
Abstract
Abstract
Objective:
The study's objective was to analyze the association between the adherence to the Mediterranean diet (MD) and the presence of nonalcoholic fatty liver disease (NAFLD) in children.
Methods:
The study consisted of three groups of children. Group 1 included obese/overweight children with recent diagnosis of NAFLD (n = 106, 12.4 ± 2.6 years). Group 2 included obese children without NAFLD (n = 21, 11.3 ± 2.6 years). Group 3 included the healthy children (without known chronic disease) with normal BMI (n = 54, 11.8 ± 2.9 years). Compliance to the MD was assessed by the KIDMED index score.
Results:
KIDMED index score in obese children with NAFLD, without NAFLD, and healthy children were 2.6 ± 2.4, 4.6 ± 1.2, and 6.2 ± 1.9, respectively (p < 0.05 for group 1 versus 2, 1 versus 3, and 2 versus 3). Diet compliance was good in only 4.7% of the patients with NAFLD, whereas it was 31.5% in healthy children. KIDMED index score was negatively correlated with BMI (p < 0.05, r = −0.53), but no correlation was found with other parameters.
The area under the receiver operation curve (AUROC) for predicting fatty liver disease in obese children (n = 127) with BMI and KIDMED index score was 0.78 (p < 0.05) and 0.24 (p < 0.05), respectively. BMI >26 has a sensitivity of 79.2% and specificity of 52.4%, and KIDMED index score ≤3 has a sensitivity of 66.9% and specificity of 76.1%.
Conclusions:
MD is an inexpensive and nontoxic dietary regimen and may be used as a therapeutic option in obese children with NAFLD.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is a common complication of pediatric obesity characterized by altered lipid metabolism that results with macrovesicular steatosis (> 5% of all liver cells with fatty infiltration) and/or fibrosis. The clinicopathological spectrum of disease may vary from simple steatosis to cirrhosis and end-stage liver disease. 1 It is the most common cause of chronic liver disease in children and adolescents in Western countries, and one of the common indications for liver transplantation in adults in the United States. 2
Nowadays, multi-hits theory has been proposed for the pathogenesis of NAFLD. 3 In the first hit there is an accumulation of triglyceride (due to their increased synthesis or decreased export) as lipid droplets within the cytoplasm of hepatocyte. Insulin resistance (IR) is the major contributor of this hepatic steatosis. This phase of hepatic steatosis is benign and reversible but makes the liver susceptible to the second hit, which advances the liver to a necroinflammatory stage. The second hit includes oxidative stress, lipid peroxidation leading to mitochondrial dysfunction, proinflammatory cytokines, and gut-derived bacterial endotoxinemia, causes steatohepatitis and may stimulate hepatocyte death. At the end, the disease may progress to fibrosis, cirrhosis, and hepatocellular carcinoma in some patients with genetic (such as PNPLA3 and KLF-6 polymorphisms) and environmental susceptibilities on the continuous hits. 4
Genetic and environmental factors are the major responsible triggers for the development and progression of the disease. Diet composition including the type and amount of macronutrients is the major potential environmental factor affecting the risk of the disease. Increased consumption of refined sugar and saturated fatty acids increases the occurrence of NAFLD by affecting the insulin metabolism. 5
In the last decade it was shown in population-based studies that adhering to Mediterranean diet (MD) has beneficial effects on healthy life and is associated with lower incidence of cardiovascular diseases, metabolic disorders, and several types of cancers. It is an intangible cultural heritage of humanity and it is commonly used in countries bordering the Mediterranean Sea, such as Greece, Italy, and Spain. 6 It is characterized by low saturated fat and high monounsaturated fatty acid (MUFA) content, a balanced ratio of polyunsaturated fatty acids (PUFA), and omega 6 and 3; and it is rich in fibers and complex carbohydrates. It includes relatively high intake of fish, nonrefined cereals, fruits, and vegetables, nuts, and olive oil. Olive oil is the main source of calories in the MD, with high levels of MUFA and phytochemicals. Omega-3 PUFA is mainly found in fish. The MD is associated with decreased levels of glycemia, plasma triglycerides, and total cholesterol, and increased levels of high-density lipoprotein. It has high antioxidant capacity mainly due to fruits, vegetables, nuts, and olive oil. Due to its lipid profile, effects on IR, and high antioxidant capacity, MD seems to have a beneficial effect on the prevention of obesity/overweight-related NAFLD.6–8
In the Black Sea (Karadeniz) region on the south coast of the Black Sea consumption of fish and nuts that are essential nutrients in MD are high in the indigenous population (Figure 1). Anchovy, rich in omega-3, is widely consumed as a source of fish in the Black Sea region, and nuts are widely cultivated and consumed.9,10
The Black Sea (Trabzon, Karadeniz) region is on the south coast of the Black Sea.
