
Abstract
Abstract
Background:
As a group, bottle-fed infants are at higher risk for rapid weight gain compared with breast-fed infants. However, little is known about individual differences in feeding behaviors of bottle-feeding infants, as well as maternal and infant characteristics associated with bottle-feeding outcomes.
Methods:
We conducted a 2-day, within-subject study of 21 formula-feeding dyads; the within-subject factor was feeding condition: mother-led (ML; mothers were given the instruction to feed their infants as they typically would) vs. infant-led (IL; the experimenter ensured feeding began when infants signaled hunger and ended when they rejected the bottle on three consecutive occasions). Intake was determined by bottle weight; feedings were video-recorded and later analyzed to determine feeding duration and types of satiation behaviors displayed. Percent difference scores were calculated for each outcome as [((ML – IL)/IL) × 100] to standardize differences among dyads. Mothers completed questionnaires of feeding styles and infant temperament.
Results:
On average, infants consumed ∼42% more formula during the ML- than IL-condition (p = 0.03). However, notable variation existed in difference scores for intake (range = −52.8% to 268.9%; higher scores reflect greater intake during ML than IL). Stepwise regression illustrated that greater intakes during the ML-condition were predicted by the combination of: (1) higher infant age; (2) lower levels of infant rhythmicity and adaptability; (3) higher levels of infant positive mood; and (4) lower levels of maternal restrictive and responsive feeding styles.
Conclusions:
This objective, experimental approach illustrated that variation in bottle-feeding outcomes is associated with characteristics of both members of the dyad.
Introduction
Infants who feed from a bottle are more likely than those who breastfeed to exhibit rapid rates of growth during the first year postpartum,1–3 a known risk factor for childhood and adult obesity and other comorbidities.4–8 One likely mechanism underlying rapid rates of growth is that formula-fed infants consume more per feeding and over the course of a day than breast-fed infants. 9 Such overfeeding may occur, because infants exert less control when feeding from a bottle, because their mothers are more responsive to contextual cues (e.g., amount in the bottle) than to their infants' hunger and satiation cues, or both.10–12
Despite these widely held hypotheses, research, although limited, suggests that bottle-feeding does not uniformly place infants at risk for overfeeding11,13,14 and excess weight gain. 13 From the perspective of the infants, those who feed from a bottle are sensitive to what is in the bottle (e.g., the composition of the formula), and will modify intake accordingly.15,16 Further, bottle-fed infants can communicate hunger and satiation, but individual differences exist in the extent to which and the ways in which they communicate during feeding. 14 Likewise, from the perspective of the mothers, some are more responsive to signals of hunger and satiation by their infants than others,17,18 and individual differences in infant feeding beliefs and practices exist and are associated with maternal characteristics, such as race, ethnicity, and obesity.19,20
To further our understanding of the dynamics of the mother–infant dyad during bottle-feeding and to identify which infants may be at risk for overfeeding, the present study used an experimental paradigm that measured infants' feeding and satiation behaviors during two conditions: (1) a “mother-led” (ML) feeding condition, wherein mothers were instructed to feed their infants as they typically would; and (2) an “infant-led” (IL) feeding condition, wherein maternal influences were minimized and the experimenter ensured that feeding began when the infant signaled hunger and ended when the infant signaled satiation by rejecting the bottle on three consecutive occasions.16,21,22 Using this within-subject and experimental approach, we aimed at directly assessing how the conditions of feeding and individual differences in characteristics of the infants (e.g., temperament; behavioral displays during feeding) and their mothers (e.g., weight status, feeding styles) relate to bottle-feeding outcomes.
Subjects and Methods
Participants
Twenty-one mothers, whose healthy infants were formula-feeding, were recruited through ads in local newspapers, websites, and Philadelphia Women, Infants, and Children (WIC) offices. Inclusion criteria included that infants were born full term and did not have any medical conditions that interfered with feeding. Six additional dyads were recruited but then excluded because they either did not complete both testing days or did not comply with study procedures. All study procedures were approved by the Office of Regulatory Affairs at the University of Pennsylvania, and informed consent was obtained from each mother at study entry. This trial was registered at clinicaltrials.gov as NCT02284152.
