
Abstract
Abstract
Background:
Earlier biological maturation has been related to increased metabolic risk. In this study, we verified mediating effects by central adiposity of the relationship between somatic maturity and metabolic risk factors in adolescents.
Methods:
In a cross-sectional study, 1034 adolescents aged 10–16 years from Londrina/PR/Brazil were evaluated. The age of peak height velocity (PHV) method was used to evaluate somatic maturity. Central adiposity was estimated through waist circumference measurements. Fasting glucose, triglycerides, high-density lipoprotein cholesterol (HDL-C), and blood pressure were measured as metabolic risk indicators. Physical activity (Baecke questionnaire) and cardiorespiratory fitness (20-m shuttle run test) were used as covariates.
Results:
Except for fasting glucose, waist circumference showed partial or full mediation of the relationship between maturity and the following metabolic risk factors with their respective z-score values: triglycerides (boys = −3.554 vs. girls = −5.031), HDL-C (boys = +5.300 vs. girls = +5.905), systolic blood pressure (boys = −3.540 vs. girls = −3.763), diastolic blood pressure (boys = −2.967 vs. girls = −3.264), and metabolic risk score (boys = −5.339 vs. girls = −6.362).
Conclusions:
The results suggest that central obesity plays a mediating role in the relationship between somatic maturation and metabolic risk during adolescence.
Introduction
Chronic diseases represent the greatest cause of death worldwide. 1 Although the majority of events are observed in adulthood, the beginnings of chronic disease are in childhood and adolescence, and it is therefore important to identify early life risk factors, 2 such as excess body fat. 3 Childhood obesity has risen steeply in previous decades 4 and predisposes to long-term health implications, including increased risk of premature mortality and morbidity in adulthood.5,6
Recent advances of the growth and development literature have provided enhanced understanding of the genesis of chronic diseases. Early factors, such as birth weight and the growth rate in the first years of life, seem to be related to fat accumulation in childhood and adolescence, thus predicting cardiovascular risk in adulthood. 7 The mechanisms that underlie the influence of these early life variables upon adult health appear to involve biological maturation, a process characterized by the growth and maturation of all tissues of the body. 8 An important point concerns marked differences in the physical and hormonal modifications that occur between boys and girls during maturation. In addition, girls present a clearer indicator of puberty, the menarche, whereas indicators of the maturity transition (such as voice breaking) are not so clearly identifiable in boys and are remembered less well.9,10 One of the alternatives is to estimate biological maturation through a somatic indicator. A commonly used approach is the peak height velocity (PHV), which uses anthropometric measurements to estimate the position of an individual in terms of the stage of transition to adulthood and pubertal timing. 11
To our knowledge, no study has investigated the relationships between somatic maturation, central adiposity, and metabolic risk factors in representative samples of adolescents of both sexes in an integrated manner. Understanding these interrelations could help to assist the development of early interventions focused on reducing chronic disease propensity. Therefore, we investigated the relationship between biological maturation and metabolic risk factors in Brazilian adolescents with an emphasis on mediation by central adiposity.
Methods
Sample
This was a school-based epidemiological cross-sectional study conducted in adolescents aged 10–16 years, who were enrolled in public schools at Londrina, PR, Brazil, in school year 2011. Located in the north of Paraná State, the city of Londrina has 506,701 inhabitants, a human development index of 0.778, and a gross domestic product per capita of US$ 8530.77. 12
Sample recruitment was performed in two stages. First, all the city's schools were listed by geographic region (north, south, east, west, and center) and two were randomly selected from each region. Thereafter, classes from the chosen schools were randomly selected and students in those classes were invited to participate. Students on medication, undergoing treatment for illness, or who did not return the written consent form signed by their parents or guardians were not eligible for the study. Initially, 1395 adolescents entered in the study, but 361 failed to provide all data for this analysis and were, therefore, excluded. We have previously commented that there are no differences in characteristics between those participants with and without complete information in this dataset. 13 The local ethics committee approved all of the study procedures adhered to the principles of the Declaration of Helsinki. Additionally, details of the final sample and methods are presented, respectively, in Supplementary Figure S1 and Supplementary Table S1.
