
Abstract
Abstract
Background:
There is growing evidence supporting social network-based interventions for adolescents with obesity. This study's aim was to determine the feasibility of a social network-based intervention by assessing adolescents' friendship networks, willingness to involve friends in treatment, and how these factors influence enjoyment.
Methods:
Adolescents (N = 42) were recruited from a tertiary care obesity clinic. Participants gave a list of closest friends, friendship characteristics, and which of their friends they would involve in treatment. A subset (N = 14) participated in group treatment, were encouraged to bring friends, and invited to a second interview.
Results:
Participants nominated a mean of 4.0 (standard deviation [SD] = 1.6) friends and were more likely to nominate closer friends (p = 0.003). Friends who attended group sessions were more likely to have multiple friendships in common with the participant's own network (p = 0.04).
Conclusions:
Involving friends in treatment is feasible and desired by adolescents and may be a novel approach for augmenting obesity treatment outcomes.
Introduction
Efficacy of pediatric weight management programs has shown some success, but is often limited by three areas of concern: high attrition, 1 moderate efficacy, and low adherence to behaviors after intervention has ended. 2 Novel approaches are needed to help participants attend intervention sessions and maintain behavior changes after programs have ended. Network-based health interventions—interventions that involve participants' social networks—have been shown to reduce attrition and increase adherence when implemented in other domains of adolescent health, such as substance abuse prevention. 3 However, the feasibility of the network-based interventions for adolescent weight management has not been evaluated.
Obesity-related behaviors, such as physical activity, eating, or sleep hygiene, have been shown to diffuse through adolescent social networks.4–10 Therefore, weight management interventions that fail to account for adolescents' social network may limit adolescents' capacity to successfully manage weight and related behaviors. For instance, a study by Bahr et al. (2009) demonstrated through simulation that individuals of the same weight status tend to cluster into the same social groups, which has been supported in other studies.9,11,12 These simulations suggest that individuals who successfully lose weight not only are less able to maintain weight loss due to influences within their surrounding social networks but they are also more likely to return to their original weight. Thus, for those who have experienced weight loss, it may be difficult to maintain associated lifestyle behaviors if their surrounding network (i.e., friends and family with whom they interact regularly) maintains and reinforces old behaviors. This suggests that a network-based intervention in which people attempt weight loss with friends and friends of friends may be promising because it would create a stable cluster of individuals practicing similar healthy behaviors. 11 A previous review described different types of network intervention approaches. In this article, we focused on the induction approach, which uses peer-to-peer interaction to create behavioral diffusion. 13
The purpose of the current study was to examine the feasibility of implementing a pediatric obesity intervention that leverages adolescents' existing social networks. We decided to focus on friendship networks because of the well-documented influence of peers on behavior during adolescence. Specifically, our aims were to (1) determine whether adolescents are open to involving friends in their weight management interventions given the stigma of obesity; (2) determine the characteristics of friends that adolescents wanted to involve in their treatment versus those they did not want to involve in their treatment; (3) determine whether friends of participants are willing to be involved in the intervention; (4) compare the friends that adolescents bring to a group class series with those that they do not bring; and (5) qualitatively asses how bringing friends affected patients' enjoyment and motivation to attend group classes. This study solicited traditionally underserved populations, including (1) Latinos with Spanish-speaking parents, (2) African Americans, and (3) rural areas with limited access to healthcare.
Methods
Study Design
This study used a concurrent, nested mixed methods design involving two standardized one-on-one interviews conducted by trained study personnel. 14 Interview 1 collected qualitative data to assess adolescents' openness to involving peers in treatment and quantitative data on the structure of adolescents' friendship networks. Among a subsample of the adolescents, Interview 2 assessed the effect of bringing friends to weight management sessions, with a specific focus on participants' enjoyment of and attendance at treatment sessions. Interview 1 was completed immediately before participation in group sessions; Interview 2 was completed after the 6-week series of weight management group sessions ended.
