
Abstract
Abstract
The growing prevalence of childhood obesity has become a serious health problem over the past decades. As the immune system is greatly affected by excess weight, in this review of reviews, we discuss the findings of review articles about the relationship between childhood/maternal obesity and children's immune system. We searched English-language articles in PubMed, Scopus, ISI Thomson Reuters, and Google Scholar databases. All relevant reviews, either systematic or narrative, were retrieved. Then their quality was assessed by using the Assessment of Multiple Systematic Reviews and International Narrative Systematic Assessment tools, respectively. In the final step, 26 reviews were included. Our review suggests that childhood obesity is associated with extensive changes in the serum levels of inflammatory and anti-inflammatory cytokines and proteins, as well as the number of immune cells and their behavior. Therefore, it might cause or exacerbate diseases such as asthma, allergy, atopic dermatitis (AD), and obstructive sleep apnea syndrome. Moreover, childhood obesity may reduce the immune system responsiveness to vaccines and microorganisms. Furthermore, studies suggest that maternal obesity increases the risk of asthma in offspring. Future studies are needed to determine different associations of childhood obesity with allergy, atophic dermatitis, and autoimmune diseases.
Introduction
According to the World Health Organization's definition, obesity is abnormal or excessive fat accumulation that presents a risk to health.1,2 The prevalence of childhood obesity has steadily increased since the 1980s 3 and now it is a serious and emerging public health problem, notably because of increasing risk of chronic noncommunicable diseases.4,5
Obesity is characterized by a low-level systemic inflammation, which also manifests within metabolic tissues, including adipose tissue and liver. This might lead to activation and infiltration of proinflammatory immune cells and dysregulated production of high levels of proinflammatory cytokines,6,7 causing differences in the immune response between obese and nonobese individuals. 8 Excessive fat accumulation might lead to substantial changes in the amount and function of immune cells, with an increase in the number and activity of some of them, for example, most notably macrophages, mast cells, neutrophils, and T and B lymphocytes. However, it might simultaneously reduce other immune cells, including eosinophils and several subsets of T lymphocytes, for example, T helper 2 (Th2), regulatory T cells (Treg), and inducible natural killer T cells. 9 The imbalance, caused by the mentioned changes in the immune cells, contributes to the development of obesity-related local and systemic inflammation. 1 The systemic proinflammatory profile in obesity has deleterious effects on the immune system, which is linked to the impaired immune responses, affecting both the innate and adaptive immune responses in obese individuals.10,11
Several reviews have been conducted regarding the association of childhood obesity with different aspects of the immune system or immune-mediated diseases. Moreover, some previous reviews did not assess the relationship between obesity/overweight and the immune system in the pediatric age group; therefore, we considered this topic in the current review. The quality of existing reviews varies; most of them cover a narrow part of the relationship between childhood obesity and immune system and some of them provided conflicting results.
The current systematic review of reviews aims to summarize the findings of the high-quality reviews concerning the association of childhood overweight/obesity with the immune system. It also aims to discuss the disorders that can be caused, mediated, or worsened by the changes in the immune system of obese children.
Methods
This article presents a systematic review of reviews on the relationship between maternal and childhood obesity and the immune system and immunological factors.
Review Questions
This review attempts to answer the following questions:
• How does childhood obesity or maternal obesity affect the immune system and the immune-mediated diseases, for example, asthma and allergy? How does it influence the functions of immune system? • How does childhood obesity affect the immune system protein products, for example, cytokines, and how changes of cytokines might affect different organs or different cells in the body? • How does childhood obesity affect the immune cells? • How does obesity-induced inflammation or other problems caused by obesity change the physiological state in the children's body to pathological state?
Search Strategy
We performed a systematic search in the following electronic databases: PubMed, ISI Thomson Reuters Web of Science, Scopus, and Google Scholar. The literature search was conducted in October to December 2015.
For searching the electronic databases, the following strategies were used:
First, we identified relevant review articles reporting association between the immunological factors (e.g., the immune cell products such as cytokines, immunological diseases, and different type of immune cells) and childhood obesity by using related terms. For PubMed search, we considered Medical subheading words, and for other databases, we used keywords. Box 1 shows the terms we used in PubMed search. For other databases, some of the terms in the PubMed were amended. We restricted our search only to the English articles, but we did not set any time restrictions. For finding more relevant articles, we screened titles, abstracts, and keywords in PubMed, Scopus, and ISI Thomson Reuters. Second, we imported related articles on the subject of the Thomson Reuters Endnote 7.1 and removed any duplicates. Third, the reference lists of review articles were controlled and the relevant articles were retrieved. Finally, two independent reviewers (M.R. and S.S.) reviewed the retrieved articles for relevance, assessed the quality, and extracted the data that are described in the following paragraphs in detail.
Search String Used (for MeSH Terms and Keywords in the Abstract and Title)
Relevance (Inclusion/Exclusion)
Included articles had the following criteria: (i) reporting a review article (systematic, narrative, or meta-analysis) and (ii) presenting the relationship between childhood obesity/overweight and immunological factors.
Articles were excluded if they contained keywords about obesity or immune system, but did not relate any of immunological factors to childhood obesity.
For making the inclusion/exclusion more accurate, we developed a relevance criterion and used it for all of the retrieved articles. This relevance tool was, based on that used in the Effective Public Health Practice Project (EPHPP) 12 and amended to become useful for this study.
