
Abstract
Abstract
Background:
Prospective patient registries have been successfully utilized in several disease states with a goal of improving treatment approaches through multi-institutional collaboration. The prevalence of youth with severe obesity is at a historic high in the United States, yet evidence to guide effective weight management is limited. The Pediatric Obesity Weight Evaluation Registry (POWER) was established in 2013 to identify and promote effective intervention strategies for pediatric obesity.
Methods:
Sites in POWER provide multicomponent pediatric weight management (PWM) care for youth with obesity and collect a defined set of demographic and clinical parameters, which they regularly submit to the POWER Data Coordinating Center. A program profile survey was completed by sites to describe characteristics of the respective PWM programs.
Results:
From January 2014 through December 2015, 26 US sites were enrolled in POWER and had submitted data on 3643 youth with obesity. Ninety-five percent were 6–18 years of age, 54% female, 32% nonwhite, 32% Hispanic, and 59% publicly insured. Over two-thirds had severe obesity. All sites included a medical provider and used weight status in their referral criteria. Other program characteristics varied widely between sites.
Conclusion:
POWER is an established national registry representing a diverse sample of youth with obesity participating in multicomponent PWM programs across the United States. Using high-quality data collection and a collaborative research infrastructure, POWER aims to contribute to the development of evidence-based guidelines for multicomponent PWM programs.
Introduction
Identifying effective and sustainable pediatric weight management (PWM) interventions remains a critical national health priority due to the increasing prevalence of severe obesity among children and adolescents over the past decade. Analysis of US data reveals a near 50% increase in severe obesity (4.7% in 1999 to 7.0% in 2012) among youth ages 2–19. 1 The concurrent rise of obesity-related comorbidities in youth, including insulin resistance, dyslipidemia, nonalcoholic fatty liver disease, hypertension, obstructive sleep apnea, and associated low self-esteem, highlights the crucial need for proven treatment strategies to improve health outcomes. 2 To date, limited evidence exists to guide effective and sustainable treatment for youth with severe obesity participating in PWM programs.
The US Preventative Services Task Force recommends that youth aged six and older with body–mass index (BMI) at or above the 95th percentile be referred to a multicomponent PWM program that includes medical, nutrition, physical activity, and behavioral counseling. 3 A systematic review of multicomponent PWM programs found that medium (26–75 provider contact hours) to high intensity (≥76 hours) interventions for at least 6 months achieved significant reduction in BMI for youth with obesity. 4 However, such guidelines for PWM program design are limited by the lack of consistent reporting of data across studies on key variables such as (1) provider type(s) dedicated to the program, (2) the level and duration of provider contacts, (3) program characteristics, and (4) process outcomes (i.e., attrition). 3
The development of pediatric registries has led to advancements in diseases, such as cancer and diabetes, through the creation of treatment protocols and multisite research collaboration.5,6 The Search for Diabetes in Youth Study (SEARCH) registry began in 2000 and is the largest US study of diabetes in children and adolescents. This successful collaborative effort is tracking youth into early adulthood to identify predictors of diabetic complications. 7 With regard to pediatric obesity, registries have been established in Europe 8 and Canada. 9 The Working Group of Obesity in Childhood and Adolescence was founded in Germany in 1998 in cooperation with the European Childhood Obesity Group, German Society of Pediatrics, German Society of Obesity, and the Childhood Obesity Task Force of the International Obesity Taskforce/World Health Organization. 8 The Canadian Pediatric Weight Management Registry published baseline data in 2015. 10 Since no such registry exists in the United States for youth with obesity seeking treatment, the Pediatric Obesity Weight Evaluation Registry (POWER) was developed to address current gaps about effective intervention strategies for the treatment of pediatric obesity in the United States.