Methods
Each mother–infant dyad was tested at the same time of day on 2 test days separated by 2.1 ± 0.4 days. The 2 testing days were scheduled to occur at a time of day that each infant typically consumed formula. After acclimating to the room and personnel for ∼1 hour (average = 59.6 ± 34.3 minutes), infants were video-recorded while their mothers fed them. Videos were captured using a video camera that was placed ∼12 feet in front of the dyad. The researcher remained in the room but was hidden behind a partition, out of view of the dyad, during the feeding. The researcher monitored the feeding via a monitor that was placed behind the partition and also out of view of the dyad. On both days, infants were fed the formula that they were currently feeding (e.g., Similac™, Good Start Gentle Plus™, Good Start Soy™) and from the type of bottle with which they were familiar. So that mothers would be blind to the hypothesis and not be influenced by experiencing the IL feeding paradigm, the first day of testing was always the ML-condition in which mothers were only given the instruction to “Please feed your infant as you normally would at home.” The second day of testing was the IL-condition, which used a protocol that enables infants to control the pace and duration of feeding16,21,22 and minimizes maternal influences on infant feeding behaviors.23,24 In brief, during the IL-condition: (1) feeding sessions began when infants displayed signs of hunger (e.g., mouthing, rooting, fussing) and mothers verified that their infants were hungry; (2) mothers were instructed not to talk to their infants and to remain as neutral as possible; (3) mothers were instructed to feed at an IL pace (i.e., guided by infant feeding cues); and (4) feeding sessions ended when infants displayed signs of fullness (e.g., turning head and/or body away from the bottle, biting or chewing on the nipple, spitting the nipple) on at least three consecutive occasions. Formula intake (g) was determined by weighing the bottle both before and after each feeding, which was then converted to volume (mL) assuming a formula density of 1.03 g/mL.25–27
Video-Record Analyses
Each video-recorded feeding (N = 42) was later analyzed frame by frame using an event recorder program (Observer XT, version 10.5, Wageningen, The Netherlands) to determine the duration of feeding and the frequency, timing, and type of behaviors infants used to signal satiation. For each video, we focused on the second half of each meal. Raters (N = 2) coded 11 mutually exclusive behavior types (see Ventura et al. 14 for more detail): (1) waves arm(s); (2) displays negative facial expressions; (3) leans away or arches back; (4) turns head and/or body away from bottle; (5) bites or chews nipple; (6) pushes bottle away; (7) spits out nipple; (8) gags, coughs, or chokes; (9) spits out formula or spits up; (10) crying bout; and (11) sleeping bout.
Inter-coder reliability was established by the common scoring of a total of 10 feedings by both raters. The mean Pearson's rho for the correspondence between the frequency, timing, and type of behaviors coded in each of the double-coded videos was ρ(8df) >0.80, indicating good reliability between raters.
Characteristics of Mothers and Infants
Mothers were queried on sociodemographic characteristics and completed questionnaires to obtain measures of infant temperament (the Infant Temperament Questionnaire28,29) and maternal feeding styles (the Infant Feeding Styles Questionnaire 30 ). Because we aimed to identify characteristics of mothers and infants that explained individual differences in intake and feeding behaviors of the infant during the two conditions, our analyses focused on the temperament subscales that describe infant behaviors during feeding: activity level, rhythmicity, approach, adaptability, and mood28,29; and on the three maternal feeding styles that are the most applicable to bottle-feeding infants: (1) pressuring, defined as the extent to which the mother encourages her infant to finish the bottle and uses food as a soothing method; (2) restrictive, defined as the extent to which the mother limits the infant's intake; and (3) responsive, defined as the extent to which the mother recognizes and feeds in response to her infant's hunger and satiation cues. 30
Infants' weight and recumbent length were measured in triplicate by using standard anthropometric techniques, 31 a scale accurate to 0.1 kg (Scale Tronix, White Plains, NY), and an infantometer accurate to 0.1 cm (Harpenden Infantometer 702, Crymych; Dyfed). Mothers' weight and height were also measured in triplicate 31 (Health-O-Meter; Sunbeam Products, Inc., Boca Raton, FL). Infant weight and length measures were normalized to age- and sex-specific z-scores [i.e., weight-for-age z scores (WAZ)], 32 and maternal BMI (BMI = weight in kg/height in m2) was determined.