The aim of this study is to analyze the association between the consumption of MD and the presence of NAFLD in children in the Black Sea region of Turkey. If we found an association, thereafter the MD might be used as a therapeutic option in children with NAFLD.
Methods
Study Group
The study consisted of three group of children; group 1 included obese/overweight children with recent diagnosis of NAFLD (n = 106, mean age ± SD; 12.4 ± 2.6 years) in our pediatric hepatology unit. All patients were diagnosed after January 2014, and none were prescribed any medical or dietary treatment. Diagnosis of NAFLD was made based on (1) presence of fatty liver disease in ultrasound examination with/without elevated ALT levels in obese/overweight children and (2) exclusion of other causes of fatty liver disease, such as Wilson disease, alpha 1-antitrypsin deficiency, viral hepatitis, and other metabolic diseases with clinical, laboratory, and/or histological examinations (liver biopsy was not used for the diagnosis of NAFLD). 1 Severity of fatty liver disease was graded as 1–3 on the basis of bright liver score criteria with ultrasound. 11 Group 2 included obese children without NAFLD (n = 21, mean age 11.3 ± SD 2.6 years). Patients with obesity secondary to genetic diseases, endocrinological disorders, or metabolic diseases were not included in the study. Fatty liver disease was excluded in all cases by liver ultrasound examination. Group 3 included the healthy children (without known chronic disease) with normal BMI (n = 54, mean age 11.8 ± SD 2.9 years).
Anthropometric parameters including weight and length were measured in all children. BMI was calculated as weight (kg) divided by height squared (m2). Total body fat level was measured by bioelectrical impedance analysis with the Tanita BC 418® device (Tanita, Tokya, Japan) in obese children.
KIDMED Index
Compliance to the MD was assessed by the KIDMED index, developed by Serre-Majeur and colleagues. 12 The index includes 16 questions that summarize the characteristics of the MD. Twelve of the questions in the KIDMED index are positive and four are negative. The Turkish version of the questionnaire was used for the study which was previously validated. 13 A score of +1 was given to “yes” responses to positive questions (0 to “no” responses), and a score of −1 was given to “yes” responses to negative questions (0 to “no” responses). Total scores range between 0 and 12. A KIDMED index ≥8 indicates optimal MD compliance (good), 4–7 indicates that compliance with the MD needs to be improved (moderate), and ≤3 indicates low nutritional quality (low). 13 The questionnaire was filled by face-to-face interview by U.E.A.
Insulin (Siemens Immulite 2000 XPI®, New York, NY), triglyceride, total cholesterol, ALT, and glucose (Beckman Coulter AU5800®, Brea, CA) levels were investigated from 5 ml blood specimens collected from all subjects after an eight-hour fast. Homeostasis model of assessment-insulin resistance (HOMA-IR) values were calculated using the formula glucose (mg/dl) x insulin (μU/ml)/405. 14 HOMA-IR threshold values of 2.22 in prepubertal girls, 2.67 in prepubertal boys, 3.82 in pubertal girls, and 5.55 in pubertal boys were adopted for insulin resistance. 15
Ethical approval was obtained from the local ethical committee of Karadeniz Technical University Faculty of Medicine. Informed consent was obtained from the parents of the participating children.