Study Population
Participants
Male and female adolescents aged 11–17 years who spoke English or Spanish were recruited from a tertiary care pediatric obesity clinic within an academic medical center (See Brenner FIT below) and invited to participate in a study interview. Participants included (1) an English-speaking population receiving care within the clinic, (2) a Spanish-speaking population receiving care exclusively in Spanish within the clinic, and (3) a rural English-speaking population receiving majority of their care through telemedicine. Friendship network data were collected through 1:1 interviews. Participants were recruited from among the patients already receiving care from the clinic. This was a two-part study (Interview #1 and Interview #2). Participants were invited for the second part of the study if they had completed the first part of the study and had signed up to participate in a 6-week group class weight management series (provided by the clinic, details below). Adolescents were only excluded if already enrolled in another research study involving weight management. It was not required that participants enrolling in the first part of the study commit to signing up for the group class series or bringing friends to classes because we did not want to bias our sample.
Brenner FIT
Brenner FIT (Families In Training) is a multicomponent, interdisciplinary, pediatric weight management program within Brenner Children's Hospital (part of Wake Forest Baptist Medical Center and Wake Forest School of Medicine in Winston-Salem, NC). Brenner FIT accepts referrals from primary care physicians and subspecialists and is open to children aged 2–18 years who are overweight or obese. In line with expert recommendations, 15 Brenner FIT employs a family-based model, encouraging participation from the entire family in all aspects of treatment, although only a parent or guardian is required to attend with the child. Treatment typically lasts 12 months, with visits averaging one to two times a month, a combination of individual visits with dietitians and family counselors who focus on behavior change and goal setting and group classes geared toward nutrition and activity education. Details of the program have been previously published.16–21
Various group class series lasting 6 weeks each are offered as an add-on to the care that the families receive in clinic. Patients who were planning to participate in one of the two group class series, strength training or self-esteem, were solicited for the second part of this study (Interview #2). Participants are encouraged, but not required, to bring friends to these classes, but their friends must be of the same gender. Although parent participation is mandated for patients enrolled in the Brenner FIT clinic, we did not require parent participation for friends attending group sessions as they were not enrolling as patients. The strength training series were led by an exercise specialist and were an all-female or all-male group. Sessions were 90 minutes in duration and consisted of graduated instructions of warm-up, strength-training exercises (resistance bands), and stretching. The self-esteem series was also 90 minutes in duration, and attendance was limited to females. Social workers led sessions with female participants about how to discuss weight with their parents and families. Girls participated in interactive sessions with estheticians who lead discussions on how to dress for their body types, how to correctly size bras, and other related topics.
Recruitment
Interview 1
Patients who received care in person were provided with an informational flyer about the study during a regularly scheduled appointment. Interested patients (and their parents) who provided permission to be contacted then received a phone call from the study coordinator to discuss the study and schedule an appointment to obtain written parental consent/child assent and begin data collection.
Patients who received care through telemedicine were first contacted through telephone by a clinician who provided basic information about the study. If interested in the study, they were asked to give permission to be contacted by study staff through telephone for more information. If the adolescent agreed to participate, they first provided verbal assent and parental permission through telephone. Data were then collected over the phone and consent/assent forms were mailed in duplicate with a prestamped return envelope. No data were analyzed until study staff received signed consent forms. All consents were obtained in participants' and parents' preferred language (English/Spanish). The Institutional Review Board at Wake Forest School of Medicine approved the study protocol. Participants received $10 for completing the first interview.
Interview 2
Those who participated in Interview 1 and were participating in one of the group training series were contacted and asked to participate in Interview 2. Participants received a $10 incentive for completing the second interview. Participants were not reconsented before participating in the second interview.
Friends who attended sessions with participants were not consented because the only data item collected about them was the number of friends a participant had brought. Names and contact information of friends were not collected by study staff.
Measures
Interview 1
Data for Interview #1 were collected before the participants started the group class series. Network Data Collection: A standard method of collecting network data with a name generator was used. 22 Participants (egos) were asked to generate a list of closest friends (alters) without aid and without limit on the number they were allowed to nominate. They were then queried for characteristics of each friend and for relationships among friends (alter ties). Figure 1 illustrates how alter tie information was collected. Alter names were filled in the first row and first column, and alter tie information was collected by filling in the appropriate code based on the relationship (alter tie strength) between the two friends. In the made-up example, a study participant provided the names of five friends. Participants were asked which friends they had told that they were in obesity treatment, to nominate friends they would prefer to bring to treatment with them, and why. If a participant nominated a friend who was not on the list, the friend was added.