POWER was established to serve as a centralized data repository for the ongoing collection and maintenance of demographic and clinical data from multicomponent PWM programs across the United States. POWER aims to identify best practices for PWM, to provide an infrastructure for prospective multisite clinical research and quality improvement initiatives on youth with obesity, and to contribute to the advancement of evidence-based guidelines for the most effective interventions to treat youth with obesity. The goals of the current study are (1) to describe the planning and implementation of a nationwide pediatric obesity treatment registry with regard to feasibility, infrastructure, site recruitment, governance, and financing; (2) to describe demographic and anthropometric data of youth with obesity from PWM programs across the United States, and (3) to describe characteristics of multicomponent PWM programs in the United States.
Methods
Feasibility
The Children's Hospital Association (CHA) sponsored the initiative, Focus on a Fitter Future (FFF), over a 6-year period (2008–2013). FFF brought together teams from 25 hospital-based, multidisciplinary, comprehensive PWM programs to explore best practices for the assessment and treatment of youth with obesity. Of interest was the development of a national registry of youth with obesity, participating in multicomponent PWM programs.
The POWER formally began in 2011 as a subcommittee of FFF with 13 participating sites. The initial project was a 2-year (2009–2010) retrospective cohort study demonstrating the feasibility of establishing a multisite registry. CHA hosted this initial registry of patient data through a secure electronic server. The retrospective cohort study reported baseline patient characteristics among 6737 treatment-seeking youth with obesity. 11 The success of this initial project validated the establishment of the prospective POWER.
Prospective Data Collection and Management
A highly reliable data collection and management system was identified as essential for establishing the prospective registry. This system includes data collection form design, data repository selection and build, data entry method (i.e., web-based data entry and/or electronic data file upload), data quality monitoring and cleaning, data extraction, and data summarization and analyses. Cincinnati Children's Hospital Medical Center (CCHMC) was selected as the Data Coordinating Center (DCC) for the prospective POWER centralized data repository site. The proposed DCC budget was $100,000 for the first 2-year phase of the prospective POWER study. A minimum of 20 enrolled sites each paying a $5000 enrollment fee were established as the target to cover these costs and begin collecting prospective patient data.
The POWER DCC then established important operating processes and standards for the prospective registry. The DCC is utilizing the Medidata Rave clinical data management system, 12 an industry-leading software system for capturing and managing clinical data. Participating sites submit a specified set of required and optional data elements for baseline patient and follow-up patient visits (Table 1). Follow-up visit data are collected as they occur since there is no standardized practice for the frequency of these clinical encounters. Sites determine who is responsible for data entry (clinician, research assistant, nurse, etc.), which can be entered directly using a web-based interface or it can be uploaded using electronic data transfer to a secure server. Medidata Rave is configured to query sites if required data are omitted. Although double data entry is not done by the POWER sites, the DCC provides quarterly data monitoring to identify and resolve errant data to allow for early identification and resolution of systematic errors. Clinical and laboratory units are standardized and boundaries defined to identify outliers.
POWER Data Elements
Shaded cells, required data elements; Unshaded cells, optional data elements, but required if collected.
Required based on site-specific IRB approval.
Single/multiple providers in individual/group setting.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMV, baseline medical visit; BUN, blood urea nitrogen; GGT, gamma-glutamyl transferase; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; POWER, Pediatric Obesity Weight Evaluation Registry; T4, thyroxine; TSH, thyroid-stimulating hormone.
The DCC has access to all data collected at POWER sites, while each site can access their own site-specific data through the RAVE system. Deidentified aggregate data sets may be made available to individual sites in accordance with research proposals that have been vetted and approved by the POWER Governance Board, including applicable Data Use Agreements.
Site Enrollment
The CHA hosted three informational webinars in 2013 to recruit eligible sites. The webinars were advertised to over 600 individuals affiliated with pediatric institutions that offer multicomponent PWM programs. Results of the retrospective POWER cohort study were presented at two national conferences,13,14 which offered additional opportunities for site recruitment.
Inclusion criteria for POWER sites are programs that (1) provide multicomponent PWM treatment for youth with obesity; (2) collect the required data elements; and (3) ensure staff availability to collect and submit data to the POWER DCC. To enroll, each site was required to obtain Institutional Review Board (IRB) approval of the POWER study protocol that included obtaining informed consent/assent from patient families. Each site also had to submit a fully executed POWER Data Coordination and Use Agreement (DUA) and pay the $5000 enrollment fee for a 2-year contract. The POWER study is registered with ClinicalTrials.gov (Protocol #: NCT02121132).