Quality Assessment
For quality assessment, articles were categorized into two groups:
(1) Systematic and meta-analysis reviews: We assessed the review articles, in which the authors stated that their articles are systematic review, by using the Assessment of Multiple Systematic Reviews (AMSTAR) tool. This tool, which is used for quality assessment of systematic reviews, is a validated 11-item tool based on factors such as an “a priori design,” comprehensiveness of literature search, and the inclusion and exclusion criteria. Each item is awarded one point if it met the criterion, and is given zero if it was not met, not applicable, or it was not possible to answer the question. In the AMSTAR, scores of 0–4 indicate low quality, 5–8 indicate mediate quality, and 9–11 indicate high quality. In this study, systematic articles and meta-analysis of mediate or high quality were studied. (2) Narrative reviews: For quality assessment of narrative articles, a new validated tool, named the International Narrative Systematic Assessment (INSA) tool, was used. INSA is a seven-criterion tool developed to assess the quality of narrative articles.
13
It is designed mostly based on AMSTAR
14
and Overview Quality Assessment Questionnaire
15
with adding some new questions for quality assessment of narrative reviews. Like AMSTAR tool, each item is awarded one point if it met the criterion, and is given zero if it was not met. Quality of narrative reviews is considered good if awarded at least five points.
Two reviewers assessed the quality of relevant articles. In the case of disagreement, a third reviewer was involved and discussion took place until consensus was achieved.
Data Extraction
Data were extracted from the strong narrative reviews (based on the INSA tool) and moderate or strong systematic reviews or meta-analysis (based on the AMSTAR tool). The main objectives of some studies were not concerning the relationship between obesity or overweight and the immune system/disease in the infants, children, adolescents, but the important data about this subject were included in this review.
A standardized data extraction form was developed to obtain required information from the eligible articles and was as follows: (i) general characteristics of the study (first author's name, publication year, type of review, and type of articles included); (ii) definition of the childhood obesity (if declared); (iii) main findings about the relationship between childhood obesity and the immune system; (iv) the probable mechanisms involved; and (v) recommendations made by authors. These data are provided in different tables and through paragraphs in the Results section.
Two reviewers extracted and then compared the data while another checked their extracted data. In disagreements, reviewers discussed until consensus on all data was achieved. As this review of reviews includes both systematic and narrative reviews, this article did not try to pool the results.
Results
Description of Included Reviews
Figure 1 shows the study flow diagram in detail. Quality assessment was done for 59 articles. All of the 24 included articles were conducted between 2006 and 2015. Among them, 17 articles were narrative articles and 7 articles were systematic reviews and meta-analysis. Based on the AMSTAR tool for the systematic reviews and meta-analysis, 2 articles were considered as weak, 6 as moderate qualities, and 1 as strong and, based on the INSA tool, 31 narrative articles were considered as weak and 17 articles were strong. The average score of all relevant systematic and meta-analysis articles (included and excluded studies) assessed by AMSTAR was 6.44; the average score of all narrative articles assessed by INSA was 3.875. All the included articles were classified as moderate or high score. The results were categorized into five main groups to organize the context: a category about cytokines and other protein products, including 6 articles; a category about the role and changes of the immune cells, containing 1 article; a category about diseases caused by immune system caused by obesity, containing 12 articles; a category about the impact of obesity on immunity and response of the immune system to vaccines, containing 2 articles; and finally a category about the relationship between maternal obesity and the offspring's immune function, containing 3 articles. Among 12 studies on diseases, 10 reviews were about the childhood obesity–asthma relationship, 1 about allergy and obesity in children, and 1 of them was about atopic dermatitis (AD). Among seven included systematic articles and meta-analysis, five of them were about the childhood obesity–asthma relationship, one article about maternal obesity and childhood asthma, and one about atherosclerosis and inflammation markers in obese and nonobese children. For other categories, no high-quality systematic reviews was found, based on our search methods, relevance criteria, and quality assessment by the AMSTAR tool.
