
Abstract
Abstract
Objective:
This study aimed to identify cutoff points for detecting hypertriglyceridemic waist phenotype (HTWP) in adolescents and to investigate the association of the HTWP with insulin resistance (IR) and metabolic syndrome components.
Methods:
A multicentric cross-sectional study of 861 adolescents (10–19 years of age, 504 girls) was conducted. Pubertal stage, anthropometric, and laboratory parameters were assessed. IR was assessed by Homeostasis Model Assessment for Insulin Resistance (HOMA1-IR) index and hyperglycemic clamp (n = 80). HTWP was defined by the presence of increased plasma triglycerides (TGs) and increased waist circumference (WC) according to cutoff points obtained in ROC curve analysis given the HOMA1-IR index as a reference method.
Results:
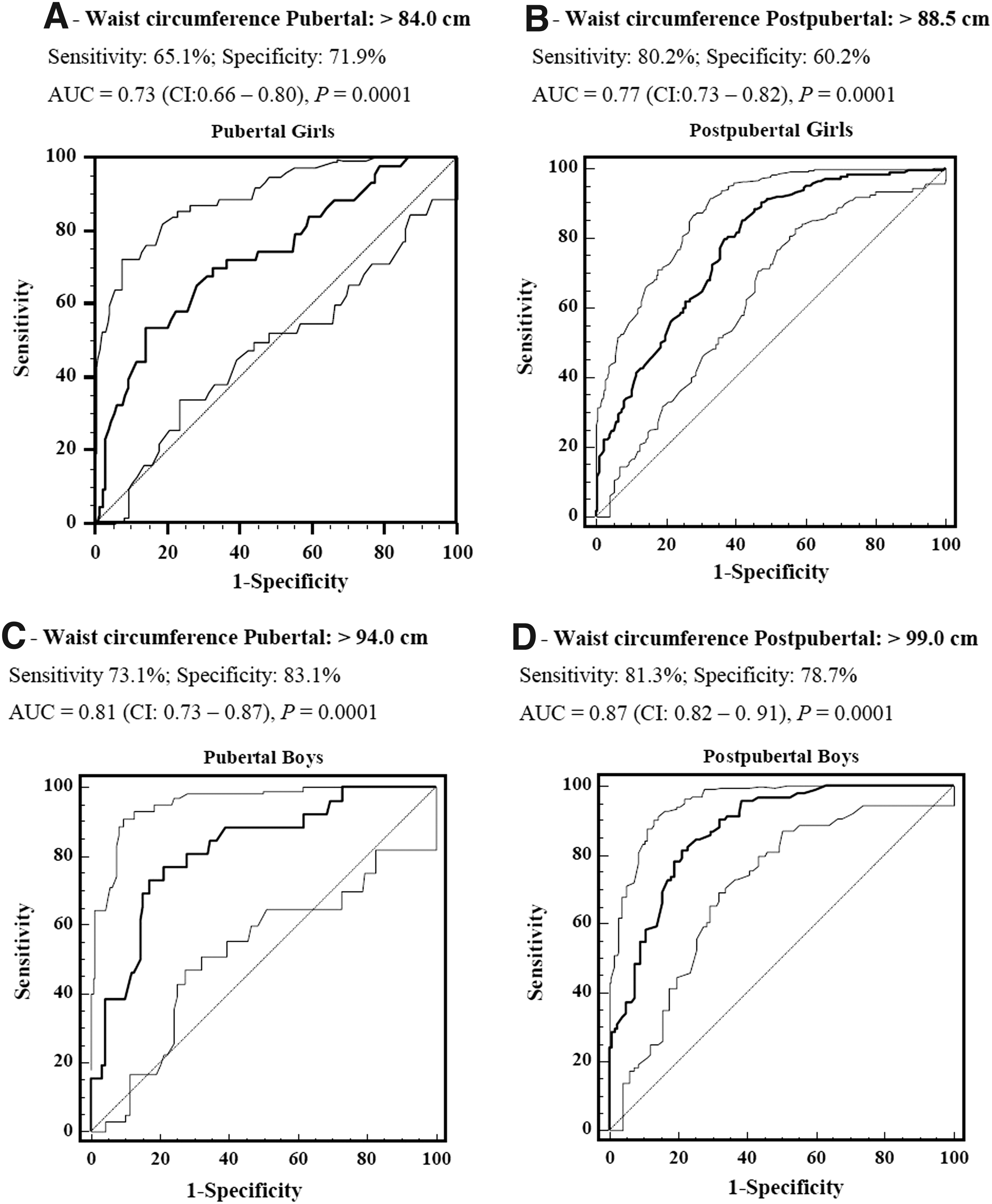
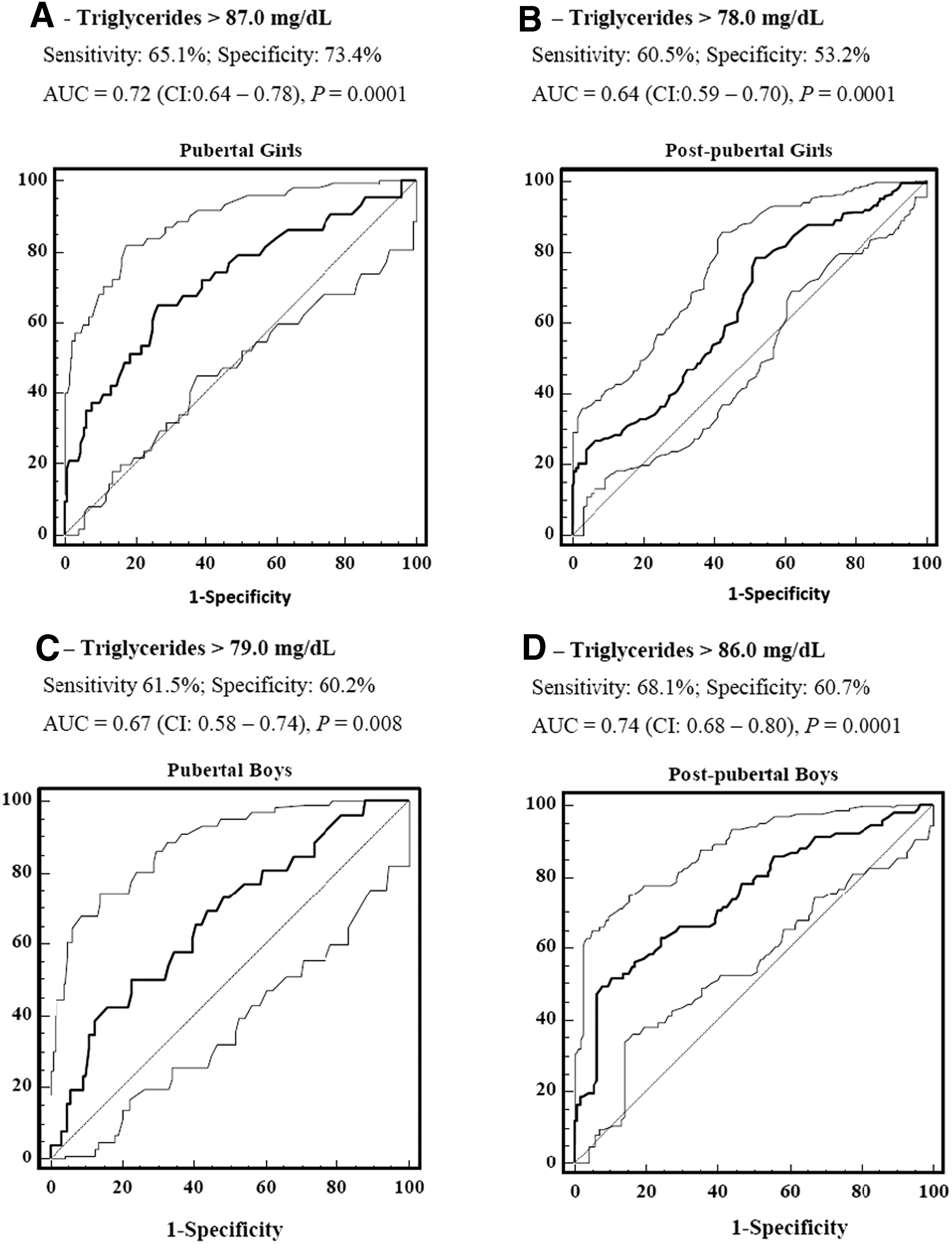
Cutoffs for WC and TGs, with a higher sum of sensitivity (S) and specificity (E), were, respectively: >84 cm (S:65.1%, E:71.9%) and >87 mg/dL (S:65.1%, E:73.4%) in pubertal girls; >88.5 cm (S:80.2%, E:60.2%) and >78 mg/dL (S:60.5%, E:53.2%) in postpubertal girls; >94 cm (S:73.1%, E:83.1%) and >79 mg/dL (S:61.5%, E:60.2%) in pubertal boys; and >99 cm (S:81.3%, E:78.7%) and >86 mg/dL in postpubertal boys (S:68.1%, E:60.7%). HTWP frequency was 27.5%. In the phenotype presence, after adjustment for age and pubertal stage, blood pressure and fasting glucose levels were elevated and high-density lipoprotein cholesterol was lower (p < 0.001). Adolescents with the HTWP showed more IR, evaluated both by the HOMA1-IR and by the clamp test (p < 0.003).
Conclusion:
The findings suggest HTWP as an IR status in adolescents. Cutoff point standardization for gender and pubertal stage, combined with the ease of application of the method, may allow their use for screening adolescents who would most benefit from lifestyle changes.
Introduction
The increase in overweight and obesity prevalence has been observed in adolescents. In Brazil, from 1974 to 2009, overweight among adolescents almost quadrupled, reaching a prevalence of 21.5%. 1 The increase in overweight prevalence favors comorbidities increasing such as metabolic syndrome (MS). 2 National data identified a 6.4% MS prevalence in adolescents, increasing the risk for developing cardiovascular diseases. 3
MS has in its pathophysiological basis the accumulation of visceral fat and the presence of insulin resistance (IR). 4 In children and adolescents, MS diagnosis is still under discussion because of a lack of consensus on their components and cutoff points. This can be explained by the fact that in pediatrics, there are no follow-up studies that have compared the effect of the combination of cardiovascular risk factors used in the definition of MS, with the same risk factors isolated. 5
Puberty is a period of rapid change in which a child, in physiological terms, becomes an adult capable of reproducing. During pubertal development, the concentrations of sex hormones and adipocytokines change dramatically. Studies measuring in vivo IR have shown that insulin levels are higher during puberty when compared with insulin levels in adulthood and in the years preceding puberty. 6 During this period, there is a physiological and transient IR, which is partly explained by the increase of sex hormones and the increased secretion of growth hormone, which still remains under investigation. 6 In children with no diabetes, IR reaches its highest levels by 12 to 14 years of age (Tanner puberty stage 3) in both genders, returning to prepubertal levels after 16 years of age (Tanner 5). This fact makes it difficult to compare studies and determine cutoff points for IR identification of this group.7,8
