
Abstract
Abstract
Background:
To examine feasibility and initial efficacy of having previously treated parents serve as peer interventionists in family-based behavioral weight management treatment (FBT).
Methods:
Children aged 7–11 years with overweight/obesity and parents (n = 59 families) were enrolled in one of two pilot trials, the EPICH (Engaging Parents in Child Health) randomized trial comparing professional versus peer FBT delivery or the Parent Partnership trial, which provided professionally delivered FBT to families (first generation) and then randomly assigned first generation parents to either be or not be peer interventionists for subsequent families (second generation). Efficacy (child zBMI change), feasibility, and costs for delivering FBT, and impacts of being a peer interventionist were examined.
Results:
In EPICH, families receiving professional versus peer intervention had similar decreases in child zBMI and parent BMI, with markedly lower costs for peer versus professional delivery. In Parent Partnership, families receiving peer intervention significantly decreased weight status, with very preliminary evidence suggesting better maintenance of child zBMI changes if parents served as peer interventionists. Previously treated parents were willing, highly confident, and able to serve as peer interventionists in FBT.
Conclusions:
Two pilot randomized clinical trials suggest parents-as-peer interventionists in FBT may be feasible, efficacious, and delivered at lower costs, with perhaps some additional benefits to serving as a peer interventionist. More robust investigation is warranted of peer treatment delivery models for pediatric weight management.
Introduction
Overweight and obesity in childhood continues to be highly prevalent in the United States.1,2 These children need interventions that prevent tracking high weight status into adulthood and to decrease physical and psychosocial consequences.3,4 The U.S. Preventive Services Task Force recommends screening and referral for these children to “moderate- to high-intensity programs [that] involve >25 hours of contact” focusing on diet, physical activity, and behavioral counseling. 5 Family-based behavioral treatment for weight management (FBT) that focuses on parents and their children changing eating and physical activity behaviors demonstrates efficacy among elementary school-aged children (6–12 years old) with overweight/obesity.6–8 However, very few children receive this intense treatment, in part, because of high delivery costs. 9
Lower intensity pediatric weight management interventions are less costly and more feasible, but demonstrate weak or no efficacy8,10,11 perhaps due to the lessened accountability, fewer opportunities for education and skills training, and less frequent problem-solving and feedback often present in more intense behavioral interventions. Internet-based and other remote interventions could reduce treatment costs, but have often been used only as adjunctive to intense direct contact interventions. 12 Indeed, meta-analyses suggest that in-person contact may significantly contribute to the success of pediatric weight management interventions. 13
An approach that could maintain intensity while reducing costs is treatment delivery by nonprofessionals. Interventions led by paraprofessionals (e.g., community health workers) have demonstrated feasibility and efficacy for changing child health conditions and behaviors. 14 For example, recent studies found improvements in children's weight-related behaviors through promotora/community health worker interventions with Latino families.15,16 The community health worker approach has the likely benefit of being more community-tailored, although does not necessarily only incorporate interventionists who are struggling with the same health issues as the intervention focus population.
One promising intervention strategy is linking individuals who share a common behavior change interest, such as peer-to-peer models, having individuals who themselves have received treatment for that problem then provide the intervention to subsequent generations of treatment seekers. 17 This article reports on initial testing of the feasibility, acceptability, efficacy, and cost of treated parent-turned-peer interventionist model in two pilot treatment trials [the Engaging Parents in Child Health (EPICH) and Parent Partnership trials]. Preliminary evidence is presented on whether serving as a peer interventionist impacts peers' and their child's long-term weight outcomes. To our knowledge, this is the first evaluation of such an approach.
Methods
Participants
Participants were 7–11-year-old children with a measured BMI ≥85th percentile for their age and sex based on population norms published in 2000 by the U.S. Centers for Disease Control and Prevention. 18 Additional inclusion criteria were child and parent (1) had no medical condition or recent start to medication that is weight affecting, (2) had no eating disorder or mental health condition that would interfere with treatment participation, (3) were able to be moderately physically active >10 minutes at a time, and (4) were able to engage in treatment conducted in English. In addition, the child needed to have at least one parent with a BMI ≥25 (based on self-report), although this did not have to be the participating parent. Participants were recruited through mailed flyers using addresses purchased from a marketing company, radio advertisements, and word of mouth. Participant demographics are provided in Table 1. Participant flow information for each trial is presented in Figures 1 and 2.