Statistical Analysis
Analyses were conducted using SAS, version 9.4 (SAS Institute, Inc., Cary, NC). Data were first assessed for normality. Distributions for the number of satiation behaviors displayed during the second half of the feedings were positively skewed; thus, they were normalized by using log transformations before analyses. After analyses, data were back-transformed by calculating the antilog or square of the estimate. 33
For both conditions, outcome measures included infant intake (mL), intake per kilogram of body weight (mL/kg), meal duration (minutes), rate of feeding (mL/min), number of satiation behaviors displayed during the second half of the feedings, and latency to first satiation behavior during the second half of the feedings. We then conducted repeated-measures analysis of variance (ANOVA) with condition (ML vs. IL) as the within-subject factor to determine whether these measures differed by feeding condition. Time elapsed since the last feeding and infant age were included as time-varying covariates in all repeated measures ANOVA models.
Second, we examined individual differences in the discrepancy between the ML- and IL-conditions by calculating, for each infant, a percent difference score for each outcome measure [((ML – IL)/IL) × 100]; this allowed us to standardize differences between the ML- and IL-conditions across infants. Higher percent difference scores reflect greater response (e.g., greater intake or number of satiation behaviors) during the ML- when compared with the IL-condition. Binomial distribution tests were used to determine whether the proportion of infants who showed greater response during the ML- than IL-condition was greater than chance. t-Tests were used to determine whether each percent difference score was greater than zero.
Third, to explore which infants were at higher risk for feeding more during the ML-condition, stepwise regression was used to determine the combination of infant and maternal characteristics that best predicted percent difference scores for intake (% DIFF-intake). The infant and maternal variables entered into the stepwise regression analysis were those previously associated with infant risk for overfeeding and rapid weight gain.17–20,34–39 The order of entry for each model variable was determined by the strength of the association between each predictor and the outcome and, with each iteration of the analysis, the most significant variable was added or the least significant variable was removed. 40 Results are presented as means or least squared means ± standard errors (SEs). p-Values <0.05 indicated significant effects, and p-values <0.10 indicated trends.
Results
Sample Characteristics
Table 1 presents the dyads' characteristics. The infants (13 girls, 8 boys) were, on average, 21 weeks (4.8 ± 0.5 months) of age and had an average WAZ of 0.4 ± 0.2. The mothers (61.1% multiparous) were, on average, 28.0 ± 1.4 years of age and had a mean BMI of 29.0 ± 1.1; 24% were classified as overweight, and 48% were classified as obese. The majority of mothers was non-Hispanic Black (62%) and had a high school degree or higher (81%). Approximately half (52%) reported an annual family income >$35,000.
Participant Characteristics (N = 21)
SE, standard error; WAZ, weight-for-age z-score; ΔWAZ, change in weight-for-age z-score.
Infant Intake and Rate of Feeding
There was no difference between conditions for time elapsed since the last feeding (ML: 2.6 ± 0.1 hours vs. IL: 2.8 ± 0.2 hours; p = 0.47); testing occurred, on average, 2.7 ± 0.1 hours since the previous feeding. When we compared how much formula infants fed and their rates of feeding during the ML- and IL-conditions at the level of the group, differences between conditions for formula intake (mL), intake per kilogram of body weight (mL/kg), and meal duration (minutes) did not reach significance (Table 2). However, infants trended toward exhibiting a greater rate of feeding (mL/min) during the ML- compared with IL-condition (p = 0.09). On average, infants consumed 139.9 ± 9.6 mL of formula per feed (20.3 ± 1.5 mL/kg) at a rate 16.7 ± 2.1 mL/min; the formula meal lasted 10.0 ± 0.8 minutes.