POWER Governance Structure and Operations
The POWER governance structure supports an organized, participatory, and transparent decision-making process (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/chi). This structure encourages participation from all sites through monthly POWER Work Group webinars. A 14-member POWER Governance Board, directed by the POWER study's Principal Investigator, makes final decisions for the registry. Five subcommittees guide specific work within the registry, including policies and procedures, data elements, reporting on outcomes, funding opportunities and research, and communications. The POWER committees’ goals and accomplishments are summarized in Supplementary Table S1.
A POWER internal website is used to post calendar events and facilitates communication among participating sites. The password-protected internal website is also used to share quarterly reports on patient outcomes for the aggregate POWER dataset (Supplementary Table S2). Enrolled POWER sites can access protected files for their site-specific outcomes for comparison with the aggregate statistics for all sites. In addition, an external POWER website provides information about participating POWER sites, the POWER governance structure, a recorded POWER informational webinar, and enrollment criteria and contact information for sites interested in joining POWER.
Patient Enrollment and Data Collection
The target patient population is treatment-seeking youth with obesity. The accessible sample is youth with obesity presenting for treatment at enrolled POWER sites. Patient inclusion criteria are youth aged 18 years and younger with obesity (age- and sex-specific BMI ≥95th percentile based on CDC 2000 growth charts 15 ) and ability to consent in English or Spanish. Enrolled patients are further classified as having severe obesity if the following criteria were met: BMI between 120% and 140% of the 95th percentile or a BMI between 35 and 39, whichever was lower (Class 2), or patients with a BMI ≥140% of the 95th percentile or a BMI ≥40, whichever was lower (Class 3). 16 No further inclusion or exclusion criteria are applied. POWER is designed as an ongoing registry, thus sample size has not been specified a priori.
Patient enrollment in POWER began in May 2014. Data were included in this baseline descriptive analysis for patients enrolled between May 2014 and December 2015. The protocol established for patient enrollment in POWER is as follows: (1) Patients and parent/guardian are approached at the time of an initial medical evaluation for consent and assent for youth when age-appropriate. In the event eligible patients are not approached at the initial medical visit, the site study team could approach them at their next follow-up clinic visit or attempt to obtain consent by phone. (2) After consent/assent is obtained, demographic and clinical data elements (Table 1) from the initial medical visit and all subsequent follow-up visits are collected prospectively and submitted to the POWER DCC as a limited dataset in accordance with HIPAA (Health Insurance Portability and Accountability Act) regulations. POWER's data elements are classified as required or optional (Table 1). Required data elements must be collected and reported for each visit, whereas optional data elements (such as laboratory values) are reported when collected as part of the program's standard clinical protocol.
Quality assurance procedures for patient data collection are specified in the Data Definitions Document for POWER, which was developed by the POWER Data Elements Committee (Supplementary Table S1). This document provides detailed criteria for measuring and recording study data, including height, weight, waist circumference, and resting blood pressure assessments. For these measurements, the document also includes recommendations for equipment type and sizing, as well as patient positioning, measurement, and recording. In addition, standardized unit values are given for all laboratory measures as well as feasibility ranges for each outcome measure. Outcomes reported outside these ranges are automatically flagged within the Medidata Rave system and queries are generated, which require site review for confirmation or revision. When available, duplicate measures are individually recorded within the database to allow for calculations of site-specific measurements of reliability.
Each site retains the ability to fully identify individual patients when POWER data are needed for their medical care. If a patient opts to discontinue or becomes ineligible, the site enters the date that the subject discontinued the study and the reason for discontinuation. The DCC notifies a site if a patient enrolled in POWER has not been seen for 12 months and provides the patient ID to the site for follow-up.
For these descriptive analyses, frequency and percentages for patient demographics and weight status at baseline were determined for each site. The range and weighted averages of the percentages were calculated, weighted by the square root of the percent of patients at each site.