Somatic Maturation
To estimate somatic maturation, we used the age of PHV, which is the most commonly used indicator of maturity in studies of adolescents. PHV was estimated using chronological age and three anthropometric variables (stature, sitting height, and body mass). 11 Predictions of the age at PHV were used to derive categories of pubertal timing for boys (late: >14.8 years; on time: 14.8–13.4 years; early: <13.4 years) and girls (late: >13.0 years; on time: 13.0–11.8 years; early: <11.8 years). In the main analyses, somatic maturation was treated continuously.
Central Adiposity
Waist circumference was measured at the midpoint between the lowest rib and the upper edge of the iliac crest to the nearest 0.1 cm. Three measurements were collected for each participant and the median was calculated. To characterize the sample, participants were dichotomized as having normal or high waist circumferences. 14
Cardiovascular Risk
Blood pressure was measured on the right arm after a rest period of 10 minutes using automatic equipment (Omron–HEM-742) that has been validated in adolescents. 15 Two measurements interspersed with a rest interval of 2 minutes were made and the arithmetic mean of values was calculated. If the difference between measurements was greater than 10 mmHg for systolic blood pressure (SBP) and diastolic blood pressure (DBP), then a third measurement was performed. In this case, the two closest values informed the mean.
Laboratory tests were conducted at the Biochemistry Laboratory at the University Hospital of Londrina State University. Blood samples were collected after a 12-hour fast from the antecubital vein, either in serum tubes (no anticoagulant) or for the determination of glucose a tube containing an anticoagulant fluoride preservative. Tubes were centrifuged at 3000 rpm for 5 minutes at 4°C to separate plasma and serum. Analyzes were performed immediately following separation of these materials using a biochemical AutoAnalyzer (Dimension RxL Max—Siemens Dade-Behring).
Continuous metabolic risk scores were derived using z-scores of the following variables: triglycerides, fasting glucose, high-density lipoprotein cholesterol (HDL-C; with opposite sign), and the arithmetic mean of SBP and DBP ((triglycerides z + fasting glucose z + [−1 * HDL-C z] + [{SBP z + DBP z}/2])/4).
Covariates
We have previously shown that somatic maturity, waist circumference, and metabolic risk factors exhibit associations with physical activity and cardiorespiratory fitness in this group of Brazilian adolescents. 13 To enable control for these factors in analyses, physical activity was self-reported using the Baecke questionnaire, which has questions about activity performed in school, formal sports, and leisure time. The sum of these domains constitutes habitual physical activity, 16 which had a good reproducibility as identified by an intraclass correlation coefficient of 0.73. Cardiorespiratory fitness was assessed using a widely implemented, reliable, and valid 20-m indoor shuttle run test 17 that is described in greater detail by Leger and Lambert. 18 Based on test results, estimated peak VO2 (mL·kg−1·min−1) was calculated using specific equations. 19
Statistical Analysis
Descriptive statistics are presented using means and standard deviations. As appropriate, Kruskal–Wallis and Mann–Whitney tests were incorporated to detect differences in variables between genders, normal vs. high waist circumference groups, and according to the three groups of pubertal timing. Due to the non-normality of outcomes, for the main analysis, SBP and DBP, fasting glucose, HDL-C, and triglycerides were normalized using a logarithmic transformation. Thereafter, partial correlations were performed between independent, mediator, and outcome variables, adjusting by chronological age, physical activity, and cardiorespiratory fitness.
The mediation analyzes were performed according to the principles of Baron and Kenny. 20 In the first instance, the mediator variable (waist circumference) was regressed onto the independent variable (somatic maturation). In the second equation, the dependent variable (metabolic risk, log SBP, log DBP, log fasting glucose, log HDL-C, or log triglycerides) was regressed onto the independent variable. Finally, in the third equation, the dependent variable was regressed into the independent variable, adjusted for the mediator.