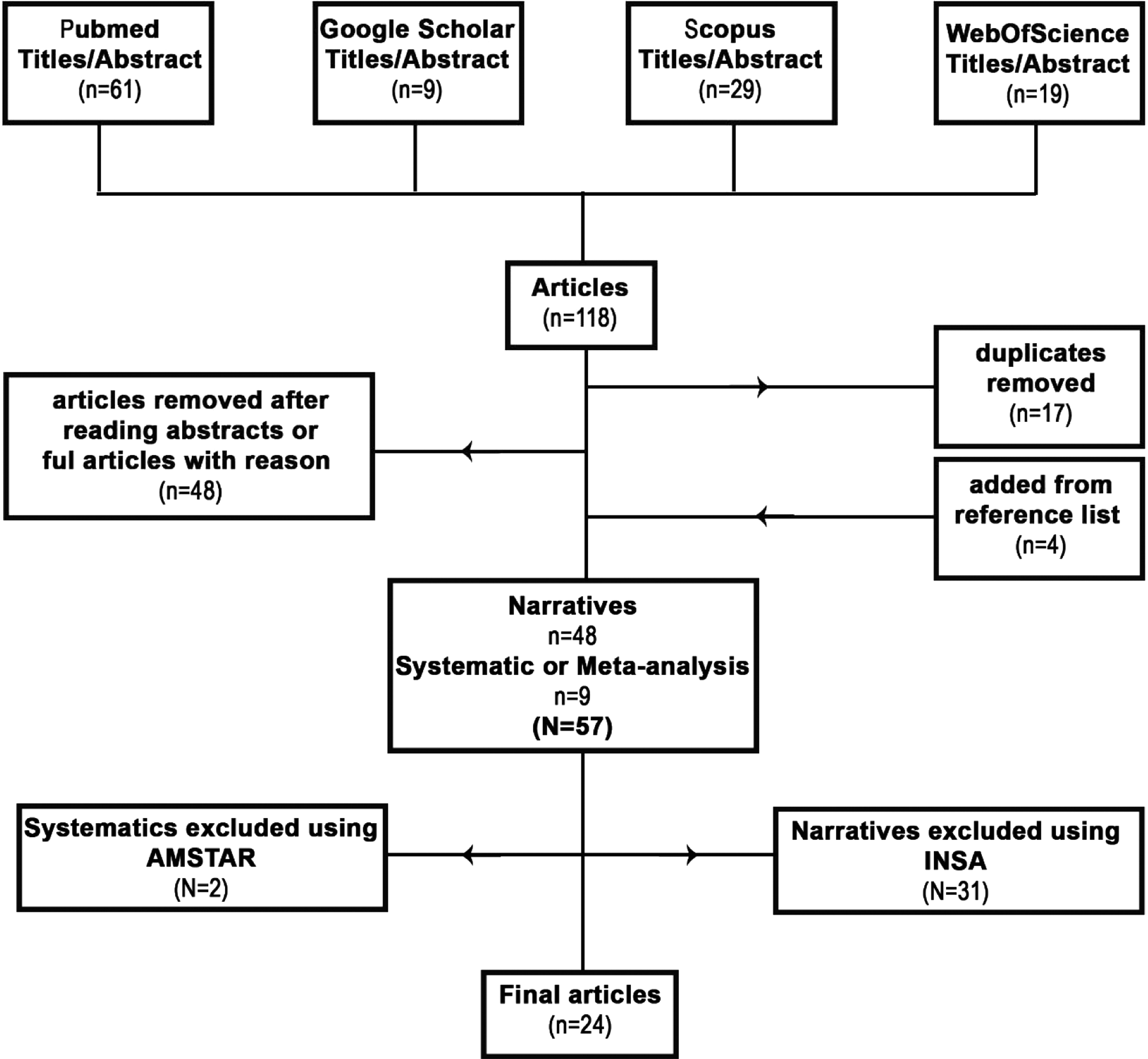
Diagram of study selection.
Definition of Childhood Obesity/Overweight
There is a difference in the definition of childhood obesity across different studies. The definition of childhood obesity or overweight is mostly based on the children's BMI. However, most of the mentioned included studies express a low-grade inflammation status as an important characteristics of the childhood obesity, which might be induced by release of different cytokines and adipokines. 16 Table 1 shows important characteristics of included systematic reviews. Table 2 shows the findings according to the definitions of childhood obesity, based on the child's BMI.
Characteristics of Included Systematic Reviews
Summaries of Included Articles
AD, atopic dermatitis; CRP, C-reactive protein; GDM, gestational diabetes mellitus; IMT, intima-media thickness; TNF-α, tumor necrosis factor-α; WAT, white adipose tissue.
Childhood obesity, biomarkers, and adipokines
Considering the important role of cytokines and other factors affecting the immune system, as well as the products of adipose tissue on different aspects of immunity and immune-mediated diseases, a summary based on high-quality narrative reviews is also included in this study. It is presented in the following paragraphs, which may help readers in studying other categories. A review on hormones and cytokines in obesity introduced different biomarkers taking part in the pathogenesis of obesity and inflammation. 3 To have a comprehensive view on the importance of cytokines in obesity, we provided a summary including supporting data from included review articles.
Adipose tissue produces some cytokine mediators, such as interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and adiponectin, but some of the mediators are not produced in adipose tissue; however, their concentrations are under the control of adipokines, such as C-reactive protein (CRP) and interleukin-10 (IL-10).