In 2000, Lemieux et al. 9 demonstrated that the combination of only two MS components, increased plasma triglycerides (TGs) and waist circumference (WC), was able to predict cardiovascular risk in adult men. The presence of concomitant increase in plasma TGs and WC was called hypertriglyceridemic waist phenotype (HTWP). The authors found that WC measurement was positively correlated with apolipoprotein B and insulin levels, and levels of TGs correlated positively with the small and dense low-density lipoprotein (LDL) cholesterol levels. The study found that over 80% of men with this phenotype were characterized as carriers of the atherogenic metabolic triad. In addition, the authors considered this phenotype as a simplified definition of MS. 9 Subsequently, another study obtained similar results for the female population. 10
In 2006, Esmaillzadeh et al. 11 demonstrated that HTWP is a good marker to identify MS risk and other metabolic abnormalities such as reduced high-density lipoprotein (HDL) cholesterol and increased LDL cholesterol and very low-density lipoprotein cholesterol in Iranian adolescents. Other subsequent studies confirmed those findings.3,12–16 Moreover, little is known about the relationship between HTWP and IR as evaluated by dynamic tests in adolescents; and about the association between HTWP, insulin sensitivity, and the risk of incident type 2 diabetes. We hypothesized that HTWP is an insulin-resistant state that increases diabetes risk.