Mediating effects were identified if the following criteria were met: (1) in the first equation, the independent variable was a significant predictor of the mediator; (2) in the second equation, the independent variable was a significant predictor of the dependent variable; and (3) in the third equation, the mediator was a significant predictor of the dependent variable, and the association between the dependent and independent variable (from equation two) was either partially or fully removed. We did not perform multilevel mediation analysis, due to the low variance of biological variables between clusters; the intracluster correlation coefficients ranged between 0.017 and 0.066 for the main variables (independent, mediator, and outcomes), according to the formula proposed by Fleiss. 21 Analyzes included the Sobel test and all statistics were carried out according to the procedures described in the literature. 22 For all statistical analyses, significance was accepted at p < 0.05. The data were analyzed using SPSS software version 22.0 (SPSS, Inc., Chicago, IL).
Results
The sample of this study was composed by 1034 adolescents, of which 21.8% presented abdominal obesity. Table 1 shows further characteristics of the sample. It can be observed that early maturing adolescents exhibited higher values for individual risk factors (including waist circumference) and the composite metabolic risk score; the same was true for individuals with high waist circumference.
General Characteristics of the Sample (n = 1034)
BP, blood pressure; CRF, cardiorespiratory fitness; HDL-C, high-density lipoprotein cholesterol; PHV, peak height velocity.
Comparisons: sex (*p < 0.05 vs. girls; **p < 0.01 vs. girls), waist circumference (*p < 0.05 vs. high; **p < 0.01 vs. high), and maturation (a: p < 0.05 vs. b).
Partial correlations between independent variable (somatic maturation), the mediator (waist circumference), and outcomes are presented in Table 2. With the exception of fasting glucose, all other metabolic risk factors were significantly correlated (p < 0.05) with somatic maturation and waist circumference.
Partial Correlations Between Independent, Mediator, and Outcomes According to Sex (n = 1034)