Data were analyzed using SPSS Version 19 (IBM, Armonk, NY) and presented as mean ± SD or percentage. The Mann-Whitney U test and chi-square test were used to compare the proportional data and categorical data (gender, etc.) between groups, respectively. The Spearman rank correlation test was used for determination of correlations. The area under the receiver operation curve (AUROC) was used to discriminate between power of the BMI and KIDMED index score for predicting NAFLD in obese/overweight children. Significant level was set at p < 0.05.
Results
Demographic findings, anthropometric measurements, and laboratory parameters of the patients and the healthy children are shown in Table 1. No difference was found in terms of age and gender among the groups. As expected, BMI and total body fat were higher in the obese patients (with and without NAFLD) than the control group (p < 0.05 for both of them), and serum ALT and total cholesterol levels were higher in patients with NAFLD than the healthy children (p < 0.05 for both of them).
Characteristics of the Patients and Control Groups
Normal values: ALT 0–45 U/L; total cholesterol <170 mg/dl; triglyceride <90 mg/dl.
p < 0.05.
ALT, alanine aminotransferase; HOMA-IR, homeostesis model assessment-estimated insulin resistence; NAFLD, nonalcoholic fatty liver disease; n.s., not studied.
KIDMED index score in obese children with NAFLD, without NAFLD, and healthy children was 2.6 ± 2.4, 4.6 ± 1.2, and 6.2 ± 1.9, respectively (Table 2) (p < 0.05 for patients with NAFLD versus obese patients, patients with NAFLD versus healthy children, and obese patients versus healthy children). Diet compliance was good in only 4.7% of the patients with NAFLD, whereas compliance was good in 31.5% of healthy children.
KIDMED Index Score of the Groups
p < 0.05.
Some parameters of the KIDMED index among the groups are shown in Table 3. Consumption of weekly fish and nuts was significantly lower in children with NAFLD compared to healthy children (39.6% versus 79.6% and 28.8% versus 51.8%, respectively, p < 0.05).
Some Parameters of KIDMED Questionnaire among the Groups
p < 0.05.
KIDMED index score was negatively correlated with BMI (p < 0.05, r = −0.53) (Figure 2), but no significant correlation was found with ALT (p > 0.05, r = 0.145), total body fat (p > 0.05, r = −0.55), total cholesterol (p > 0.05, r = −0.113), triglyceride (p > 0.05, r = −0.057), and HOMA-IR (p > 0.05, r = 0.11). No significant difference was found in KIDMED index score between NAFLD patients grade 1 (n = 62) and grade 2, 3 hepatosteatosis (n = 44) (2.5 ± 2.4 versus 2.8 ± 2.5, p > 0.05). Additionally, no significant difference was found in KIDMED index score between NAFLD patients with normal (n = 28) and elevated ALT levels (n = 78) (2.0 ± 2.0 versus 2.9 ± 2.5, p > 0.05).

Correlation between KIDMED index score and BMI in obese and healthy children (p < 0.05, r = −0.53).
The AUROC for predicting obesity in the whole study group (n = 181) with the KIDMED index score was 0.16 (p < 0.05). KIDMED index score ≤3 has a sensitivity of 59.8% and specificity of 90%. The AUROC for predicting fatty liver disease in obese children (n = 127) with BMI and KIDMED index score was 0.78 (p < 0.05) and 0.24 (p < 0.05), respectively (Figure 3). BMI >26 has a sensitivity of 79.2% and specificity of 52.4%, and KIDMED index score ≤3 has a sensitivity of 66.9% and specificity of 76.1%.