Accurate evaluation of in vivo IR can be performed with an euglycemic hyperinsulinemic clamp or through hyperglycemic techniques; the first is considered the gold standard.17,18 However, neither technique is applicable in clinical practice because they are invasive, highly complex, and expensive.17,19
In the current epidemiological panorama, identifying a consensual, practical, and affordable screening method to evaluate IR in adolescents is necessary. The objectives of this study were (1) to identify cutoff points for detecting HTWP in adolescents and (2) to investigate the association of HTWP with IR and MS components in adolescents.
Materials and Methods
Study Design and Study Sample
This is a multicentric cross-sectional study, which is part of a more comprehensive investigation entitled the Brazilian Metabolic Syndrome (BRAMS) Study, which is a study on the clinical, anthropometric, metabolic, and hormonal aspects of IR syndrome, which included adolescents from three cities in the state of São Paulo (São Paulo, Itu, and Campinas).
The volunteers were included using a nonprobabilistic intentional sample, consisting of adolescents from the Clinic of Obesity in Children and Adolescents at Clinical Hospital of Campinas University, from the Sao Paulo Hospital of Federal University of Sao Paulo, and from Health Units and institutions offering educational programs for adolescents from the three cities in the study. From a database of 1033 adolescents, a total of 861 adolescents were selected; those selected for inclusion were of both genders, 10 to 19 years of age, and either pubertal or postpubertal.
There was no inclusion of adolescents with developmental delay, genetic syndrome, liver disease, nephropathy, metabolic disorders (such as hypothyroidism, hyperthyroidism, and type 1 diabetes), and using systemic corticosteroids.
This study was approved by the Research Ethics Committee of the University of Campinas (UNICAMP), protocol number 900/2010. All parents or guardians of the adolescents signed the Free and Clarified Consent Term.
Clinical Evaluation
Blood pressure (BP) was assessed using the auscultation technique with a mercury column sphygmomanometer and cuff with a rubber bag of appropriate size to the circumference of the adolescent's arm, following the procedures recommended by the Brazilian Society of Cardiology. 20
Assessment of sexual maturation was performed by self-evaluation according to the criteria proposed by Tanner. 21
Anthropometric Assessment
Body weight and height were assessed according to the techniques proposed by Gordon et al. 22 From these measurements, the BMI percentile for age and gender was determined using the software, Epi Info® version 3.5.2.
The classification of nutritional status according to BMI for age and gender was performed following the CDC criteria described as follows: normal weight ≥percentile 5 and <85 percentile; overweight ≥85 percentile and <95 percentile; and obesity ≥95 percentile. 23
WC was measured with inelastic measuring tape in the middle point between the iliac crest and the last rib in the end-expiratory phase without the compression of tissues. 24
Determination of the Waist hypertriglyceridemic phenotype
HTWP was defined by the simultaneous presence of raised TGs and WC. The cutoff points for WC and TGs were determined from ROC curves, using the Homeostasis Model Assessment for Insulin Resistance (HOMA1-IR) index as the reference method. The cutoff points used for setting IR by HOMA1-IR were obtained from the BRAMS study: 4.07 for pubertal adolescents and 2.91 for postpubertal adolescents.