All models were adjusted for chronological age, cardiorespiratory fitness, and physical activity.
Log, logarithm.
p < 0.05.
Results for mediation by waist circumference of the association between somatic maturation and metabolic risk factors in girls are shown in Figure 1. As each model shows, in girls every 1 year later in the age of PHV was associated with ∼6.9 cm lower waist circumference. Waist circumference acted as a mediator of all associations, except for fasting glucose. Similar results were found in boys (Fig. 2).
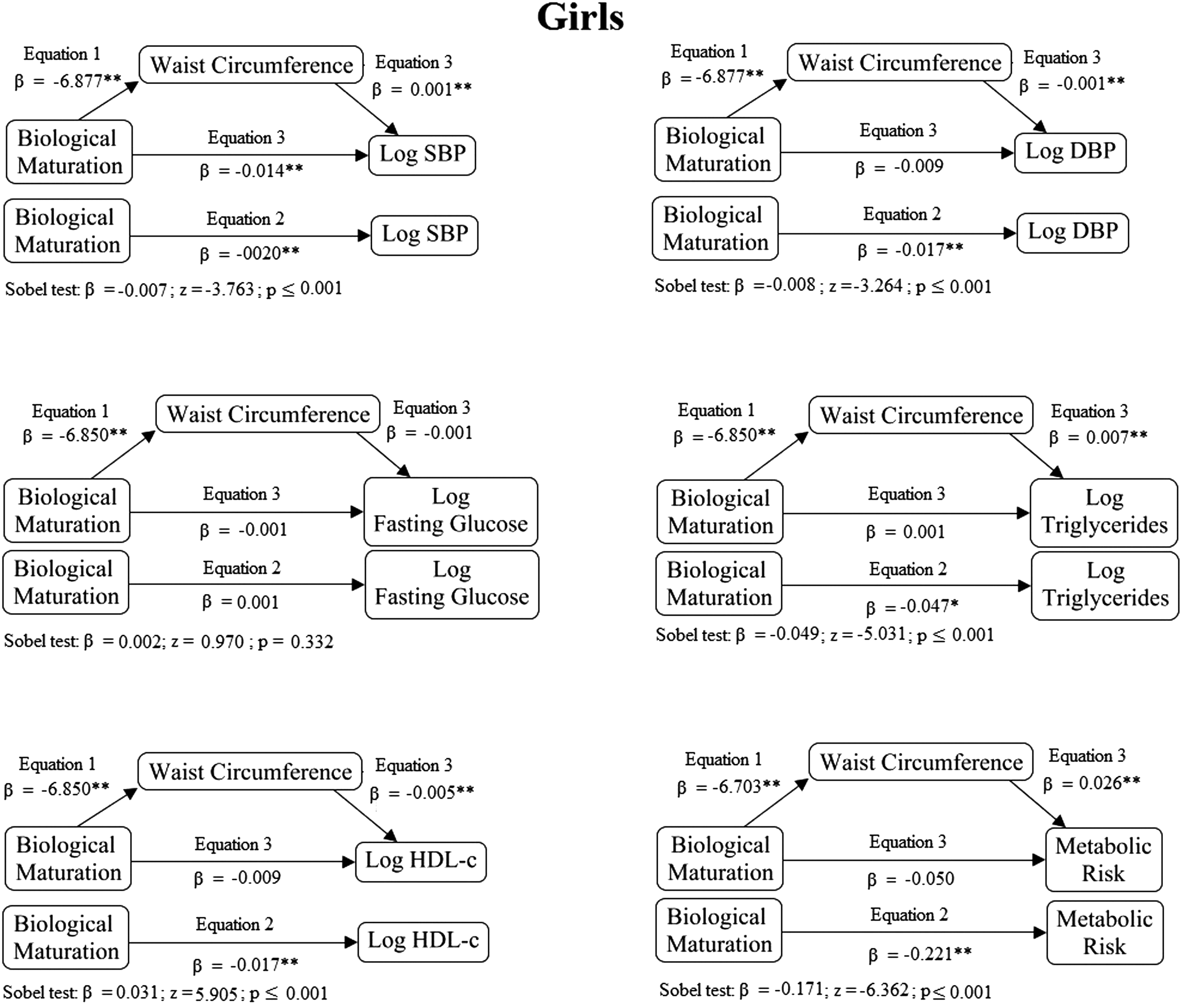
Mediation by waist circumference of the relationship between biological maturation with single risk factors and a composite metabolic risk score in girls. Models were adjusted for chronological age and physical activity. *p < 0.05; **p < 0.001.
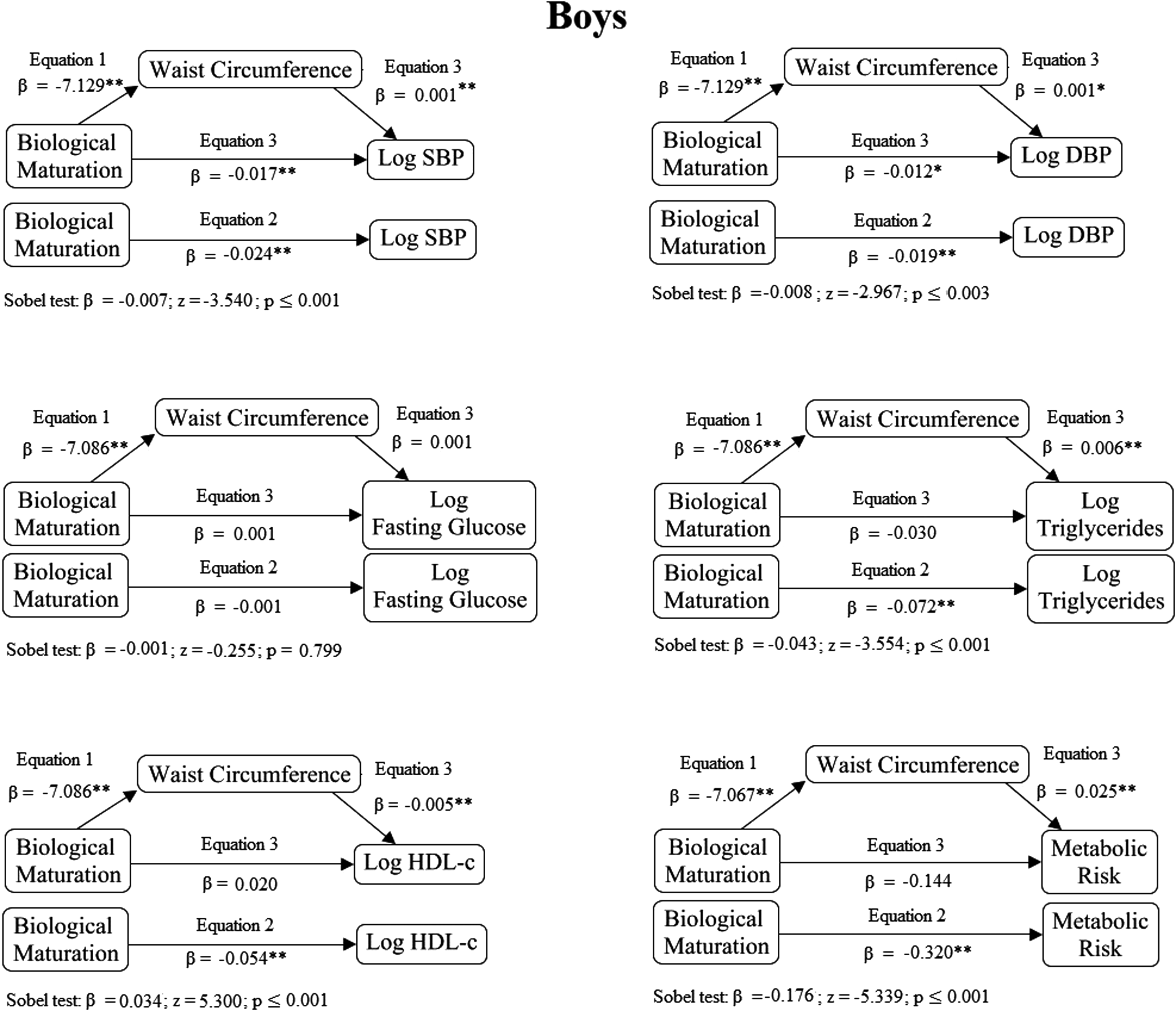
Mediation by waist circumference of the relationship between biological maturation indicator with single risk factors and a composite metabolic risk score in boys. Models were adjusted for chronological age and physical activity. *p < 0.05; **p < 0.001.
Discussion
Our findings indicate that early maturing adolescents have more central adiposity and present with greater metabolic risk. We further established that central fat mediated at least partially the relationship between somatic maturation and metabolic risk profile for both boys and girls. The results, therefore, implicate both biological maturation and central adiposity in determining metabolic risk in youth, but identify that neither is solely responsible.
It has previously been acknowledged that earlier somatic maturation is adversely related to cardiometabolic risk.23,24 For instance, studies have shown that earlier menarche is positively associated with cardiovascular risk in adulthood.24,25 Body fat, in particular centrally stored adiposity, also exhibits a strong relationship with metabolic risk factors. 26 However, the interrelations between biological maturation and central adiposity in determining cardiovascular risk have not been well established, particularly in terms of mediating effects and the exact sequence of biological events taking place.27,28 The present study offers insight into these matters.