Leptin
Leptin is a protein containing 166 amino acids. It is mostly produced in the adipose tissue and only small amounts are synthesized in other human tissues. It affects different organs and various systems, including the immune system and bone formation by leptin receptor, also it has an important role in the energy balance. Studies included in “hormones and cytokines in childhood obesity” have shown elevated leptin levels in obese children along with decreased leptin levels during the weight-loss period. A review study focusing on the role of leptin on the mucosal immunity found that leptin is a critical immunomodulator in both humans and murine models. Leptin levels are changed because of genetics and nutritional statuses. Obesity increases leptin levels, whereas malnutrition reduces its levels. As both kinds of these weight disorders increase the susceptibility to infections, it is suggested that leptin levels are associated with alterations of the immune system. 17 Leptin is greatly associated with the cardiovascular risks and metabolic syndrome. 3 As another review suggested, leptin increases the secretion of proinflammatory cytokines such as TNF-α, IL-6, and IL-1 by macrophages. In addition, it promotes macrophages phagocytosis, suppresses the generation and proliferation capacity of Tregs, accordingly making individuals more susceptible to the autoimmune diseases. 18
Adiponectin
Adiponectin is a highly expressed protein in the adipose tissue. Two adiponectin receptors are cloned, adipoR1 in the skeletal muscle and adipoR2 in the liver. Adiponectin is clinically considered important because of its insulin-sensitizing, anti-inflammatory, and antiatherogenic properties. Studies have shown that adiponectin serum levels decrease in obese people, whereas weight loss increases. 3 In a review by Tam et al., three studies out of six demonstrated a direct correlation between the weight loss or fat mass reduction and an increase in the adiponectin serum levels, but three of them found no relationship between the lifestyle change and adiponectin serum levels; however, the authors concluded that there is enough evidence to support the reduction of adiponectin in obesity. 19
Tumor necrosis factor-α
TNF-α is a proinflammatory cytokine. Macrophages and T lymphocytes are its main producers, and it is also produced in the adipose tissue in less quantities. Studies have shown an increase in the serum levels of TNF-α in the obese compared with the nonobese people. The main reason for this increase is probably because of the systemic effects of leptin or other adipokines on macrophages and lymphocytes, causing elevation of TNF-α levels. TNF-α has two clinically important effects on obese children, adolescents, and adults: insulin resistance and endothelial inflammatory changes, the latter changes the vascular tissue, causing tissue dysfunction and hypertension. 3
Interleukin-6
IL-6 is a cytokine, functions in inflammation, immune response, and tissue injury processes. Many cell types and tissues produce IL-6, such as the immune cells and the adipose tissue. Studies have shown increased IL-6 production by the adipose tissue in obese people. Enhancement of IL-6 in obesity causes insulin resistance and increases risk for cardiovascular complications, and predicts type 2 diabetes and future myocardial infarction. 16 It also affects some other proteins playing an important role in obesity and inflammation, such as reducing adiponectin secretion and increasing CRP production in the liver. 3
Interleukin-10
IL-10 is an immunosuppressive cytokine, which is produced by the activated macrophages and Th2 lymphocytes. Obesity decreases the serum levels of IL-10, which is considered a risk factor for insulin resistance, atherosclerotic plaque instability, and acute coronary ischemia. IL-10 antagonizes TNF-α and IL-6, causing them to have insulin-sensitizing, anti-inflammatory, and endothelial protective properties. 3
C-reactive protein
CRP is an acute phase plasma protein mainly produced by hepatocytes. Inflammatory processes increase CRP plasma levels, and obesity, which causes a low-grade inflammation, causes higher concentrations of CRP. The data extracted from different studies confirm strong relationship between CRP and obesity, and also between CRP and BMI. It is suggested that an increase in the serum levels of CRP imposes inflammatory effect on obesity. 20 The association of CRP with type 2 diabetes is documented. 16 A review showed that CRP levels are higher in the children and adolescents having higher values of waist circumference. 21 Another review found reasonable evidence about the association of obesity with increased CRP. It also suggested that weight loss of at least 5% significantly improves the levels of inflammatory mediators such as CRP in the children. 19
Other adipokines
Adipokines impress different systems, including the immune system. A review by Barraco et al. focused on most recently identified adipokines: adipocyte–fatty acid–binding protein, chemerin, fibroblast growth factor-21, lipocalin-2, omentin-1, and vaspin. The review summarized the results of 17 studies about these recently identified adipokines; however, because of the small sample size of most of the studies and the lack of enough confirming articles in this area, larger cohort and randomized clinical studies are needed to understand the molecular mechanisms of adipokines deeply. 22
A review including 12 studies (mean age range in studies between 7.87 and 17 years) on the effects of lifestyle interventions on the levels of circulating inflammatory mediators in children suggested that the different levels may be because of differences of gender, pubertal status, and sensitivity of the assays. 19 The authors concluded that longitudinal studies examining inflammatory-related molecules in obese children are needed to examine the persistence of increased levels of markers of inflammation over childhood.
Obesity and immune cells in childhood
Only one of the included reviews summarized the role of immune cells in the obesity–immunity relationship; however, it did not specifically study this subject, but reviewed the obesity–immunity relationship and the role of nutrition, generally. This review suggested that a considerable change in the immune cells, their distribution, and products happens in obesity, causing inflammation. Important and documented results of this review are presented hereunder.
Macrophages
A total of 40%–60% of the visceral adipose tissue (VAT) immune cells are macrophages. The review discusses two different macrophages: in the lean VAT, M2 macrophages secrete factors such as arginase 1. Therefore, it exerts anti-inflammatory activities, but in obesity, obesity-associated macrophages, known as M1 macrophages, are activated. These macrophages secrete large amounts of TNF-α, IL-1β, IL-6, IL-12, and monocyte chemotactic protein-1, which seem to cause insulin resistance.
Lymphocytes
Tregs decrease in both obese mice and obese humans, but T helper 17 cells (Th17 cells) increase in both, leading to more IL-17 production and release. The review suggests the imbalance between these two cell types to maintain the inflammation in obesity. The evidence shows an association between the autoimmune diseases and Th17 cells through some mechanisms. Studies in obese mice have shown higher number of CD4+ T helper cells, CD8+ cytotoxic T cells, and B cells in the VAT. B cells infiltration into the VAT provokes insulin resistance through some mechanisms.