Insulin Resistance Assessment
IR was measured by two methods, a fasting test and a dynamic test. The HOMA1-IR was the fasting test, obtained by the mathematical model: [Fasting insulin (μU/mL) × fasting glucose (mmol/L)]/22.5.17,19
The hyperglycemic clamp was the dynamic test in a subsample of 80 adolescents. In the subsample composition, 50% of adolescents were male, there was a similar proportion of pubertal and postpubertal adolescents, and there was the same distribution of nutritional status compared with the total sample. After a 12-hour overnight fasting, there were two venous punctures: the first was in a superficial arm vein, where all blood samples were held; and the second was in the other arm, where another cannula was inserted into a vein for a 25% glucose solution infusion. Glucose infusion was divided into two phases: the first dose, which comprises a sufficient amount of glucose to acutely raise blood glucose levels to 225 mg/dL plateau, and the maintenance dose, which comprises a sufficient amount of glucose to maintain blood glucose to 225 mg/dL plateau during the 2-hour test duration. Insulin sensitivity was evaluated by the insulin sensitivity index (ISI) and was measured according to the average rate of glucose infusion during the last 60 minutes of the clamp (mg·kg·min−1) test minus urinary glucose excretion, with an adjustment for fat-free mass, and divided by the mean insulin concentration of five dosages during the same period. 25
Assays
For biochemical evaluation, venous blood samples were collected after 12-hour overnight fasting and stored at −20°C for later analysis.
The measurements comprised glucose plasma concentrations (K082-2; Bioclin Therapeutics, San Ramon, CA), total cholesterol (TC) (K 015; Bioclin), LDL cholesterol (K088; Bioclin), HDL cholesterol (K071-23; Bioclin), and TGs (K 117; Bioclin) that were measured through the automated enzymatic method and colorimetric methods. Plasma insulin was determined by chemiluminescence (Immulite 1000 System, Siemens Diagnostics Health, Los Angeles, CA).
Statistical Analysis
Data analysis was performed using the Statistical Package for Social Sciences (SPSS) software, version 20. The significance level was 5%. For quantitative variables, data were presented as median and interquartile range (percentiles 25% to 75%). Categorical variables were expressed as percentages and compared using the chi-square test. The Kolmogorov–Smirnov test was applied in the exploratory data analysis to assess the normality of the data. The Mann–Whitney U test was used for comparison of two independent groups. Analysis of covariance (ANCOVA) was used to compare the distribution of averages of MS components among individuals with HTWP against those with none or one change in the two components of the phenotype. The covariates used in the analysis were age and pubertal stage. Subsequently, the Sidak post hoc test was used to investigate significant statistical difference in those who had HTWP compared with other groups. ROC curves were constructed and separated by gender and pubertal stage to identify WC cutoff points. Therefore, the WC and TG cutoff points chosen were those that obtained the highest sum between Sensitivity (S) and Specificity (E) reflecting fewer false positives and fewer false negatives and, simultaneously, at least minimum values of 60% for S and E to IR identification.
Results
Table 1 shows the clinical and biochemical characteristics of the 861 adolescents. Both the total sample and the subsample had a higher proportion of girls, pubertal adolescents, and obese adolescents. Comparing the total sample with the subsample, the majority of the variables did not present statistical difference between the groups, except the pubertal stage and age in both genders, and diastolic BP and fasting glucose for boys, ensuring subsample representativeness in relation to the total sample.
Clinical, Anthropemetric, and Metabolic Characteristics of the Adolescents Studied According to Gender
BP, blood pressure; HOMA1-IR, homeostasis model assessment for insulin resistance.
In Figures 1 and 2, ROC curves were built separately for each gender and pubertal stage to find the cutoff points for WC and TGs to establish the HTWP classification. It is known that area under the curve (AUC) value above 0.70 has a high discriminatory power. The AUCs identified ranged from 0.64 to 0.87 (p < 0.05). As expected, higher cutoff points for WC were identified for postpubertal adolescents and for boys, and no pattern was identified for TGs.