Program Profile Survey
POWER members developed a site survey to identify variation in PWM program design and other site-specific characteristics. This survey also included key components of evidence-based recommendations for the provision of care to youth with obesity. Domains included (1) program duration and intensity; (2) program provider types, (3) patient assessments; and (4) treatment strategies. In accordance with published standards, 4 program intensity was defined as hours of face-to-face patient contact over a 6–12-month period as the following: low intensity as <25 hours; moderate intensity as 25 to <75 hours; and high intensity as ≥75 hours. The program profile survey was administered electronically to POWER site leads by the POWER DCC through the Research Electronic Data Capture (REDCap) survey tool. Site leads completed the survey over a 6-month period (September 2014 to February 2015) within 1 year of enrollment. Sites offering more than one program completed a separate survey for each one. Survey responses were summarized and descriptive analyses reported using SAS version 9.2 (SAS Institute, Inc., Cary, NC).
Results
POWER Site Enrollment
In January 2014, 25 qualifying sites began the enrollment process for POWER. This included seven of the original 13 sites from the retrospective POWER cohort study. For the six original sites not continuing, barriers included the $5000 enrollment fee, need for staffing on site for data management and data entry, and other competing academic commitments. Since enrollment is ongoing for the prospective POWER study, outreach to these sites has continued so that they may enroll in the future.
By January 2016, 34 sites representing 22 states (Fig. 1) were in the process of enrolling, with 29 sites (85%) having completed the enrollment process during the first cycle of POWER (January 2014 to June 2016). After 6 months of planning, data submission started in June 2014 when the 20-site minimum enrollment was achieved. When enrollment reached 29 sites, the additional enrollment fees supported a 6-month extension of POWER's first cycle through June 2016. Site recruitment for the next 2-year cycle of POWER (July 2016 to June 2018) began in February 2016. As of July 2016, 30 sites (29 sites from the first cycle of POWER and 1 new site) have committed to participate in the next cycle of POWER.
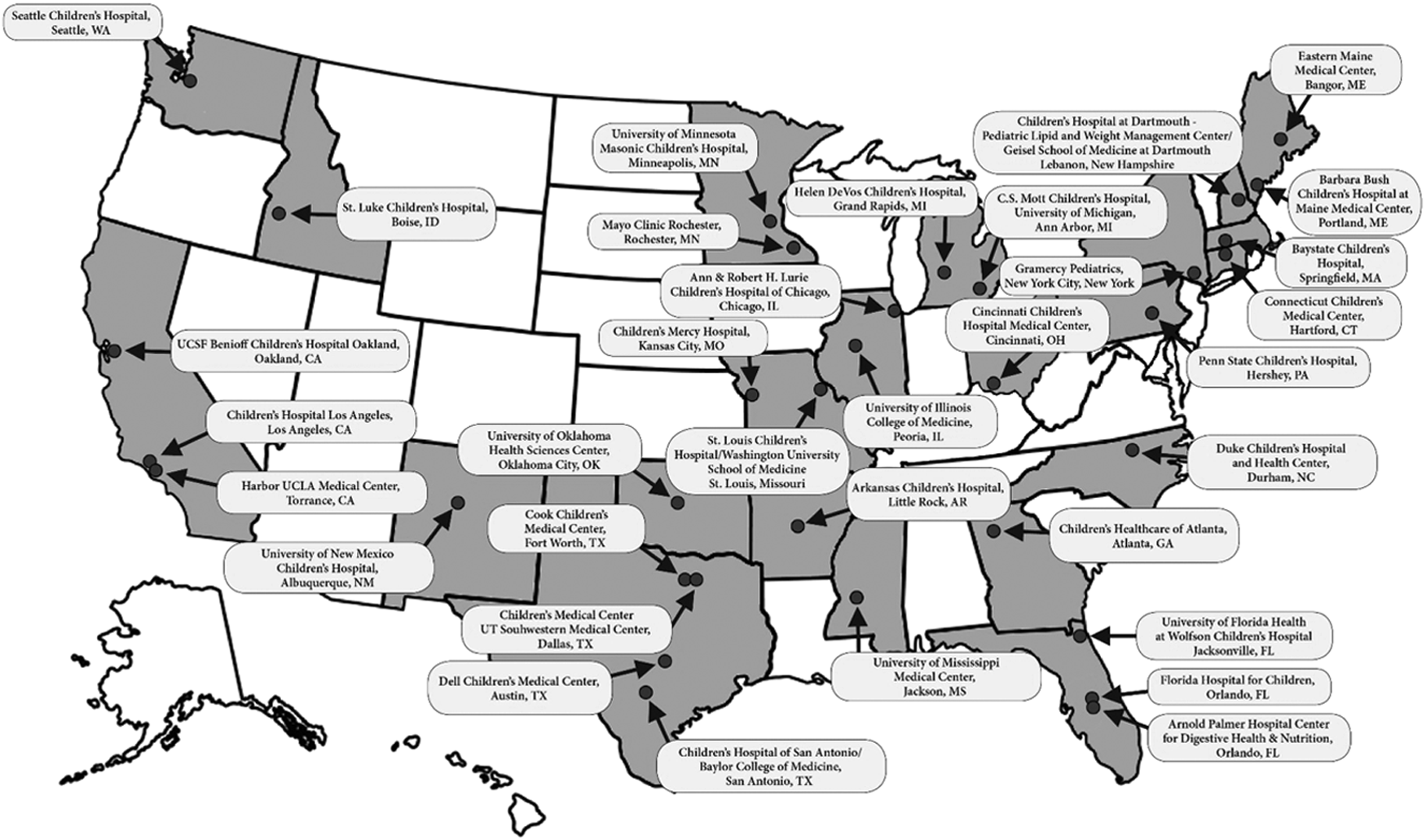
Sites participating in POWER (N = 34) up through December 2015. POWER, Pediatric Obesity Weight Evaluation Registry.