Other immune cells
Neutrophils and mast cells contribute to inflammation, whereas the number of eosinophils is decreased in obese mice. 16
Obesity, the immune system, and diseases in children
The relationship between overweight/obesity and asthma in children
The aim of writing this category is to take a deeper look at the effect of obesity on asthma in children, statistically by reviewing some of the high-quality reviews. It is provided by evaluating and mentioning the role of the immune system, cytokines, and inflammation and inflammatory processes as involving factors, which mitigate or worsen asthmatic symptoms in overweight/obese children. The following systematic reviews mostly dealt with the prevalence of asthma and the risk of asthmatic symptoms development, presented an epidemiological view of the relationship, and evaluated the role of different factors such as age and gender, whereas the narrative reviews in this category were concerning mostly on mechanisms involved in the relationship between overweight/obesity and asthma in children.
A meta-analysis on the effect of weight status on future asthma found that excess weight among children would increase the risk of future asthma. The combined results of four and nine studies provided a relative risk of 1.5 (95% confidence interval [CI] 1.2–1.8) and 1.2 (95% CI 1.1–1.3) for future asthma in school-aged children and those with high birth weight, respectively. It mentioned that sources of bias in the meta-analysis were because of misclassification of exposure, especially because of the difference in definition of high body weight, variety of ages, and different BMI centiles in various cohorts. However, levels of homogeneity showed that the association of obesity with high birth weight was not because of misclassification exposure. This meta-analysis concluded that risk factors such as family history, air pollution, and atopia have more important roles on asthma than on weight. 23
A systematic review included 35 studies: 27 of these reported positive association of obesity/overweight with asthmatic syndrome in the pediatric population of 0–18 years. 24 One of the studies included in this review found that overweight or obese children are 1.16–6.8 times more likely to develop new asthmatic symptoms than their normal weight counterparts. It found that gender was the most important recognized effect modifier. Twelve studies reported the effect of gender on the relationship between asthma or asthmatic symptoms and obesity, and more than half of them showed a stronger association between BMI and asthma in girls than in boys.
Another systematic review that included six cohort studies on children younger than 18 years found that the combined risk ratio of obesity was associated with asthma in both genders (RR = 1.50; 95% CI = 1.22, 1.83), in boys only (RR = 1.40; 95% CI = 1.01, 1.93), and in girls only (RR = 1.53; 95% CI = 1.09, 2.14). 25 According to the authors' view, gender effects were inconsistent and they identified no other effect modifiers except gender. Another systematic review found that the relative risk of elevated BMI on incidence of asthma is significantly larger among boys (relative risk: 2.47; 95% CI, 1.57–3.87) than among girls (relative risk: 1.25; 95% CI, 0.51–3.03).
A systematic review that included 10 longitudinal analyses found a positive association between overweight/obesity and asthma in 8 studies. 26 In this review, the role of gender in obesity–asthma relationship was controversial and vague, but it provided strong evidence on the association of obesity with the persistence and intensity of asthma symptoms.
Another systematic review and meta-analysis that included six studies found increased risk of asthma incidence in overweight children than in nonoverweight children in its combined results (relative risk: 1.19; 95% CI, 1.03–1.37) and elevated relationship for the obese compared with the nonobese children (relative risk: 2.02; 95% CI, 1.16–3.50). 27 The risk of incident asthma in obese children was significantly higher among obese boys than among obese girls (boys: relative risk: 2.47; 95% CI, 1.57–3.87; girls: 1.25; 95% CI, 0.51–3.03). Some of the suggested mechanisms to explain the obesity–asthma relationship by the authors were hormonal and inflammatory mediator changes, dyslipidemia, sleep disordered breathing, gastroesophageal reflux, and obesity-related reduction in the lung volume.
Two studies suggested that the differences in results for the role of gender may be because of various stages of sexual maturation, pulmonary mechanics, sleep disordered breathing, and the level of circulating leptin, as the age range of the study participants was not the same.26,27 Categorization of the obese asthmatic children, based on factors such as their age and sex, plays an important role in development of more accurate weight-loss strategies. 28
A review dealt with possible mechanisms of the association between obesity and asthma. The target age of this study was not restricted to children and it provided a general discussion about the matter. This review showed that the following factors play a role as possible mechanisms: mechanical factors such as reduction of functional residual capacity and tidal volume, low-grade systematic inflammation caused by obesity, changes in adipokines such as IL-6 and TNF-α, and changes in the adipose tissue-derived energy-regulating hormones such as leptin and adiponectin. It suggested that leptin, because of its proinflammatory effects, plays an important role in the relationship between obesity and asthma, mainly because of its remarkable increase in obesity, but adiponectin, which is known for its anti-inflammatory effects, in contrast with other adipokines, declines in obesity. 29
Another study that took a deeper look on the immune aspect in the asthmatic obese children suggested two pathogenetic mechanisms. First, by enhancement of vistatin and leptin serum levels, T helper 1 cytokines such as IL-2 and IFN- γ are increased and Th2 cytokines such as IL-4 and IL-13 are decreased. Second, because of decreased level of adiponectin, Tregs are reduced, causing more proinflammatory cytokines production, for example, IL-1β, IL-6, and IL-8. 16
A review that included 32 different studies, mostly cross-sectional and case–control, answered some important questions on the asthma–obesity relationship during childhood. It suggested nine major mechanistic explanations of the obesity–asthma relationship, including higher production of proinflammatory cytokines such as TNF-α, IL-6, and IL-1β. 30 A narrative review mentioned the convincing evidence of the role of macrophage and mast cell in obesity, but also stated their unclear mechanisms of contribution in the obesity–asthma pathogenesis. 28
A narrative review assessed some of the most important mediators measured in obese asthmatic children or adolescents in 24 cross-sectional and case–control studies, and suggested some mechanisms. 31 The age of studied children varied, but all were aged between 2 and 19 years. Of six studies, measuring leptin, three of them showed higher levels in obese than in nonobese children, two of them found higher levels of leptin in the healthy weight asthmatic children than in the healthy weight controls; only one study showed nonsignificant difference between the asthmatic patients and healthy controls. Of four studies on adiponectin, three studies showed lower levels of adiponectin in obese children than in nonobese or healthy weight children; only one cross-sectional study did not find any significant difference in the adiponectin level between the asthmatic children and healthy controls. Of seven studies on CRP, six of them showed higher serum levels of CRP in obese children than in nonobese children, only one study found no difference, which may be because of its small sample size. All four studies on the serum levels of IL-6 showed higher levels of IL-6 in obese children than in nonobese or healthy weight children, and all three studies on TNF-α showed higher levels of TNF-α in children with excess weight than in healthy controls. Given that the volume and number of adipocytes are increased in obese individuals, more proinflammatory mediators are released, providing a stimulus for chronic, low-grade systemic inflammation.