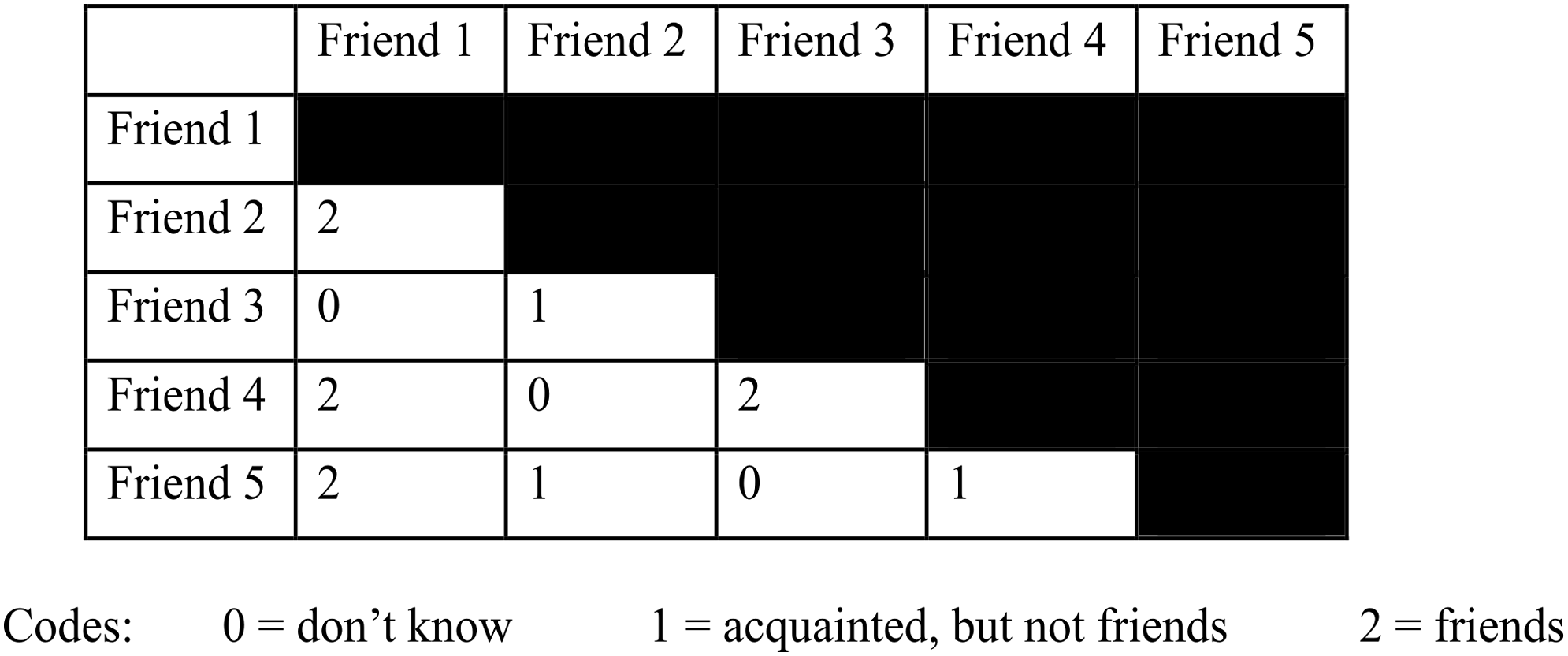
The figure shows an example of friends and alter tie strength: Friend 1 and Friend 2 are friends. Friend 1 is not acquainted with Friend 3. Friend 2 and Friend 3 are acquainted, but not friends.
Qualitative Data Collection: Participants were asked how they anticipated bringing friends would make them feel.
Interview 2
Interview #2 was completed after the group class series was finished. Network Data Collection: Participants were asked which of their friends they were able to bring to group sessions. The list of friends was then compared with the list provided in Interview 1.
Qualitative Data Collection: Participants were then asked about (1) barriers to bringing friends, (2) how bringing friends affected their participation in the program, both in session attendance and enjoyment, and (3) whether they wished to continue to bring friends to sessions with them.
Data Analysis
Several egocentric network measures were calculated and are listed along with alter characteristics in Table 1.
Ego and Alter Characteristic Measures
T tests were performed on the following continuous variables: tie strength, age difference, and frequency of contact. Chi-square tests were performed to assess the difference between groups on the following categorical variables: perceived weight status, previously discussing treatment, and gender homophily. We used data from Interview #1 to compare friends who participants said they wanted to bring with them to clinic and those they did not say they wanted to bring.