Least-Squared Means (SE) for Infant Feeding Behaviors during Mother-Led and Infant-Led Conditions (n = 21)
For the mean difference between the IL and the ML feeding; all models were controlled for time since last feeding and infant age.
Percent difference score, calculated as [(ML − IL)/IL] × 100.
For t-tests to determine whether the percent difference score was significantly different than zero.
% DIFF, percent difference score; IL, infant-led; ML, mother-led.
When differences between the ML- and IL-conditions were standardized across infants, there was a wide variation in how condition (ML vs. IL) modified infant feeding outcomes. As shown in Figure 1, the percent difference scores for intake (% DIFF-intake) during the ML- compared with the IL-condition ranged from −52.8% to 268.9%; recall positive scores indicate that the infant consumed more during the ML-condition compared with the IL-condition, whereas negative scores indicate that the infant consumed less. Sixty-seven percent of infants (14 of 21) consumed more during the ML- than IL-condition; this proportion trended toward being significantly different from chance (p = 0.09). The average % DIFF-intake score (41.8% ± 17.8%) was significantly greater than zero [t(20) = 2.35, p = 0.03; Table 2]. Results did not change when we accounted for the body weight of the child (i.e., intake/kg; p = 0.04). Percent difference scores for rate of feeding were also significantly greater than zero (p = 0.01).
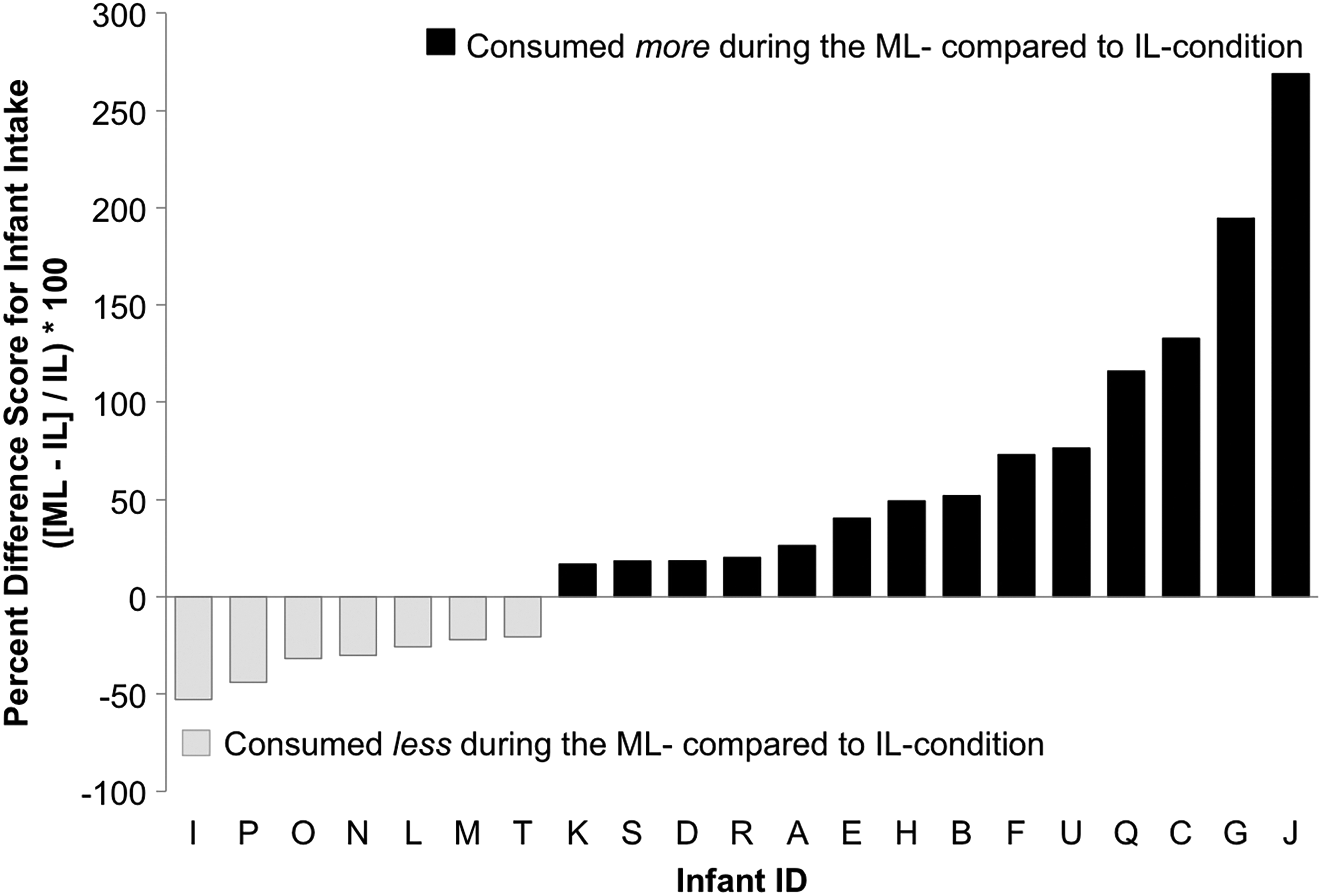
Percent difference scores for infants' intakes during ML vs. IL feeding conditions. Percent difference is defined as [(ML – IL)/IL] × 100. ML, mother-led; IL, infant-led.
Infant Satiation Behaviors
Infants were consistent in the overall number, frequency, and timing of satiation behaviors displayed during the second half of the ML- and IL-conditions (Table 2). In addition, the latency to display the first satiation behavior did not differ between the two conditions (p = 0.62). When considering each satiation behavior individually, there were no significant differences in the frequency of 10 of 11 behaviors (i.e., waving arms; negative facial expressions; leans away or arches back; turns away from bottle; bites or chews nipple; pushes bottle away; spits out nipple; gags, coughs, and chokes; spits out formula or spits up; crying bout; or sleeping bout; all p > 0.05). Displays of leaning away or arching back was displayed significantly fewer times during ML- than IL-condition (0.2 ± 0.1 vs. 1.7 ± 0.5 displays, respectively; p = 0.01). On average, infants displayed 13.7 ± 1.1 satiation behaviors, which began 6.1 ± 3.3 minutes after the start of the feeding.