A study showed the attenuated efficacy of inhaled steroid medications in the asthmatic children because of their obesity; it suggested more investigation on the effects of excess weight on childhood asthma treatment. 32 Some of the mentioned data on different serum levels of cytokines are controversial. In addition, most of the performed studies in this category were of observational type. Thus, we need a review to emphasize on high-quality randomized controlled trials regarding weight loss in obese children and adolescents to assess the systemic and airway inflammation and clinical asthma outcomes. 31
Did the excluded reviews come to different conclusions than included reviews?
Although all excluded studies confirm the association between childhood obesity and asthma, they suggest different mechanisms responsible for this association and they differ in details. A review suggested that low-grade systemic and airway inflammation is not the only mechanism involved, but there is mounting evidence to support there are noninflammatory mechanisms involved in this association in obese asthma mouse models as well, but these data should be translated to humans. The importance of these data is that by finding noninflammatory and nonatopic mechanisms involved in the association, there is a need to change the treatment of obese asthmatics from inhaled corticosteroids to bronchodilators and/or anticholinergics. 33
As described previously, most of the included narrative reviews mentioned the importance of the role of adipokines in obese asthmatics, but a review concluded that adipokines play an important role in certain phenotypes of asthma, not all of them. 34
Another review suggested that the risk of asthma development is increased in obese children, but there is not enough evidence supporting that obesity increases the severity of asthma 35 ; however, a systematic review suggested that central obesity in children is associated with the incidence and severity of asthma. 36
Childhood obesity and allergy
A review included eight cross-sectional, case–control, and population-based studies evaluating the relationship between obesity and allergy. It concluded that the association of nonallergic asthma with obesity is stronger than the association of allergic asthma with obesity. The association of obesity with allergic diseases other than asthma is inconsistent, which is possibly modified by factors such as age, gender, and ethnicity. This association is more consistent in eczema, but some studies on the relationship between allergic rhinitis/rhinoconjunctivitis and obesity did not show any association, and some found inverse relationship. 37
Childhood obesity and AD
AD is a chronic, recurrent, pruritic inflammatory disorder of the skin. A review study expressed its multifactorial etiology and considered the role of childhood obesity in other atopic diseases, including atopy, asthma, and rhinoconjunctivitis. It introduced AD as a disease that can be caused or worsened by obesity, as data corroborate that obesity is a modifiable risk factor for AD; moreover, weight control and dietary interventions may alleviate its excess risk. Obesity may increase the risk for other types of dermatitis as well. 38
Childhood obesity on the immune response to infections and vaccines
As most vaccines are administered during childhood, the effect of childhood obesity on the response to vaccines is discussed. A review on the effect of obesity on the response to vaccination in humans has summarized nine studies: six of them studied the immune response to hepatitis B vaccine, one of them studied the immune response to tetanus, and two of them studied the immune response to influenza vaccine in obese people compared with that in controls. All of the studies on hepatitis B vaccine showed reduced immunogenicity, as HBsAg (hepatitis B virus surface antigen)-specific IgG response or low anti-HBs (hepatitis B surface antibody) levels were lower postvaccination in obese individuals than in their nonobese counterparts. One study on the immune response to tetanus vaccine in obese people showed lower antitetanus IgG antibodies, higher IL-6 levels, and no change in TNF-α, IL-1β, and IL-1α cytokine levels. The review also studied the relationship between obesity and reduced resistance to infections such as Mycobacterium tuberculosis, Coxsackie virus, Helicobacter pylori, and influenza. It suggested that the reduced resistance may be because of change in the number of lymphocytes and reduction of some cell types such as dendritic cells, which are professional antigen-presenting cells, reduced lymphocytes responsiveness to microbial stimulation, and alterations of cytokine levels because of obesity. 18
Another review also showed poor antibody response to hepatitis B vaccine in obese individuals and lower IgG antibodies in response to vaccination in obese children than in healthy weight children. 39 The review also emphasized on the higher susceptibility to H1N1 influenza virus through the 2009 pandemic. The study hypothesized that the immune response reduction in obese people may be because of generation and/or function of the antibody-secreting plasma cells and reduced adsorption at the site of injection because of excess adiposity.
