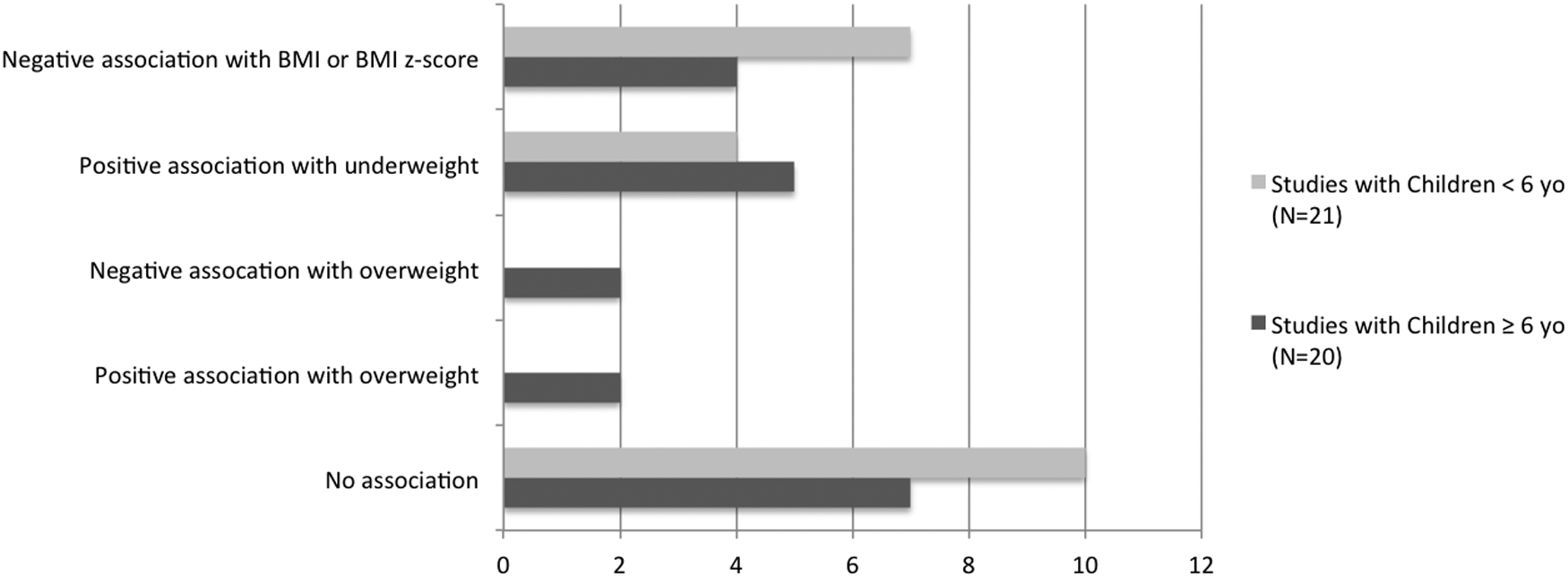
Association of picky eating or food neophobia with weight, by age.
No clear relationship was found between picky eating or food neophobia and weight status based on type of study (9 longitudinal, 31 cross sectional, and 1 case–control) or whether anthropometrics were obtained via parent report or directly measured. When studies were examined based on the type of questionnaire used, 16 studies assessed food fussiness with the CEBQ, 7 studies assessed food neophobia with the CFNS, 4 studies assessed picky eating with the CFQ, 2 studies assessed picky eating with the SFQ, and 6 studies asked parents directly whether the child is a picky eater. There was no clear relationship between picky eating and weight status based on the questionnaire type. When examining severity of picky eating, only three studies classified children as severe (e.g., referred to a feeding specialist) or persistent (e.g., for 3 years in a row) picky eaters, and all of these studies found increased odds or proportion of underweight status among severe picky eaters.12,17,24 In addition, the studies of severe picky eaters had lower prevalence estimates (10%–21%) than most of the studies not examining severe picky eaters.
Strength of the Evidence
All studies in this review are observational and many were rated as having at least medium risk of bias (Table 3). All studies were at risk for bias due to their reliance on parental report to define picky eating or food neophobic behavior, as child weight status could potentially influence parental perceptions of children's eating behaviors. For example, parents might be more likely to describe an underweight child as a picky eater compared to a child with normal weight, independent of actual eating behavior, as a means of justifying the former child's low-weight status. Conversely, parents of a child with overweight may justify offering more high calorie, palatable foods if they believe the child is a picky eater. Different means of determining picky eating status may therefore contribute to risk of bias and variability in results across studies. Furthermore, many studies solicited parent report of child height and weight (rather than direct measurements), which is known to often be incorrect, resulting in weight status misclassifcation. 54
Risk of Bias and Confounding of Included Studies
As determined by the Agency for Healthcare Research and Quality RTI Item Bank, 15 an item was low risk of no affirmative answers, medium risk if one affirmative answer, and high risk if more than one affirmative answer.
Bias = Q 1,3,7,8,9,11.
Confounding = Q 6,12,13.
Most studies attempted to correct for potential confounders such as demographics, family income, and parental education. However, many other important factors were often missing, such as parental weight status, feeding styles, and community characteristics, which led to at least a medium risk of confounding in most identified studies. When studies with high risk for bias (n = 1) or confounding (n = 6) were excluded from analysis, results did not differ (results not shown, please see Tables 2 and 3 for additional details).