Baseline Characteristics of Patients Enrolled in POWER
Those enrolled in the POWER between June 2014 and December 2015 included 3643 unique patients with obesity from 26 sites (Table 2). The majority of patients enrolled are publicly insured and over two-thirds have severe obesity. The patients in POWER are racially and ethnically diverse; one-third of patients are nonwhite and one-third Hispanic.
POWER Baseline Patient Characteristics
Patient data collected from 26 POWER sites.
Weighted by square root of percent of patients at each site.
Weight status: Percent of the 95th percentile for BMI and/or BMI (kg/m2).
Obesity (Class 1): 100–120% of 95th percentile for BMI and BMI <35.
Severe Obesity (Class 2): 121–140% of 95th percentile for BMI or BMI = 35–39, whichever is lower.
Severe Obesity (Class 3): >140% of 95th percentile or BMI ≥40, whichever is lower.
BMI, body–mass index.
Required data elements (Table 1) were reported for over 99% of patients at baseline and follow-up visits. During the first 18 months of data collection, 65% of patients had at least one follow-up visit (median = 1 visit; interquartile range = 1–3 visits). For the optional data elements (Table 2), blood pressure measurement was reported at baseline for over 95% of subjects. Sexual maturity rating and body composition were reported for about 50% of subjects. Rarely reported measures (<20% of subjects) included hip and waist circumference measurements and mother's education. At least one medical diagnosis was reported for 34% of patients and at least one medication was reported for 11% of patients. Laboratory measures were reported as available; 79% of subjects had an initial laboratory value and 54% had at least one laboratory value at a follow-up visit. The most frequently reported laboratory measures were glucose, hemoglobin A1c, lipid profile, or liver profile, whereas TSH and 25-OH vitamin D were reported only occasionally.
POWER Program Profile
During the first cycle of POWER, the program profile survey was completed by 28 of the 29 sites contacted, representing 20 states. One site reported on two different multicomponent program offerings, one hospital based and the other community based, which resulted in a total sample size of 29 programs.
Program size
Site size is classified by the number of patients enrolled in POWER. Of the 26 sites that submitted patient data up through December 2015, 15 sites were classified as small (<100 patients), 7 sites were medium (100 to <200 patients, n = 7), and 4 sites were large (≥200 patients).