The relationship between maternal obesity during pregnancy and offspring immunity
The outcome of our own review concerning the impact of maternal obesity during pregnancy on offspring immunity, abnormal growth, and neural tube defects is stated hereunder.
A review included 11 human and 3 animal studies that determined the impact of pregravid obesity on infants. 40 It showed that high-fat intake or increased maternal BMI might change the offspring's immune system in utero. The immune system is crucial in the pathogenesis of various diseases, including asthma, diabetes, and cardiovascular disease; therefore, the maternal obesity is associated with increased incidence of the mentioned diseases. The placenta has a key role in fetal growth and development, and also in the neonatal immune system because it transports nutrients to the fetus. The review hypothesized that the placenta blood flow is reduced in obese mothers because of lipid accumulation in the placenta, especially in the villi stroma. This might lead to hypoxia and to increase in placental inflammation, therefore, altering the nutrient transport to the fetus and causing health problems. Because of this change, levels of the fetal cytokines may be altered, resulting in different response to vaccination and allergens later in childhood or adulthood. Another suggested mechanism is that maternal obesity may impact the offspring's immune system by changing the gut microbiota. 41 Further studies are needed to understand the mechanisms of maternal obesity–offspring's immunity relationship. A better understanding of the subject may be helpful in treating diseases such as asthma, diabetes, and cardiovascular diseases.
In another review, changes in inflammatory mediators in the maternal and fetal/placental compartments in obese and gestational diabetes mellitus (GDM) were inconsistent (e.g., the serum levels of TNF-α in both the maternal and fetal/placental samples). 42 It suggested that the placenta mediates inflammation in obese and GDM, but data are insufficient to equate inflammation in the fetal serum and maternal inflammation. This review also recommended further researches to find inflammation mechanisms in pregnant women and in their offspring.
A systematic review assessed the effect of maternal obesity on pregnancy or increased maternal gestational weight gain. 43 Wheezing was categorized as ever, current, transient, or persistent, and asthma as ever or current types. The pooled analysis represented higher odds of asthma or ever wheeze in association with maternal obesity in pregnancy (OR = 1.31; 95% CI, 1.16–1.49) or current (OR = 1.21; 95% CI, 1.07–1.37) and an association was seen between the high gestational weight gain and increased odds of asthma or ever wheeze (OR = 1.16; 95% CI, 1.001–1.34). For each 1 kg/m2 increase in maternal BMI, the odds ratio of childhood asthma would increase by 2%–3%. The authors suggested some mechanisms for the relationship seen between maternal obesity and asthma in offspring: (1) Elevation of inflammatory cytokines such as TNF-α, IL-6, and transforming growth factor-beta-1. (2) Higher concentrations of leptin, which is a proinflammatory cytokine, in both pregnant obese women and their offspring than in nonobese pregnant women and their offspring. (3) Decreased adiponectin levels in obese and in newborns of obese mothers. They also suggested that in obese women, the serum levels of vitamin D3 have lower concentrations (normal range: 75–299 nmol/L), which is associated with increased risk of childhood asthma. Genetic polymorphism and changes caused by maternal obesity might cause or mediate the increased risk of asthma in their offspring.
Discussion
This systematic review of reviews aims to study the association of maternal and childhood overweight or obesity with the immune system function. The second objective is to study the effects of these factors on diseases that might be caused, mediated, or worsened by the changes in the immune system of the pediatric age group. The effect of maternal obesity on the fetal immune system has also been discussed, but few studies were supporting data on this matter.
Many cytokines, hormones, and adipose tissue products have been suggested to affect the immune system in both children and adults, but the role of leptin, adiponectin, TNF-α, CRP, IL-6, and IL-10 is more thoroughly discussed. As indicated by most studies included in this review, obesity is associated with increase in the serum levels of leptin, TNF-α, CRP, and IL-6. These factors are considered as risk factors for insulin resistance, metabolic syndrome, and cardiovascular problems, they also mediate diseases such as asthma, allergy, and other diseases already discussed; we did not include other immune-mediated diseases in this review. Obesity also leads to lower serum levels of adiponectin and IL-10, which are the protective factors in the mentioned diseases. Losing weight significantly reduces the inflammatory markers such as CRP and might increase protective factors including adiponectin. 20
One of the included reviews that presented some information on the immune cells in obese children showed considerable change in the immune cells, their distribution, and products caused by obesity, especially macrophages and different types of T lymphocytes such as CD8+ and Th17 cells. The imbalance of these cells may lead to inflammation and autoimmune diseases. Limited data exist on obesity-related change of immune cells and its consequences; therefore, more studies are needed in this area.