The number of satiation behaviors displayed during ML-condition was significantly and positively associated with the number of satiation behaviors displayed during IL-condition [r(19) = 0.42, p = 0.05], suggesting a consistency in the behavioral phenotype of the infant. The number of satiation behaviors displayed during each condition was not associated with how much formula the infant consumed during that particular condition (ML: p = 0.47 and IL: p = 0.64).
When differences between the ML- and IL-conditions were standardized across infants, the percent difference scores for each infant's satiation behaviors displayed during the second half of ML- compared with IL-condition (% DIFF-behaviors) ranged from −94.3% to 320.0% (mean = 6.9 ± 21.8%); recall positive scores indicate that the infant displayed more satiation behaviors during the second half of the ML- compared with the IL-condition, whereas negative scores indicate that the infant displayed fewer. Sixty-two percent (13 of 21) of infants displayed more behaviors (i.e., had a positive % DIFF-behaviors scores) during the ML- than the IL-condition; this proportion was not significantly different from chance (p = 0.19). In addition, the average % DIFF-behaviors score was not significantly greater than zero [t(20) = 0.32, p = 0.75].
Predictors of Percent Differences in Intake During ML- vs. IL-Feeding Conditions
Stepwise multivariate regression was used to explore which combination of mother and infant characteristics best predicted infants' % DIFF-intake. Predictor variables included % DIFF-behaviors; infants' age and WAZ at testing, and temperament scores; and mothers' age and BMI at study entry, and levels of pressuring, restrictive, and responsive feeding styles. Table 3 illustrates the best-fit model for prediction of % DIFF-intake scores.
Final Regression Model Predicting Percent Difference for Infant Intakes (% DIFF-Intake) a during Mother-Led vs. Infant-Led Conditions
Model F-value = 6.66, p = 0.0021. Model R2 = 0.75.
