
Abstract
Abstract
Background:
Little information is available regarding changes in adiponectin fractions. The objective of this study was to examine changes in the composition of differing adiponectin fractions using a population-based, prospective pediatric cohort.
Methods:
A total of 358 fourth graders (9–10 years old) from Ina town in Saitama, Japan, were followed up for 3 years. BMI and total adiponectin (TAD), high–molecular weight adiponectin (HAD), medium–molecular weight adiponectin, and low–molecular weight adiponectin levels were measured in these subjects at baseline and at the end of the follow-up.
Results:
Of the fourth graders participating in the study, 326 (172 boys and 154 girls; follow-up rate, 91.1%) became available for follow-up. No significant changes were observed in TAD values after 3 years. HAD values were significantly decreased in both the boys (2.4 to 2.2 μg/mL: p < 0.001) and girls (3.1 to 2.7 μg/mL: p = 0.005). All values in the parameters examined at baseline and after 3 years were significantly correlated. A negative correlation was found between the ratios of follow-up compared to baseline values for BMI and those for TAD (boys, r = −0.322, p < 0.001; girls, r = −0.433, p < 0.001) as well as those for HAD (boys, r = −0.353, p < 0.001; girls, r = −0.351, p < 0.001).
Conclusions:
HAD had the most robust correlation between its values at baseline and those after 3 years in both boys and girls. The changes in HAD also had the most robust correlation between the changes in BMI in 3 years.
Introduction
The prevalence of obesity in children is increasing throughout the world, including in Asia and Japan.1–3 However, there is no clear evidence of the role of childhood obesity in the development of adult obesity, and whether the age of onset of obesity in children is related to development of cardiovascular disease (CVD) in later life.4–7 Adult obese patients tended to have low birth weight, with a lower-than-average BMI up to 2 years of age, with a subsequent sharp increase in body weight before 11 years of age; the authors cited this growth pattern as a risk factor. 7 In addition, the risk of obesity in children progressing to adult obesity increases with age at onset, especially after 10 years of age. 4 Thus, in our previous study, we focused on the 3-year period between the ages of 9–10 and 12–13 years as representing the greatest risk group for progression to adult obesity and investigated changes in BMI, leptin, and adiponectin. The results demonstrated that those children with an increase in BMI over this period were also found to have decreased adiponectin and increased leptin values. 8 Furthermore, adiponectin was shown to be the strongest predictive variable for carotid intima media thickness in children with a mean age of 13 years. 9
Adiponectin is mainly classified into high–molecular weight adiponectin (HAD), hexameric medium–molecular weight adiponectin (MAD), and trimeric low–molecular weight adiponectin (LAD).10–12 While biological activities among these three isoforms are a matter of controversy, previous studies have indicated that HAD, MAD, and LAD have different biological activities. A number of clinical findings were reported on HAD, indicating that HAD levels, rather than the total adiponectin (TAD) levels, are better for predicting the development of insulin resistance, metabolic syndrome, and coronary artery disease.10,13,14
We have previously published three articles regarding adiponectin in children. The adiponectin composition varies markedly depending on whether the TAD value is high or low in children. 15 HAD was a strong predictor of abdominal obesity. 16 Monitoring waist-to-height ratio was a surrogate marker for HAD among elementary school students, especially in obese children. 17
However, there were no reports till this study had examined the changes in HAD, MAD, and LAD in the general population using a prospective cohort.
In this study, we focused on the 3-year period corresponding to the ages during which the onset of obesity is most likely to lead to either adult obesity or CVD.4,7 The objective of this study is to examine changes in the composition of differing adiponectin fractions, as well as their relationship between the changes in BMI, using a population-based, pediatric, prospective cohort over a 3-year period.
Methods
This study was conducted as part of a pediatric health promotion program8,15–19 initiated in 1994 in Ina-town, Saitama Prefecture, Japan. Ina is ∼30 km to the north of Tokyo with a population of 35,000 comprising both farmers and residents who commute to work in Tokyo. In addition to annual national health examinations performed in accordance with the School Health Law, Ina has a unique health-promotion program in place. Of the fourth and seventh graders who had undergone regular health examinations, those who volunteered to take part in the program underwent blood and physical examinations.
A total of 358 fourth graders (9–10 years old) from a town in Saitama Prefecture with a population of about 35,000 participating in community-based health examination programs in the fiscal year 2005 were followed up until they became seventh graders (first graders at junior high schools). Weight measurements included clothing, and height was measured with the subjects not wearing shoes.
BMI, TAD, HAD, MAD, and LAD were measured in these subjects at baseline (BMI 1, TAD 1, HAD 1, MAD 1, and LAD 1) as well as at the end of follow-up (BMI 2, TAD 2, HAD 2, MAD 2, and LAD 2).