In the overall sample, HTWP frequency was 27.5% (24.6% for boys and 29.6% for girls). The exclusive increase in the TG and WC levels was 20.4% and 19.0%, respectively; and in 33.0% of adolescents, there was no increase in any of HTWP components. Among the HTWP carriers, 0.8% were classified as eutrophic, 8.0% as overweight, and 91.1% as obese. In the separate analysis by gender of those with HTWP, 85.9% of girls were obese, 12.8% were overweight, and 1.3 were eutrophic; in boys, 100% were obese.
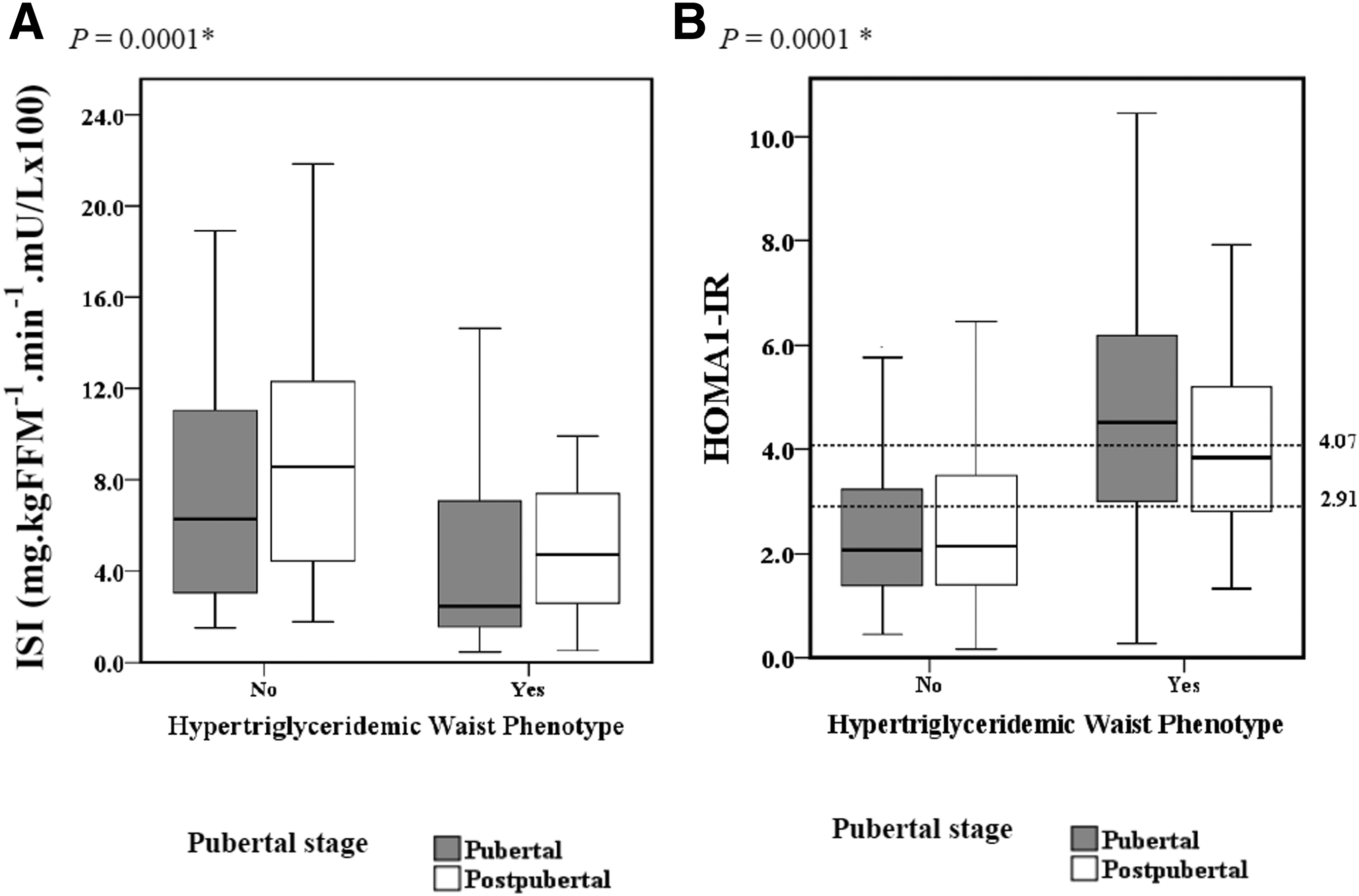
Figure 3 shows the distribution of clinical and metabolic parameters, with adjustment for age and pubertal stage, according to the presence of HTWP components. In the presence of the HTWP, HOMA1-IR index, BP levels, and fasting glucose levels were elevated, whereas insulin sensitivity evaluated by clamp and HDL cholesterol were lower in comparison with the adolescents without the phenotype (p < 0.001).