Percent difference scores for infant's formula intake during ML vs. IL feeding = [(ML – IL)/IL] × 100.
Higher scores = greater levels of restrictive or responsive feeding style; from the Infant Feeding Styles Questionnaire. 28
p < 0.05; **p < 0.01.
ML, mother-led; IL, infant-led.
The final model explained 75.4% of the variance in infants' % DIFF-intake and was statistically significant [F(6,19) = 6.66, p = 0.0021]. The variables that remained in the final model included infants' age, mothers' perceptions of infants' level of rhythmicity, adaptability, and mood, and mothers' level of restrictive and responsive feeding style. This model suggests that greater infant intakes during the ML- than the IL-condition were predicted by the combination of: (1) older age of infant; (2) lower levels of infant rhythmicity and adaptability; (3) higher levels of infant positive mood; and (4) lower levels of maternal restrictive and responsive feeding styles.
Discussion
The present research illustrated a novel approach to study infant behaviors and satiation during bottle-feeding, which can be used to identify sources of individual differences in bottle-feeding outcomes. We illustrated that infants can and do signal satiation during bottle-feeding and are consistent in their display of satiation behaviors during different feeding conditions. Although how much formula infants consumed and how long they spent feeding in the present study were characteristic of infants in this age range,9,14,16,41 we noted wide variation in infant feeding outcomes when comparing ML with IL feeding conditions. This variation was associated with characteristics of both members of the dyad.
Our exploration of the maternal and infant characteristics that was associated with variation in formula feeding outcomes provides some insights into our understanding of which dyads are at higher vs. lower risk of consuming more during typical, ML feeding conditions compared with IL-conditions. With respect to maternal characteristics, we noted significant associations between mothers' self-reported feeding styles and infants' relative intake during ML- vs. IL-conditions. Specifically, higher levels of restrictive feeding style were associated with lower intakes, whereas lower levels of responsive feeding style were associated with higher intakes during the ML- compared with the IL-condition. These findings are consistent with previous research illustrating that restrictive feeding styles are associated with lower daily energy intake for infants, whereas feeding styles that are less responsive to infant hunger and satiation cues are associated with greater daily energy intake. 39
In addition, although it is commonly reported that responsive feeding is characteristic of breastfeeding mothers and controlling or restrictive feeding is more characteristic of bottle-feeding mothers;10,42–45 our study illustrates that this dichotomy may oversimplify associations between feeding mode and feeding styles. Rather, among our sample of bottle-feeding mothers, we noted variation in mothers' level of restrictive and responsive feeding styles and that greater levels of responsive feeding and lower levels of restrictive feeding were associated with a closer match between ML and IL feeding conditions for feeding outcomes—in other words, for some bottle-feeding mothers, the ML feeding was essentially an IL feeding, likely because these mothers fed in response to their infants' cues. Thus, bottle-feeding and responsive feeding are not mutually exclusive, and future studies should aim at understanding how to promote responsive feeding styles for all mothers who choose to bottle-feed. 46
When considering infant characteristics, we found that older age, lower levels of rhythmicity and adaptability, and more positive mood were predictive of greater intakes during ML- compared with IL-conditions. These associations are consistent with previous research illustrating that what the child “brings to the table” may influence the dynamics of feeding and be determined, in part, by the children's past experiences with their caregivers during feeding.22,36,47,48 For example, it is well documented that children learn to overeat in response to parent feeding practices that are overly restrictive or prompt children to eat in the absence of hunger (see Rollins et al. 49 for a review); similarly, our finding that older infants had greater discrepancies between ML compared with IL feeding conditions may represent the greater experience that older infants have with their mothers' feeding styles, resulting in a learned tendency to consume more during ML feeding.