Blood samples were drawn from the subjects at the time of their health examinations to measure their adiponectin isoform values using a commercially available ELISA kit (Daiichi Pure Chemical Co. Ltd., Tokyo, Japan). Intra-assay coefficients of variations for TAD, HAD+MAD, and HAD were reported to be 5.3%, 4.1%, and 3.3%, respectively.11,12 Most children had their blood sampled between 2 and 3 hours after eating breakfast as recommended by the institutional review board.
All values were expressed as median and interquartile range. The Wilcoxon signed-rank test was used to evaluate statistical significance.
The correlations in TAD, HAD, MAD, and LAD between their values at ages 9–10 years and their values measured at ages 12–13 years were assessed by using Spearman's correlation coefficient. The correlation of the ratios of follow-up compared to baseline values for TAD, HAD, MAD, and LAD to that of BMI values was plotted.
Also, the correlation of the ratios of follow-up compared to baseline values for TAD (TAD 2/TAD 1), HAD (HAD 2/HAD 1), MAD (MAD 2/MAD 1), and LAD (LAD 2/LAD 1) to that of BMI (BMI 2/BMI 1) values was plotted to demonstrate how these ratios were affected by changes in BMI value. Statistical analyses were made using SPSS program version 22.
The study protocol was approved by two independent Institutional Review Boards at Jikei University School of Medicine and Showa University School of Medicine. Written informed consent was obtained from all study participants and their guardians.
Results
Follow-Up Rates
Of the 358 (186 boys and 172 girls) children, follow-up physical and laboratory examination was performed on 326 (172 boys and 154 girls) subjects 3 years later (follow-up rate, 91.1%). Relocation was the major reason that children were lost to follow-up. There was no statistical difference in baseline values for sex and BMI between those subjects available for follow-up and those lost to follow-up.
Values Measured at Ages 9–10 Years and at Ages 12–13 Years
BMI was significantly increased over the 3 years in both boys (p < 0.001) and girls (p < 0.001).
No significant changes were observed in TAD values after 3 years in both boys and girls. HAD values were significantly decreased in both boys (p < 0.001) and girls (p = 0.005) from a median of 2.4 (1.8–3.5) μg/mL at baseline to a median of 2.2 (1.4–3.2) μg/mL after 3 years in boys, and from a median of 3.1 (2.0–4.1) μg/mL at baseline to a median of 2.7 (1.8–4.2) μg/mL after 3 years in girls. A significant increase in MAD values was observed only in boys (p = 0.048), but not in girls (p = 0.132). In contrast, LAD values were significantly increased in both boys (p < 0.001) and girls (p < 0.001) with the LAD values being a median of 1.3 (1.1–1.6) μg/mL at baseline to a median of 1.7 (1.5–2.0) μg/mL after 3 years in boys and a median of 1.4 (1.1–1.8) μg/mL at baseline to a median of 1.7 (1.5–2.0) μg/mL after 3 years in girls (Table 1).
The Median (Interquartile Range) for BMI, and Total Adiponectin, High–Molecular Weight Adiponectin, Medium–Molecular Weight Adiponectin, and Low–Molecular Weight Adiponectin in the Study Participants at Ages 9–10 and 12–13 by Gender
HAD, high
Wilcoxon signed-rank test.
Correlation Analysis
All values in the parameters examined at baseline and after 3 years were statistically significantly correlated (correlation coefficient: TAD, r = 0.715 for boys and r = 0.835 for girls; HAD, r = 0.739 for boys and r = 0.795 for girls; MAD, r = 0.505 for boys and r = 0.580 for girls; and LAD, r = 0.291 for boys and r = 0.252 for girls). With decreasing adiponectin molecular weight, the correlation became less robust in both boys and girls (Fig. 1).