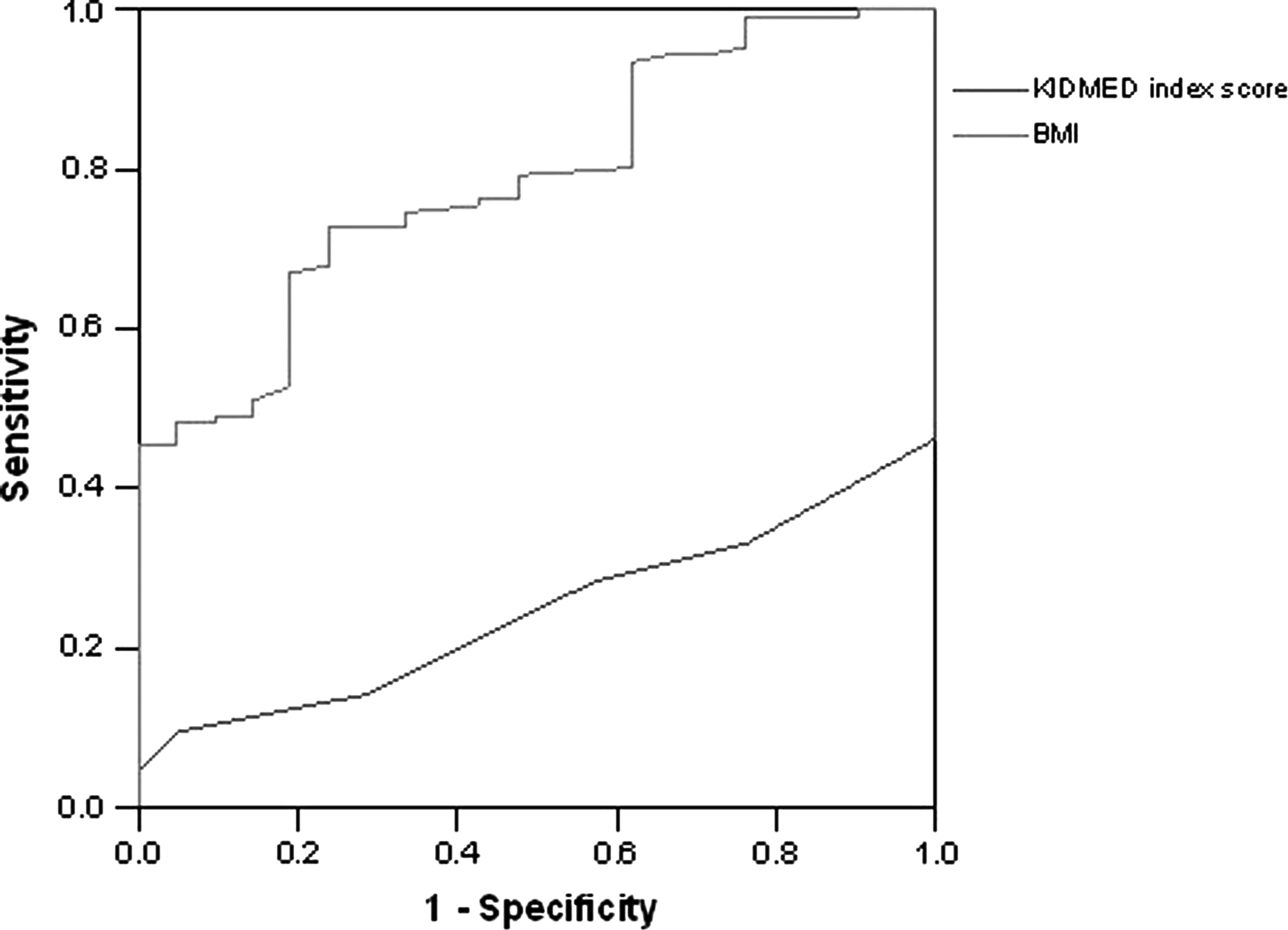
Area under the receiver operation curve (AUROC) of KIDMED index score and BMI to examine predictive use for assessing fatty liver disease in obese children. AUROC for BMI and KIDMED index score was 0.78 and 0.24, respectively, with p < 0.05 for both.
Discussion
In this study we found that low KIDMED index score (low adherence to the MD) is associated with high BMI and obesity in children, and it is one of the main predictors of NAFLD in obese children.