The categorization of adolescents according to the presence and absence of HTWP shows that adolescents with HTWP are more resistant to insulin, evaluated both at fasting and also under intravenous stimulus in the clamp test (p < 0.03) (Fig. 4).
Discussion
Given the need for accurate and relevant tools to pediatric clinical practice for IR screening, this study is the first to investigate HTWP performance in IR evaluation in adolescents using the hyperglycemic clamp test as a reference method. Furthermore, this study is a pioneer in identifying cutoff values for TGs and the WC to the screening IR using the HTWP.
In the scientific literature, there are different cutoff points for WC and TGs in defining HTWP in adolescents. For WC, previous studies with HTWP considered 70, 75, or 90 percentiles for age and gender of the respective samples, hindering its application.12,13,16,26,27 Moreover, there is no consensus among studies related to TGs values, ranging from 100 to 129 mg/dL,12,13,15,16,24,26,27 which are within the borderline recommended by the National Cholesterol Education Program Pediatric Panel Report, 28 ranging from 90 to 129 mg/dL.
Considering the difference between the genders and the impact of sexual maturation in WC measurement and TGs, cutoff points were obtained, separated by gender and pubertal stage: WC in pubertal girls (>84 cm) and postpubertal girls (>88.5 cm); WC in pubertal boys (>94 cm) and postpubertal boys (>99 cm); TGs in pubertal girls (>87 mg/dL) and postpubertal girls (>78 mg/dL); and TGs in pubertal boys (>79 mg/dL) and postpubertal boys (>86 mg/dL). The definition of cutoff points was based on these adolescents' IR levels. The AUCs and the sensibility and specificity values were best for boys.
HTWP prevalence has been under investigation in several works. Although this is not the focus of this study, 27.5% of adolescents had the HTWP, higher value compared with the prevalence of preliminary studies with adolescents from other countries that found values of the order of 6.4%, 11 7.3%, 13 and 8.5%. 12 In studies with Brazilian adolescents, the overall prevalence was 6.4%, 7.2%, and 20.7%.3,14,15 The high HTWP frequency in this study can probably be explained by our convenience sample that obtained part of the adolescents from clinics and units of health and by the increased adiposity in the adolescents studied because more than half were obese (52.6% girls and 53.0% boys) and, among those with the phenotype, 91.1% were classified as such, corroborating the findings of Esmaillzadeh et al. 11 and Conceição-Machado et al., 14 who observed this phenotype in 38.7% and 63.4% of obese adolescents, respectively. Distinct values of HTWP prevalence may also be because of different cutoff points used to define the phenotype as well as the change in anatomic location of WC measurement. The high frequency of HTWP identified in obese adolescents indicates the need for surveillance and for clinical and nutritional follow-up of this age group.