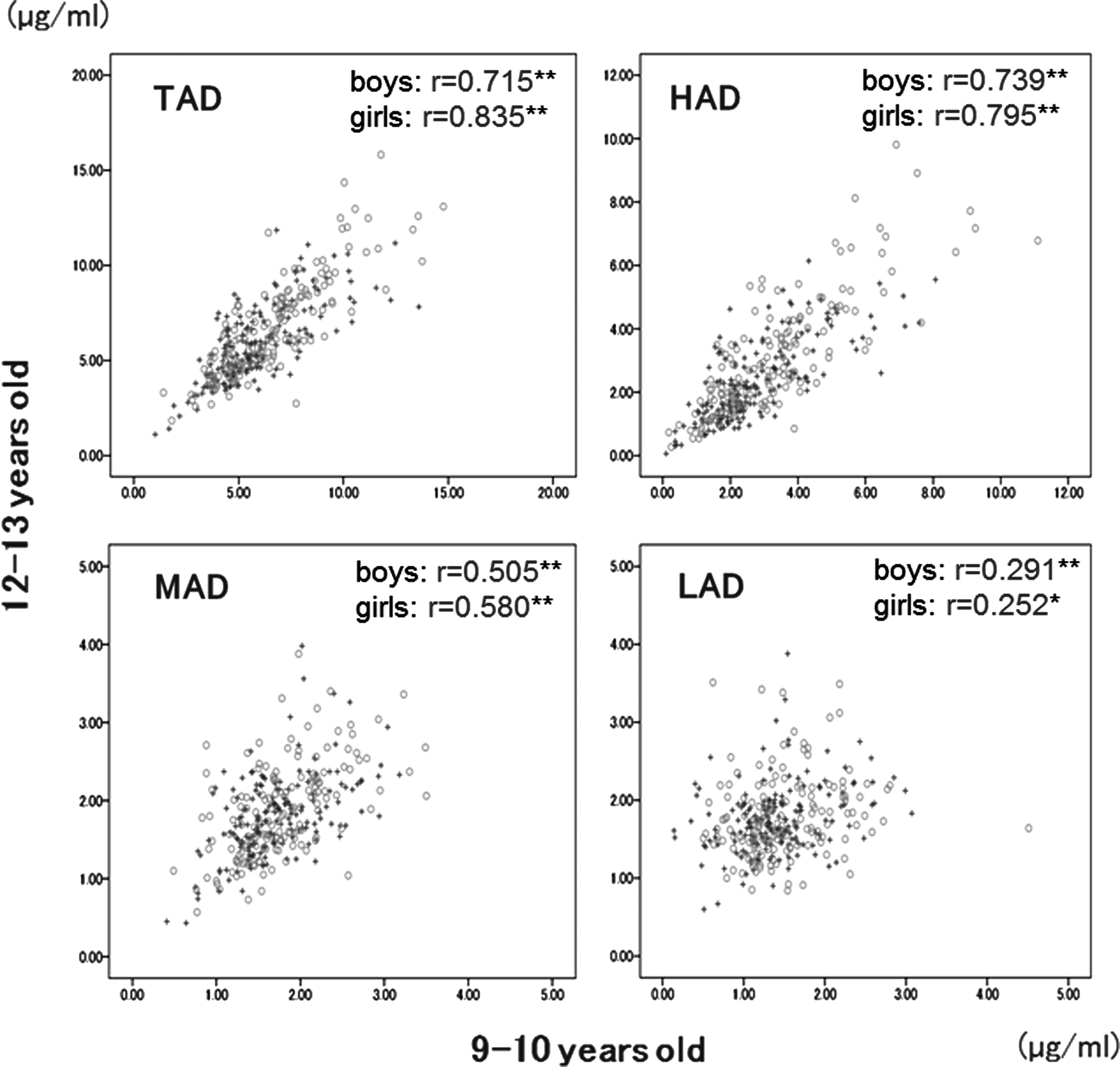
Correlation in TAD, HAD, MAD, and LAD between their values at ages 9–10 and their values measured at 12–13 by gender. Boys (+): n = 172; girls (○): n = 154. r: Spearman's rank correlation coefficients. **p < 0.001; *p < 0.01. HAD, high–molecular weight adiponectin; LAD, low–molecular weight adiponectin; MAD, medium–molecular weight adiponectin; TAD, total adiponectin.
A significant negative correlation was found between the ratios of follow-up to baseline BMI and those for TAD (boys, r = −0.322, p < 0.001; girls, r = −0.433, p < 0.001) as well as those for HAD (boys, r = −0.353, p < 0.001; girls, r = −0.351, p < 0.001) in both boys and girls. A significant negative correlation was found for the ratios of follow-up to baseline BMI and those for MAD only in girls (r = −0.277, p < 0.01) and those for LAD only in boys (r = −0.171, p < 0.01) (Fig. 2).

Ratios of the values for BMI (BMI 2/BMI 1), and total adiponectin (TAD 2/TAD 1), high–molecular weight adiponectin (HAD 2/HAD 1), medium–molecular weight adiponectin (MAD 2/MAD 1), and low–molecular weight adiponectin (LAD 2/LAD 1) measured at ages 9–10 (BMI 1, TAD 1, HAD 1, MAD 1, LAD 1) to those measured at 12–13 (BMI 2, TAD 2, HAD 2, MAD 2, LAD 2), and their correlation by gender. Boys (+): n = 172; girls (○): n = 154. r: Spearman's correlation coefficients. **p < 0.001; *p < 0.01.
Discussion
In this study, we focused on the 3-year period between the ages of 9–10 years and 12–13 years, reported to be the high-risk group for developing adult obesity,4–7,20–22 and investigated changes in adiponectin fractions and BMI.