A growing body of research has also recognized associations between child temperament and both children's eating behaviors34–38 and parents' feeding practices.50,51 This research has highlighted that children who score higher on measures of temperamental surgency or impulsivity also show greater food responsiveness and risk for overeating,34,35,37,38 whereas children who score higher on measures of temperamental difficulty or negativity have parents who report greater use of food to soothe and are at greater risk for overfeeding.50,51
Consistent with these findings, our analyses revealed that dimensions of surgency/impulsivity (i.e., greater levels of positive mood 52 ) and difficult/negative temperament (i.e., lower levels of rhythmicity and adaptability 28 ) were predictive of greater intakes during ML compared with IL feeding conditions. However, given that our measure of temperament was self-reported by mothers, it is unclear whether infant temperament is a driver of mothers' feeding practices and infant intake, or whether mothers' perceptions of their infants' temperament are shaped by feeding interactions and outcomes. 22 Further research that appreciates what both mothers and infants contribute to feeding interactions is needed to better understand causal mechanisms linking maternal and infant characteristics and feeding outcomes.
It is likely that additional factors not assessed in the present study also contributed to individual differences in feeding outcomes, and some aspects of our methodology (e.g., the order of conditions and conditions of testing) may have contributed to variation in feeding outcomes. First, we intentionally designed our study such that the ML-condition preceded the IL-condition in an attempt to minimize mothers' expectations regarding how they should feed their infants. However, it is possible that some of the infant behaviors observed on the first day of testing (e.g., faster suck rates) may have been in response to the novel feeding setting, rather than in response to the mothers' feeding behaviors.
Second, we used an established protocol to create an IL feeding condition, wherein the feeding occurred in response to infant hunger and fullness cues and the influence of the mother was minimized, in an effort to allow the infant to express behaviors that typical ML feeding conditions may inhibit or modify. However, it is possible that mothers' lack of talking and maintained neutrality during the IL-condition caused infants to behave differently in response to the novelty of this condition.53,54 In line with this possibility, Lumeng et al. 23 illustrated that when 7- to 14-week-old infants were bottle-fed in an IL manner by trained research nurses, infants consumed 43% more formula when the nurses interacted with them compared with when the nurses were instructed to remain neutral, 23 indicating that social interaction was a driver of intake for young infants. Whether these findings translate to mother–infant interactions was not directly tested, but it is plausible that social interaction from mothers would similarly influence infant intake—for example, as a driver of faster sucking rates seen during the ML feeding—and that greater social interaction during the ML feeding conditions or variation in the degree to which mothers interacted with their infants may have led, in part, to variation in how much formula infants consumed.
It should also be noted that, although our small sample size allowed for in-depth coding of infant behaviors, it may have also led to Type II errors due to low power. Thus, further research that uses the approach illustrated in the present study, but also includes a larger sample size and observational measures of maternal behaviors, is needed to further understand the effects of mother–infant social interaction, mothers' feeding practices, and infants' characteristics on bottle-feeding outcomes in the short term, and infants' weight gain trajectories and developmental outcomes in the long term.
Conclusions
The experimental paradigm used here allows for the observational assessment of independent contributions of the infant and mother to short-term bottle-feeding outcomes. Our approach complements the research of others,1,2,23,55–57 in that we objectively assessed infant intake during a typical feeding, wherein mothers were given no instruction regarding how or how much to feed, and then compared feeding outcomes with an IL feeding paradigm during which infants determined the pace and duration of feeding and the influence of their mothers was minimized.16,21,22 This within-subject approach allows for observational measurements of the behaviors of infants and could be applied to similarly assess the behaviors of caregivers to better understand the unique contributions of each member of the dyad during bottle-feeding interactions.22,47,58–60 Further research using this paradigm has the potential to increase knowledge on how to improve feeding interactions and outcomes for bottle-feeding dyads.
Footnotes
Acknowledgments
The project described was supported by NIH grants R01HD072307 and R01HD37119; American Recovery and Reinvestment Act supplement 3R01HD037119-10S1; and National Research Service Award F32HD063343 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funding agencies had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the article. The authors thank Loma Inamdar, Mariya Keselman, Sehris Khawaja, Jillian Fink, Shawna Comalli, and Nicole Halfin (whose position was created by ARRA supplement 3R01HD037119-10S1) for technical assistance. They also thank Dr. Linda Kilby and the staff at the Philadelphia WIC Program for their assistance with subject recruitment.
Author Disclosure Statement
No competing financial interests exist.