Consumption of fish (≥2 times/week), olive oil, and nuts (≥2 times/week) are the major components of the MD. Fish is the main source of omega-3 PUFA, and fish like salmon, anchovies, herring, and mackerel have a high content of omega 3. PUFAs are thought to have a protective role in the development and progression of NAFLD. 16 High intake of olive oil is considered a hallmark of the traditional MD, resulting in high intake of MUFA, antioxidants, and phytochemicals. Dietary olive oil has a regulative effect on hepatic lipid metabolism by reducing the lipogenic pathway, and thus attenuating liver steatosis. 17 Nuts have beneficial effect on metabolic syndrome by improving inflammation, oxidative stress, and endothelial function. These mechanisms can modulate insulin sensitivity and secretion and may decrease the risk of obesity and related complications. 18 Fish and nut consumptions were low in patients with NAFLD compared to healthy children in our study. However, the frequency of fish consumption was higher in our healthy group than reported in healthy children in a previous study, with 36% of adolescents reporting they ate fish ≥1 time/week (versus 79.6% ≥ 2 times/week). 19
The association between adherence to the MD and overweight/obesity has been shown in previous studies in children and adults.13,20–24 In the GRECO study in 2011 Farajian et al. 22 reported the highest ever prevalence of obesity in Greek children, and they claimed that increased prevalence of obesity is associated with low adherence to the MD. Kabaran et al. 13 reported inverse association between the KIDMED index and BMI in children aged between 9 and 12 years. Lazarou et al. 23 showed that adherence to the MD is inversely associated with obesity in adolescent children, and increased physical activity mediates the protective effect of the MD on obesity. In all studies authors claimed that prevalence of obesity may be decreased with high adherence to the MD.
The association between the MD and NAFLD has been well defined in adult patients.25–27 Kontogianni et al. 26 analyzed the impact of adherence to the MD on the presence and severity of NAFLD in adult patients. They found that higher adherence to the MD was associated with a lower degree of IR and less severe liver disease among patients with NAFLD. Ryan et al. 25 examined the effect of the MD on hepatic steatosis and insulin sensitivity in adult patients with NAFLD and they found that six weeks of MD decreases hepatic steatosis by improving peripheral insulin sensitivity and reducing circulating insulin concentration. Trovato et al. 27 assessed impact of adherence to the MD on hepatic steatosis after a six-month intervention, finding that adherence to the MD was a significant predictor of changes in the fat content of the liver in patients with NAFLD. The effect of diet was gradual and independent of other lifestyle changes. In all studies beneficial effect of the MD on NAFLD was associated with improvement of IR.
The association between the MD and NAFLD in children has not been studied previously. Only St-Jules et al. 28 analyzed association between dietary fish and omega-3 fatty acid intake, major components of the MD, and NAFLD in pediatric patients. They found that only 15% of the patients consumed fish ≥2 times per week and only 5% of the patients consumed ≥200 mg of long-chain omega-3 fatty acids per day. Lack of fish and long-chain omega-3 fatty acids was associated with greater portal and lobular inflammation. They recommend consuming a high amount of fish for patients with NAFLD. Our study is the first study that analyzes the association between adherence to the MD and the presence of NAFLD in obese children. We showed that low adherence to the MD in association with high BMI was the predictor of NAFLD in obese children.
The limitations of our study were (1) histology could not be used for the diagnosis of NAFLD, therefore we were unable to make a correlation between severity (such as grade of inflammation, steatosis, or fibrosis) of NAFLD and level of adherence to the MD; (2) the effect of high adherence to the MD on the improvement of liver steatosis must be prospectively evaluated in order to make a definite conclusion; and (3) lack of assessment of the effect of physical activity in our study group.
In conclusion, the MD is an inexpensive and nontoxic dietary regimen and may be used as a therapeutic option in children with NAFLD especially in regions where the ingredients are produced and consumed commonly. Education of medical doctors professionally about the content of the MD and beneficial effects on health will increase the consumption of the MD by children. 29
Author Disclosure Statement
No competing financial interests exist.