This study targeted children living in an archetypal Japanese town with little population outflow, and followed changes in adiponectin fractions in a childhood population-based cohort over a 3-year period. The study results demonstrated that adiponectin fractions measured at baseline (9–10 years) correlated with those measured 3 years later. Therefore, these variables measured at ages 9–10 years were predictive for results obtained 3 years later.
The results of this study have demonstrated that the values of adiponectin fractions measured at ages 12–13 years were lower than those measured at ages 9–10 years. Adiponectin values in postpubertal children are reported to be lower than those in prepubertal children, especially in boys, which is explained by the elevated serum androgen levels in boys.23,24 Other reports in infants show that the adiponectin value drops in a 2-year-old to a greater extent than it does in a 1-year-old 25 or than in those less than a year old. 26 The report in adults indicates that adiponectin values do not change in women aged 18–80 years. 27 Mantzoros et al. reported that cord blood adiponectin levels were associated with birth weight for gestational age, inversely associated with weight gain in the first 6 months of life, and can predict an increase in central adiposity at age 3 years. 28
An examination of changes in the composition of adiponectin fractions over the 3 years in school children demonstrated that HAD had the most robust correlation between its values at baseline and after 3 years, with the HAD values being significantly decreased in both boys and girls; in contrast, LAD had the weakest correlation between its values at baseline and after 3 years, with the LAD values being significantly increased from baseline in both boys and girls. The changes in HAD also had the more robust correlation between the changes in BMI in 3 years than did other adiponectin fractions.
Limitations of this study include the lack of information regarding pubertal stage (Tanner's stages) of the studied children,23,24 which may act as a confounder for the data obtained. This study examined the relationship between the changes in adiponectin fraction and BMI, and did not take the children's lifestyles into consideration.
Recently, several reports regarding controversial aspects of adiponectin were published.
Higher serum adiponectin concentration was reported to be associated with increased all-cause and cardiovascular mortality in a community-dwelling elderly Asian population. 29 Adiponectin has been indicated as a cytokine with protective properties; however, the findings were surrounded by several controversies.30,31
Furthermore, several reports explored the relationship between adiponectin and skeletal muscle. It was shown that adiponectin is not only exclusively released from adipocytes but is also produced and released by skeletal muscle.32,33 One report's focus on muscular fitness in adolescents is of special interest. Muscular fitness is a determinant of adiponectin levels, in addition to overweight status, in adolescents. 34
Based on the previously mentioned, recent findings, further study is necessary to properly interpret the results of the current study. Especially, a long-term follow-up study should be conducted to determine the relationship between changes in adiponectin level and the onset of noncommunicable disease and CVD, and the relationship between the changes of adiponectin level and skeletal muscle or muscular fitness. These studies will be quite important in evaluating adiponectin as an important predictor of relevant clinical outcome.
In a population-based childhood cohort, baseline adiponectin, especially HAD, had the most robust correlation between its values at ages 9–10 years and those after 3 years in both boys and girls. The changes in HAD also had the most robust correlation with the changes in BMI over 3 years. Further in-depth research is required to clarify what implications these findings may have for the onset of noncommunicable diseases in later years.
Footnotes
Acknowledgments
The authors thank all study participants, their parents and guardians, all members of the Board of Education in Ina Town, Saitama Prefecture, and the Ina-machi Conference for the Promotion and Implementation of the Childhood Lifestyle-Related Disease Prevention Examination (Chairman: Dr. Yoshihito Toriyama). This study was supported, in part, by Grants-in-Aid from the Ministry of Education, Culture, Sports, Science and Technology of Japan (2002–2004, No. 14207020; 2005–2008, No.17209024; and 2013–2015, No.25350854). The Ministry of Education, Culture, Sports, Science and Technology, Japan, had no direct input into the design or conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript.
Author Disclosure Statement
R.N. has received research support from the Japan Diabetes Foundation, has participated in speaker's bureau/advisory panels for Astellas, Astra Zeneca, Boehringer Ingelheim, Daiichi-Sankyo, Eli Lilly, Johnson & Johnson, Kissei, Kowa, Medtronic, Novo Nordisk, Ono, Sanofi, Taishyo, Takeda and Tanabe-Mitsubishi, and served as a consultant for Abbott, Boehringer Ingelheim, Eli Lilly, and Taisho. N.T. has served as a speaker for MSD, Takeda Pharmaceutical Company, Eli Lilly Japan, Nippon Boehringer Ingelheim, Novartis Pharma, and Novo Nordisk Pharma. K.U. has received research support from Kowa, Ono, and Taishyo, and has participated in speaker's bureau/advisory panels for Astellas, Astra Zeneca, and Sanofi. All the other authors have no conflict of interest to declare.