In adults, HTWP has been considered an accessible and more accurate tool than the simple use of BMI and/or WC for screening metabolically unhealthy obese individuals, characterized by IR and an atherosclerotic profile. However, when HTWP is reported in adolescents, the impact of the sexual maturation process must be taken into consideration. A well-conducted recent study showed that during puberty, adolescents who initiate a growth spurt do not necessarily remain insulin sensitive throughout the sexual maturation process. 5 In this case, when analyzing associations between HTWP and metabolic alterations in adolescents, the use of age as a covariate does not provide the finest setting for the influence of hormonal changes and body composition that occur during puberty.
In the present study, after adjusting for age and pubertal stage in the presence of HTWP, the MS markers (BP, glycemia, insulin, and HOMA1-IR) increased, and HDL cholesterol and ISI averages were lower compared with individuals who did not have the phenotype. Accordingly, other studies in adolescents with adjustments only for age showed that HTWP was positively associated with fasting glucose, 12 lipid profile (high levels of TC and LDL cholesterol and low HDL cholesterol levels), higher levels of BP,11,14 and worse cardiometabolic score. 16 Moreover, in these studies, the association between HTWP and all previously mentioned parameters was not supported consistently. Such a difference from the present study may be explained by the high number of adolescents who are overweight, strengthening these associations. Hosseinpanah et al. 29 suggest that HTWP is a simple marker for identifying adolescents at risk of developing MS because combinations of individual components as low-serum HDL cholesterol levels associated with high TG serum and abdominal obesity levels favor MS screening and prevent the risk of cardiovascular diseases in adolescents.
Regarding the IR, in this study, higher means of HOMA1-IR index and lower ISI in adolescents with HTWP were identified. Compared with previous studies, the study of Buchan et al. 16 evaluated HOMA1-IR and found that in the presence of HTWP in adolescents, HOMA1-IR index is higher compared with adolescents without the phenotype. Carlsson et al. 30 investigated the association between HTWP and insulin sensitivity evaluated with a hyperinsulinemic euglycemic clamp in 1026 elderly men. In the beginning of the study, those without the HTWP had higher levels of insulin sensitivity with the clamp compared with those who had the phenotype [6.8 mU/L (1.7) vs. 3.9 mU/L (1.4); p < 0.05], respectively. The elderly men with the HTWP had a higher risk of developing type 2 diabetes compared with those without the HTWP (odds ratio 4.64, 95% CI 1.61–13.4, p = 0.004) during the study. Those findings are in agreement with the results of our hyperglycemic clamp study because adolescents with HTWP had lower ISI averages compared with those without the phenotype (p < 0.0001).
The strength of the present study relies on the assessment of a large sample of adolescents with the utilization of a robust dynamic test for the IR measurement, 31 although the hyperglycemic clamp test is not the gold standard for IR evaluation, previous studies with adolescents have shown strong correlation of IR assessed by hyperglycemic clamps and euglycemic hyperinsulinemic clamps. Correlations were r = 0.82, p = 0.005, 18 and r = 0.90, p < 0.001, 31 in adolescents with different levels of adiposity and glucose tolerance.
This study has some limitations. The results are based on a cross-sectional analysis, which does not allow inferring causality. The sample was selected for convenience, with a higher proportion of obese, which does not reflect the nutritional status of Brazilian adolescents.
The pubertal stages of the study adolescents were determined using the self-reported Tanner. Although the utility of this self-reported stage is consolidated, the Tanner pubertal questionnaire can result in discrepancies between self-reported stage and the actual pubertal stage because of many aspects, including cultural influences and self-image. 32
The findings suggest that HTWP is an IR state and an important indicator of metabolic health among Brazilian adolescents. Cutoff point standardization, combined with the ease of application and the low cost of the method, may allow the use of the HTWP in clinical practice and in epidemiological studies for screening IR adolescents who would most benefit from changes in lifestyle.
Footnotes
Acknowledgment
The authors acknowledge the support of National Council of Scientific and Technological Development (CNPq), process no. 563664/2010-0 and Coordination for the Improvement of Higher Education Personnel (CAPES) 01-P-4346-2015.
Author Disclosure Statement
No competing financial interests exist.