There is continued debate about whether or not adiposity acts as a precursor of earlier maturational development. Contemporary youth are maturing earlier than before and one hypothesized explanation is an increased prevalence of pediatric overweight and obesity. 29 Particularly in girls, increased body fat seems to be an indicator of advanced physical biology and readiness for sexual reproduction. A mechanism underlying this concept involves increased production of growth hormone in response to heightened blood concentrations of leptin, a source of which is adipose tissue.29,30 Our data confirm that there is a relationship between body fat and early maturation in adolescents, but due to an absence of repeated data collected on either side of puberty, our analyses preclude any conclusions regarding the temporal nature of the association. Interestingly, however, for half of the metabolic outcomes we studied, central adiposity did not totally mediate the association between somatic maturation and metabolic risk. This means that other features arising from earlier maturational development, aside from higher central fatness, must predispose to an adverse metabolic profile. 9
An alternative perspective on the interrelations between somatic maturation and abdominal obesity with metabolism does not begin with adiposity, but rather implies that early sexual maturation itself provokes a cascade of negative metabolic events. These events, such as hyperplasia of adipose cells, 31 which acts to confer higher body fat, are thought to result from the faster growth rates in cells and tissues of earlier matures compared to their on-time or late developing peers. Cardiovascular and endocrine systems may also be disrupted by early maturation, and even gene expression altered, potentially increasing cardiovascular risk.32–34 Our data can neither confirm nor deny these mechanisms of effect, but highlight that they cannot be sole explanatory factors. Abdominal obesity either partially or fully mediated the relationship between somatic maturation and metabolic risk, at least for most of the risk factors we investigated.