Discussion
No clear association can be determined between childhood weight status and picky eating among the 41 studies included in this systematic review. Our findings indicate a wide range of conflicting evidence, with results ranging from “no association” between picky eating and weight status, to associations with either overweight or underweight. In addition, results of some individual studies were mixed, with varying associations found depending on baseline BMI, 32 gender, 19 or the persistence of picky eating.11,24 Definitions of picky eating varied significantly between studies, varying from parental report of “is your child a picky eater?” to referral to a subspecialist due to picky eating behaviors that interfered with daily routines. These inconsistencies in the conceptualization and measurement of picky eating contribute to the large discrepancies in reported prevalence of picky eating and association with weight. In contrast, food neophobia was consistently defined as a fear of trying new foods and was measured in each study using the CFNS. 55 This resulted in more narrow prevalence estimates (40%–60%) and a more consistent finding of no association with food neophobia and weight status.
Most of the studies in this review were cross-sectional, preventing the ability to infer causal relationships. It is especially important to note that the odds ratios are not comparable in magnitude across study designs—for example, one study finding that overweight kids are five times as likely to be picky does not mean that picky kids are five times as likely to be overweight. Even in studies that found a relationship between picky eating and overweight, it is not possible to determine if picky eating behaviors predisposed children to overweight, if the overweight preceded picky eating, or if another confounding factor is responsible for both. Also, most studies did not clearly report possible effect modifiers (e.g., types of foods offered to the child, parenting styles, parent weight status) that could affect the relationship between eating behaviors and weight status. Other limitations that may affect the cumulative evidence in this systematic review include publication bias and the risk of selective reporting within studies. As null articles may be less likely to be published, the category of studies reporting “no association” is probably underrepresented.
Although 20 studies in this review included children older than 6 years old, only three of these were longitudinal studies, and none of the longitudinal studies followed children beyond 11 years old. A growth velocity nadir occurs in children between 2 and 6 years old, which is then followed by a period of adiposity rebound (the period during which BMI increases from its nadir). 56 Children who experience adiposity rebound at earlier ages are at higher risk for increased BMI during adolescence 57 ; thus, accounting for adiposity rebound in study designs is crucial in the interpretation of findings regarding the cross-sectional association between childhood eating behaviors and weight status, and to our understanding of how early childhood eating behaviors influence weight trajectories over time. Longitudinal studies with longer follow-up periods are needed to assess picky eating behaviors and weight during a child's growth velocity nadir, adiposity rebound, and then into adolescence, to better understand how these behaviors affect long-term growth trajectories. In addition, longitudinal studies should adjust for baseline BMI or BMIz in their analysis, as this was not commonly done by studies in this review. In the case of Rodenburg et al., 48 there was an overall negative association between food fussiness and BMIz (beta = −0.08, p < 0.01); however, when baseline BMIz was adjusted for, this association was no longer significant.
Our finding that severe or persistent picky eating is associated with increased odds of underweight suggests that these studies are describing different eating behaviors than many of the other studies A recent review article by Kerzner 58 describes a new classification of feeding problems commonly described in children and a systematic approach to management that incorporates severity of feeding problems and parent feeding style. Kerzner describes feeding problems as a pyramid, with “feeding disorders” at the top as the most severe, followed by “milder feeding difficulties,” “misperceived feeding problems,” and finally “normal” at the bottom of the pyramid. Although this conceptualization nicely distinguishes categories of child feeding behaviors by severity and consequences, there remains a need for more universally accepted definitions of picky eating as well as a determination of where certain eating behaviors should be classified within Kerzner's pyramid. This information would indeed help clinicians in appropriately classifying pediatric patients and providing counsel for parents.
The existing literature supports that food neophobia is common in children and does not put children at increased risk for being underweight. The longitudinal studies in this review do not show consistent relationships between pickiness and weight status, likely due to inconsistent definitions. A more recent longitudinal study published after our search 59 narrowly defined picky eating by incorporating several CEBQ subscales, with a resulting group representing <6% of the population, and found that picky eating increases the risk of underweight. However, given the variety of available definitions for picky eating, it is unclear if this finding would stand up for all. A more uniform definition of picky eating and a better understanding of the pathology of picky eating in various age groups are needed to clarify this literature. Further research also is warranted to examine how picky eating affects the timing of the BMI nadir between 2 and 6 years old, and subsequent adiposity rebound. In addition, more information is needed regarding the role of environment as a determinant of parents' and children's food preferences and whether these environmental influences are responsible for maladaptive nutrition practices during childhood.
Conclusions
No consistent definition exists for picky eating throughout the literature. This has, in turn, led to very different conclusions regarding the prevalence of picky eating and whether picky eating may affect current or future weight status. The relationship between picky eating and weight has significant clinical implications, as parents' concerns about picky eating may potentially change how they feed their children. This may increase the frequency of pediatric medical visits and also may lead to disagreements between caregivers regarding management of children's eating behaviors. If uniform definitions of picky eating are established and if picky eating is then shown to have no association with weight status, then physicians and parents may be able to reduce related anxiety and interventions. Should additional evidence show that such traits are predictive of children's weight trajectories, primary care providers should prioritize anticipatory guidance and counseling about management of picky eating behaviors. Equipped with definitive empirical evidence regarding the role of picky eating in determining childhood weight trajectories, pediatricians and childhood healthcare providers can better support parents and children in transitioning from picky eating to appropriate self-regulation of childhood nutrition behaviors.
Footnotes
Acknowledgment
The authors thank the NRSA fellows at UNC Chapel Hill for their helpful review of the article.
Supported, in part, by a grant from NICHD/NIH Mentored Patient-Oriented Research Career Development Award K23 HD061597 (J.A.S.) and from the Health Resources and Service Administration National Research Service Award (NRSA) grant T32 HP14001 (C.L.B. and E.B.V.). These funding agencies had no role in the design and conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript. This information or content and conclusions are those of the author and should not be construed as the official position or policy nor should any endorsements be inferred by HRSA, HHS, or the US Government.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.