Program duration and intensity
Of the 23 PWM programs reporting interventions of specific duration, 22 (96%) offer at least 6 months of behaviorally based lifestyle modification therapy, with one program offering a 12-week group intervention. Only 5 (17%) of the programs have a fixed duration. The most common reasons that programs purposefully vary treatment duration include the presence of obesity-related comorbidities (n = 21; 72%), patient–family level of motivation (n = 20; 69%), and severity of obesity (n = 19; 65%).
The majority of programs (n = 15; 52%) provide only low intensity services, while fewer programs (n = 5; 17%) provide only moderate intensity services. Only one (3%) of the POWER sites offered a high intensity program. Eight (28%) of the programs provide more than one level of intensity. While current obesity treatment recommendations include offering a moderate to high intensity PWM program for optimal effectiveness, only 13 programs (45%) met this criteria. Sites reported that the program intensity level recommended to patients was most affected by the following factors: severity of obesity, obesity-related comorbidities, motivation, patient–family proximity to the program, and/or whether bariatric surgery is being considered.
Program provider types
Of the 27 programs reporting, all included one or more medical providers (i.e., physician or certified nurse practitioner), while other provider types varied across programs (Table 3). Certifications relevant to PWM also varied among providers in POWER. For medical providers (N = 99), 12% were certified by the American Board of Obesity Medicine, and for registered dietitians (N = 56), 48% earned the Certificate of Training in Childhood and Adolescent Weight Management. Motivational interviewing, a patient-centered counseling strategy recommended for facilitating change of obesity-related behaviors, 4 was the advanced training most frequently reported across all provider types: medical providers (41/99 = 41%); registered dietitians (25/56 = 45%); psychologists (23/28 = 82%), social workers (11/21 = 52%), exercise physiologists (5/21 = 24%); physical therapists (5/15 = 33%); and health educators (6/9 = 67%).
Combination of Provider Types in PWM Programs in POWER (N = 27)
Provider types: medical provider (physician or certified nurse practitioner);
EP, exercise physiologist; HE, health educator; PSYCH, psychologist; PT, physical therapist; PWM, pediatric weight management; RD, registered dietitian; SW, social worker.
Patient site-specific eligibility criteria
Of the 25 programs responding to this survey question, all included weight status as referral criteria. The weight status criteria used included the following: >85th percentile for BMI (n = 14; 56%); >95th percentile for BMI (n = 9; 36%). Participation criteria for two programs (8%) combined weight status with the presence of an obesity-related comorbidity.
Patient assessments
Programs reported using a variety of psychological and physical fitness assessments for patients. The most common psychological instruments used included the Pediatric Symptom Checklist-17 17 (n = 9; 31%) and Pediatric Quality of Life Inventory 18 (n = 9; 31%). The most commonly used physical fitness tests were the 6-minute walk test 19 (n = 7; 44%), maximal or submaximal treadmill study (n = 6; 38%), and 3-minute step test 20 (n = 5; 31%).
Treatment strategies
For the initial dietary approach, a nutrient-balanced portion-controlled diet was the most common dietary approach used by programs (n = 24; 83%). However, 13 different dietary approaches were reported as initial options for weight management across the 29 PWM programs, with the most commonly reported as mindful eating strategies 21 (n = 10; 34%); calorie-defined plan, 1200–1800 kcal/day (n = 6; 21%); DASH (Dietary Approach to Stop Hypertension)-type diet for youth 22 (n = 6; 21%), and reduced glycemic load diet23,24 (n = 3; 10%).
Ten (34%) of the programs offered pharmacotherapy for obesity management, with metformin identified as the most commonly used medication to specifically facilitate weight loss (n = 9; 31%). Fifteen (54%) of the 28 POWER sites offered weight-loss surgery. Specific procedures include vertical sleeve gastrectomy (n = 11 sites; 39%), Roux-en-Y gastric bypass (n = 7 sites; 25%), and laparoscopic gastric banding (n = 4 sites; 14%).