Our results seem to concur with the “perfect storm” proposition, 9 which suggests that, regardless of the direction of the association between biological maturation and body fat, both conspire to increase cardiovascular risk during puberty. Body fat (especially visceral compartments) certainly exhibits a strong and direct relationship with cardiovascular risk that is independent of maturational status.24,35,36 The role of maturational timing may be more indirect, acting through various physiological and psychosocial mediators, of which increased adiposity may be just one.
With regard to previous findings, although we did not observe relationships between pubertal timing and central obesity with plasma glucose levels, Hillman et al. 37 reported that a relationship between maturation and insulin sensitivity in girls was mediated by adiposity. Differences in measurement methods for maturation, adiposity, and insulin resistance, and differences in study population, may underlie the discrepant conclusions. To the best of our knowledge, no other formal evaluations have been conducted on the topic of biological maturation, metabolic risk, and mediation by central adiposity.
A point worthy of discussion is the similarity of results in both sexes. Girls and boys tend to respond differently to puberty-related changes in the endocrine system, with girls accumulating more subcutaneous adipose tissue peripherally around the hips 31 and boys preferentially depositing subcutaneous adipose tissue about the abdomen and more visceral fat around internal organs.38,39 Despite these differences, our results indicate that the “perfect storm” applies to both sexes, and therefore, attention should be targeted toward girls and boys equally for the prevention and treatment of metabolic disease. It may be wise to suggest that behavioral interventions, particularly performed in schools,40,41 and with a focus on the prevention of early obesity, could be particularly worthwhile, and may even assist in reversing the secular trend of early maturational timing. 7 Moreover, obese and early maturing adolescents should receive special attention, as, in accompaniment to a worse metabolic health profile, they are more likely to adopt and sustain unhealthy lifestyle behaviors due to a myriad of biological and psychosocial factors.
It is important to mention that our cross-sectional investigation does not allow us to establish causal relationships, let alone the directions of association, between exposure, mediators, and outcome variables. However, we adopted an objective, valid, and commonly implemented method to estimate somatic maturation. This approach (PHV) also eliminated the necessity to analyze categories of pubertal timing, avoiding limitations of cutoffs. 42 Finally, our analyzes of more than 1000 Brazilian adolescents were adjusted for important confounding variables, including cardiorespiratory fitness, which have relation with the main variables of the study,14,43 and self-reported physical activity levels, which we have shown to be related to maturation and metabolic risk in the study population.13,14 We do acknowledge, however, that objective measurements of physical activity would have been superior.
We conclude that central adiposity plays a mediating role in the relationship between biological maturation and metabolic risk in adolescents. These findings highlight the importance of tackling the determinants of obesity, which may include early maturation, for improved metabolic health. They also provide support for focused health promotion directed toward adolescents who have matured early and who may be at elevated risk for obesity and metabolic disease. Prospective, observational, and experimental studies should be conducted to further augment understanding of these phenomena in the first two decades of life and to help formulate an evidence base for effective intervention.
Footnotes
Acknowledgments
The authors thank the school administrators, in which the study was conducted, for allowing the researchers to conduct observations and the young people who took part in this investigation. The authors also thank Alessandra Okino, Jair Oliveira, Danielle Venturini, Crisieli Tomeleri, Mariana Carnelossi, and Sandra Kawaguti for their substantial contributions to the research, including assistance in data collection and entry. This study was funded by the National Council of Scientific and Technological Development (CNPq/Brazil–Process 483867/2009–8). ERVR, ESC, and RAF were supported by grants from CNPq/Brazil. DRS (sandwich doctorate scholarship - process 201022/2015-0) and AOW (scientific initiation) are also supported by CNPq.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.