We found a well-documented relationship between childhood obesity and asthma, but gender differences were inconsistent in this regard. Our findings suggest that the immune system has a crucial role in the relationship between obesity and asthma in children. Through different ways, the immune system might trigger or exacerbate the asthma and asthmatic symptoms. Most studies included in this review had mainly focused on the role of inflammatory markers and adipose tissue protein products. Most studies revealed increased levels of some proinflammatory factors, including leptin, CRP, IL-6, and TNF-α in obese or overweight children. They also showed that some anti-inflammatory factors such as adiponectin are reduced in obese children. Therefore, we suggest that in obese children, asthmatic symptoms are aggravated because the low-grade chronic inflammation related to obesity is added to the inflammatory pathways of asthma. The immune system and inflammatory process are not the only factors worsening the asthmatic symptoms, the role of other variables including the mechanical factors should be considered as well. 29 The current evidence cannot prioritize which factors are more important in the obesity–asthma relationship, thus more studies are necessary in this regard. Further studies in this field might also provide more accurate weight-loss strategies. 31 Our findings propose that as several studies showed clear relationship between childhood obesity and asthma, it is necessary to implement interventional and randomized controlled trials on the effect of weight loss and clinical outcomes on asthma.
We found few articles on obesity and its consequences on immune-mediated diseases other than asthma. The association of obesity with allergic disorders is inconsistent 37 and warrants further research in this area. A review was written on the relationship between AD and obesity, 38 showing AD as a disease caused or exacerbated by obesity. Moreover, it suggested that weight loss and dietary interventions might alleviate the excess risk of AD. We found few articles on the relationship between childhood obesity and autoimmune diseases and we propose conducting research in this area as well.
The data from some included reviews showed positive relationship between obesity and the response of the immune system to infections and diseases.17,39 These reviews showed depressed immunogenicity to vaccines such as hepatitis B because of lower antibody titers in obese people and reduced resistance to diseases such as Mycobacterium tuberculosis and H1N1. However, these studies were not specifically done in the pediatric age group, and they were included because vaccination is done in children as well as in adults.
Three included articles,40,42,43 one systematic and two narrative articles, found the significant association of maternal obesity with infant's immunity or risk of asthma. It is suggested that the accumulation of lipid in placenta might lead to hypoxia and increased placental inflammation, causing health problems, such as change in level of cytokines in infants, which would result in different responses to vaccination and allergens later in childhood or adulthood. In our review, we found that for each 1 kg/m2 increase in maternal BMI, the odds of childhood asthma would increase by 2%–3%. These findings suggest that the higher serum levels of TNF-α, IL-6, and leptin of both pregnant obese women and their offspring might be one of the underlying factors for immune-related disorders such as asthma.
Our findings propose that obesity and overweight in infants and children might greatly affect the immune system by changing the immune cell responses and levels of cytokines. In turn, it may reduce the immune response to antigens or vaccines, or may alter the immunological response and inflammatory processes in a way that causes or worsens diseases or their symptoms, such as asthma and other related disorders. Our review confirms the importance of prevention and early control of childhood obesity for reducing the risk of immune-mediated disorders. Prevention is considered as the key strategy for controlling the obesity outbreak, 44 because treatment modalities are largely ineffective. 45
Maternal obesity is associated with reduced offspring's immune system and might be related to increase in the risk of asthma and other diseases in offspring, because of the controversial data on the role of interpregnancy weight change and its consequences on the offspring46,47; preconceptual weight control should be underscored. 48
Although the relationship between childhood obesity and asthma is well documented, we suggest that the following studies are needed: interventional studies about the effect of weight loss on the clinical outcomes of asthma in children, the effect of obesity on the efficacy of medications used for asthma control, and studies considering gender to develop more accurate weight-loss strategies in obese asthmatic children. Further research is needed on the relationship between obesity and allergy, AD, and autoimmune diseases, as well as on the effect of childhood overweight/obesity on the immune cells' function. This can illuminate the underlying mechanisms on the relationship between childhood obesity and the immune system.
Study Limitations and Strengths
Of 26 included studies, 7 were systematic reviews and others were narrative studies: out of 7 systematic reviews, 5 had dealt with the relationship between childhood obesity and asthma. This study suggests that enough evidence exists for confirming the obesity–asthma relationship in children, and also shows lack of enough systematic reviews to strongly investigate the relationship between obesity and other diseases and the immunological changes in the pediatric age group. The other limitation is that although the risk of type 2 diabetes and insulin resistance is greatly influenced by obesity, and the immune system also plays a role in this relationship, we did not study this topic because of its too broad spectrum.
The strength points of this study are that a combination of the systematic and narrative reviews on the association of childhood obesity with proinflammatory cytokines of TNF-α, IL-6/leptin, and CRP as well as anti-inflammatory cytokine of IL-10/adiponection is performed. More interestingly, this review has focused on the association of childhood obesity with the immune cells such as anti-inflammatory Tregs, inflammatory CD4+ Th17 cells, dendritic cells, and macrophages. Lastly, it has focused on the association of childhood obesity with the allergic diseases, including asthma and AD.
Conclusion
Obesity and overweight in infants and children might be associated with reduced immunological response and inflammatory processes, which might be related to worsening diseases or their symptoms such as asthma. In addition, maternal obesity might be associated with changes in the offspring's immune system, which might increase the risk of asthma and other diseases in their offspring.
Supplementary Data
Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/chi) shows the quality assessment of systematic articles by using AMSTAR, whereas Supplementary Table S2 shows the quality assessment of narrative articles by using INSA. Both tables contain the information about all included and not-included studies in detail.
Supplementary Box S1 shows the relevance tool we used. This relevance tool was, based on that used in the EPHPP, 12 previously mentioned in the main text.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.