Data from participants who only were in Interview #1 were excluded from all Interview #2 analyses. We used data from Interview #2 to compare friends who participants were able to attend group classes with participants and those who were not. Additionally, for Interview #2, attendance rates of participants who brought friends were compared with attendance rates of a historical group of adolescents who had participated in the same group classes, but none had brought friends.
Qualitative Analysis
Interview transcripts were analyzed using a systematic content analysis to gain a different perspective on adolescents' view on involving friends in their obesity treatment. Interviews were transcribed verbatim and then reviewed to develop a set of common codes that arose among the interviews. Alike codes were then assembled and differences were adjudicated as necessary in an iterative process until a final set of themes about the interviews had been reached.
Results
Network Analysis
Interview 1
A total of 46 eligible adolescents were contacted and 42 participated in Interview 1. Among those who chose not to participate (one white male, one Hispanic male, one Hispanic female), one felt that questions would be too personal and another patient's mother did not want her daughter to participate in a private interview. An additional participant who provided consent declined to participate due to time constraints.
Demographics of participants are described in Table 2. The ethnically diverse sample was representative of the clinic population from which they were recruited. 20 The participants (N = 42 egos) nominated and described 166 friends (alters) who are in their close friend group. The nominations demonstrated high gender and age homophily; most ego–alter pairs were similar in sex (Table 2).
Ego and Alter Demographics
BMI, body–mass index; SD, standard deviation.
The friends that participants wanted to bring to group sessions with them were only different from other close friends, in that they were closer or better friends (significantly higher tie strength, p < 0.003); all other variables assessed were not significantly different (frequency of contact, alter–alter ties perceived by ego, closeness, ego–alter age difference, weight status, whether the ego had discussed treatment with that alter, sex), as shown in Table 3.
Characteristics of Alters Nominated or Not Nominated To Be Involved in Treatment or Characteristics of Alters Brought or Not Brought to Treatment
T tests were used to test for differences between means; Chi-square tests were used to test for differences between proportions.
Interview 2
Fourteen of the 42 participants who participated in Interview 1 also participated in Interview 2. Participants in Interview 2 (N = 14) discussed 58 friends for this section of the analysis.
The friends that participants brought to group sessions were only different from other close friends they nominated, in that they were friends with more of the participant's friends (alters had significantly higher degree in ego network, p < 0.04); all other variables assessed were not significantly different (Table 3). Definitions of degree and other measures are listed in Table 1.
The average number of group sessions attended, of six sessions in total, was 44% (SD = 27) for participants attending with one or more friends and 38% (SD = 26) for adolescents attending without any friends. Attendance rates were not significantly different between groups (p = 0.5).
Qualitative Analysis
Of the 42 participants, 94% reported that they would be open to bringing friends to treatment, although only 42% of participants had previously discussed treatment with friends (Table 2). Reasons for not telling their friends were nonspecific such as “I forgot” or “It never came up in conversation.” Very few reported that they had not or would not tell their friends about weight management because it was too sensitive a topic. Most felt neutral about telling their friends they were in treatment “I wouldn't care” or “I wouldn't be ashamed.” All who wanted to bring friends reported they felt it would help them have a more positive experience. Specifically, they felt it would help them have more fun, be more comfortable, and motivated:
Because we all laugh at each other, because the last time we were here they had us doing yoga, and some of those positions are very compromising and we were laughing at each other because [my friend] would fall over or [my friend] would kick me in my head by accident because we were so close together in the room, so we're all looking stupid, but we were laughing about it.
Analyses showed that there was no relationship between friends whom adolescents nominated to bring to treatment and that friend's weight status, how long they had known that friend, or other characteristics (Table 3). However, the qualitative data showed that adolescents reported a mixture of reasons for nominating certain friends to bring to treatment or choosing to discuss treatment with that friend. Some reported they picked their closest friend (in agreement with the quantitative analyses) and others because that friend was overweight and would be able to relate or would be nonjudgmental. Some chose friends they felt would be good at helping them make new friends among the other adolescents in the program. Almost all adolescents felt that their friends would react positively and be supportive when they discussed treatment with them.