Discussion
POWER has been successfully established as the first US-based multicenter registry of treatment-seeking youth with obesity. As of December 2015, 26 POWER sites have submitted data on 3643 youth with obesity. Currently, 30 sites have formally committed to ongoing participation (July 2016 to June 2018). The descriptive analyses for this large sample of youth with obesity highlight several notable strengths of this registry.
First, POWER's geographically diverse sites across the United States provide a racially and ethnically diverse cohort, with the majority being publicly insured. Although rates of obesity are increasing in youth from all ethnic and racial groups, disparities exist and the prevalence of obesity is higher in nonwhite and lower-income groups, particularly for severe obesity. 25 The reasons for differences in prevalence of pediatric obesity among racial and ethnic groups are not fully understood, but likely involve a complex interplay among genetics, physiology, culture, socioeconomic status, and environment, as well as other factors that are not fully recognized. POWER is well positioned to increase understanding of the influence of these variables on health behavior patterns and to understand the predictors of treatment success across different populations.
Second, nearly 75% of the POWER cohort comprises youth that present with severe obesity. The prevalence of this group in the US population is still increasing. 26 Additionally, youth with severe obesity are much more likely to develop health complications secondary to their obesity 27 compared with youth with less severe degrees of obesity. 2 The POWER cohort offers a unique opportunity to study this high-risk group.
Third, the results of the program profile survey show a broad diversity of program design and treatment practices among POWER sites. Together with the consistent collection of high-quality patient outcome data, this diversity of PWM program design and implementation provides a natural experiment for identifying best practices for improving the treatment of pediatric obesity and its related comorbidities. Current obesity treatment recommendations include offering a moderate to high intensity PWM program for optimal effectiveness, yet only 45% of PWM programs in POWER offer this. Thus, there is a discrepancy of what is ideally recommended over what is available. This raises questions of how to establish more intensive programming nationally so that comparisons of outcomes among different program intensities can be made. POWER is positioned to help answer these questions.
The structure of POWER creates a collaborative environment in which hypotheses related to best practices can be formulated and tested with high-quality, multisite clinical trials with large sample sizes of adequate power. Future POWER studies will identify associations between characteristics of PWM programs, patient characteristics, and health outcomes. Another important benefit for POWER sites is the quarterly POWER data reports on key health outcomes and process measures, which can help track the impact of both site-specific and multisite quality improvement initiatives.
Challenges facing POWER include the need for ongoing funds to cover the cost of DCC activities and additional larger scale studies, such as multicenter clinical trials. Funding would also be beneficial to support staff at each site for patient enrollment and tracking, data entry, and effort of site that leads to fully participate in POWER. More resources could also help broaden the scope of data elements collected, which in turn could better characterize the treatment of pediatric obesity and associated patient outcomes.
Conclusion
POWER is an established national registry representing a diverse sample of youth with obesity participating in multicomponent PWM programs across the United States. A strength of POWER is its high representation of low-income, racially, and ethnically diverse patients, as well as those with severe obesity. Participating POWER sites reflect the variation in mode and method of care delivery of PWM programs. POWER aims to identify best practices for PWM, to provide an infrastructure for prospective clinical research and quality improvement initiatives on pediatric obesity, and to contribute to the advancement of evidence-based guidelines for the most effective interventions to treat youth with obesity.
Footnotes
Acknowledgments
The authors gratefully acknowledge the administrative support provided by program coordinator, Deborah Wolff, BS, and technical support provided by regulatory specialists, Alison Wheeler, BA, and Halley Estridge, BS, CCRP, and project manager Diana McClendon, MSW, MPH, with the Heart Institute Research Core, CCHMC. In addition, database programmers, Michael Kuhlmann, BS, and Stacy France; data specialist, Carolyn Powers, BS, RD, CCDM; SAS programmer, Yanhong Liu, MS; and manager, Rachel Akers, MPH, CCDM, with the POWER Data Coordinating Center in the Division of Epidemiology and Biostatistics, CCHMC, have made important contributions to the management and analysis of the POWER data.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.