Adolescents in this study did not perceive that the behavioral lifestyle changes they were making in treatment (increasing physical activity, fewer sugar-sweetened beverages) influenced their friends to make these same changes. However, there were some who felt their friends influenced their ability to make those changes (either positively or negatively) by either facilitating or being detrimental to the changes.
Adolescents most frequently cited scheduling conflicts as the reason that friends were not able to come. Several adolescents said they brought family members instead or brought friends they knew would be available at the time group sessions were scheduled. All participants who brought friends said they would like to bring friends to treatment again.
Discussion
This study indicates that a network-based intervention among adolescents participating in pediatric obesity treatment is feasible. All adolescents had at least one friend in their friendship network (degree >0) and the majority was open to involving friends in their treatment (Table 2). Importantly, for a network-based intervention, the friends that participants actually brought to group sessions were friends with more of the participant's friends, thus in the position of reaching other network members. Additionally, because clustering was high (Table 2), involving multiple friends may also be feasible. Adolescents preferred to bring friends who were closest to them (high tie strength) regardless of other factors (Table 3). This confirms findings from other social network research that found that strong ties are more important for sharing consequential actions that affect health. 23 However, their reasons for choosing certain friends to bring to treatment included weight status or someone who would help them make more friends. The main barriers to bringing friends to treatment were scheduling and transportation. It is possible that a network-based intervention would be more difficult in adolescents because they are dependent on their parents for transportation and have less control over their schedule than adults.
We did not find that bringing friends to treatment improved attendance, but the study was not powered to detect such a difference. However, we found there may be other benefits to attending with friends that became apparent through interviews. Overall, adolescents felt it was more fun and felt more supported to attend with friends. Bringing friends may be helpful in preventing attrition if friends attend sessions that patients miss and are able to help keep patients engaged. Friends attending may also allow for carpooling, which could potentially improve attendance.
Results of the study are intended to inform a pilot implementation of a friendship network-based intervention for pediatric obesity treatment. These efforts have the potential to accelerate and maintain behavior change in adolescents undergoing obesity treatment through utilization of existing social relationships. This study helped determine that this design is feasible in practice, with adolescents expressing comfort in bringing friends to weight management group sessions.
This study suggests that further testing of a network-based intervention among adolescents is warranted and holds potential as a new treatment. An additional challenge to involving friends in clinic was identified: the friends that adolescents are able to bring to treatment may not be the preferred friend due to logistics of scheduling and transportation.
Limitations
The main limitation to this study is the small sample size. Participants were exclusively recruited from one obesity treatment program in North Carolina, and results might not be generalizable to different locations. However, the sample recruited was representative of the clinic population from which they were recruited, and included ethnic/racial and urban/rural diversity. Personal network exposure was calculated based on whether the ego perceived their friend to be overweight, rather than measured body–mass index. This information was still valuable in the current study because we sought to understand if adolescents preferred to bring friends who they perceived as also overweight. This study was an observational study without a control group, which makes it harder to determine the true effect of bringing friends to treatment. Adolescent friendships may be dynamic and change over time, leading to further complexity in social networks. Specifically, other studies have found that best friends (strong ties) and the person who people trust from their social network may change frequently when queried at multiple time points. 23 Our study only examined a single time point in time. Additionally, the adolescents we observed were followed for a short period of time (6 weekly sessions). It may take more time and a larger sample size for the effect of friends on attendance to become apparent.
Conclusions
Involving adolescents' friends in pediatric obesity treatment is feasible. This study suggests that bringing friends improves enjoyment and was even desired by adolescents. Future research is needed to investigate the impact of using friendship networks in obesity interventions, especially during adolescence when peer influences are significant.
Footnotes
Acknowledgments
The authors would like to acknowledge Caroline Kimes for help in data management. Funding: Ms. Giannini was supported by the National Institutes of Health Research Supplement to Promote Diversity in Health-Related Research, Award Number P60MD006917 (Bell PI), from the National Institute on Minority Health and Health Disparities and by National Institute of General Medical Sciences T32 GM063483–14; this work was supported by Award Number K23HD061597 (Skelton PI) and Award Number K23HD064700 (Gesell PI), both from the Eunice Kennedy Shriver National Institute of Child Health and Development. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
The research included in this article was carried out at Wake Forest School of Medicine.
Author Disclosure Statement
No competing financial interests exist.