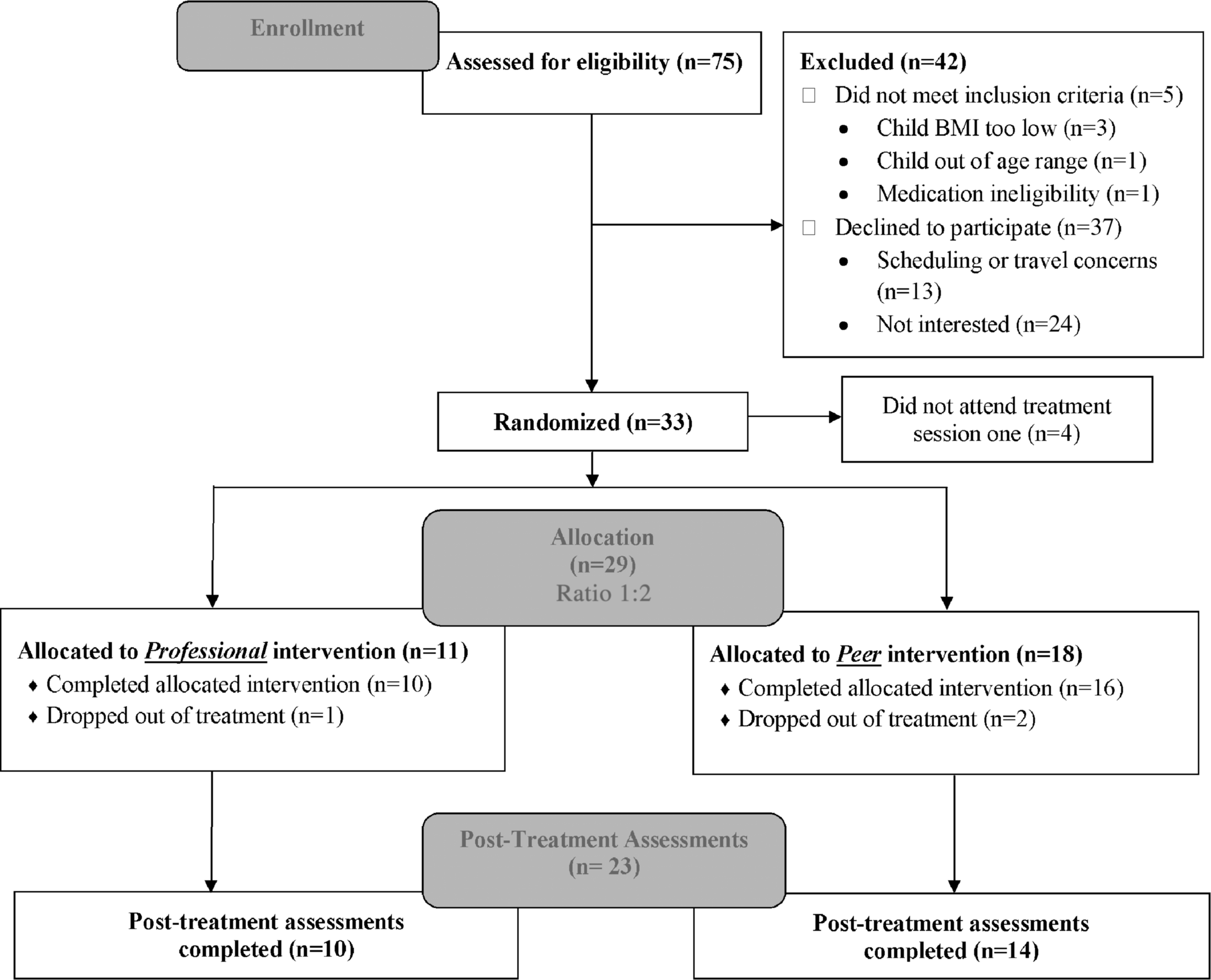
Participant flow for the EPICH trial. EPICH, Engaging Parents in Child Health.

Participant flow for the Parent Partnership trial.
Sample Characteristics for the Treatment Enrollees and Peer Interventionists in the Engaging Parents in Child Health and Parent Partnership Trials
Information from four of the peer interventionists is also included in the household/income and parental marital status data in the “Treated by Professionals” portion of the Parent Partnership trial.
Values for the “families treated” columns are for the child participant receiving treatment where applicable and values for the “peer interventionists” column are for the peers themselves.
One parent in EPICH and two parents in Parent Partnership declined to report annual household income.
EPICH, Engaging Parents in Child Health.
Trial Overviews
EPICH used a parallel design, with families randomly assigned by flipping a coin to receive either FBT delivered by professional interventionists or by parents who had previously received FBT (peers) (allocation 1:2), with children first stratified based on sex and level of percent above median BMI for age and sex (> or <60%) and block sizes of 3 within each strata. EPICH peer interventionists were recruited from among parents who had completed one of our FBT trials in the past 3 years. EPICH families receiving treatment were measured at baseline and posttreatment, with no follow-up assessments. EPICH treatment was conducted in two cohorts January 2013–March 2014.
The Parent Partnership trial first recruited families to receive FBT delivered by professionals (first generation). After receiving treatment, first generation parents were randomly assigned to be or not be peer interventionists for the next generation of families (second generation). Thus, all second generation Parent Partnership families received only peer-delivered intervention. All Parent Partnership families were evaluated before receiving treatment (baseline) and after receiving treatment (posttreatment). The first generation families completed posttreatment assessments before knowing whether they had been randomized to be a peer or not. Follow-up assessments were conducted 6 months and 1 year after receiving treatment ended for all first generation families. For first generation parents who served as peer interventions to the second generation families, the 6-month follow-up assessment coincided closely (<3 weeks) with the end of their delivering treatment to second generation families. Only a 6-month follow-up assessment was conducted among second generation families. Parent Partnership treatment was conducted April 2013–March 2014.
Both trials were approved by the Seattle Children's Research Institute (SCRI) IRB, and parents consented and children independently assented to study participation following phone calls with research staff describing the trials and in-person presentations and opportunities for questions about the trials and study participation. All assessments and treatment were conducted at SCRI.
FBT Format and Content
FBT was structured similarly for professional and peer interventionist delivery in both trials. The 20 session FBT is based on social cognitive theory and was adapted from our and others' existing evidence-based interventions.6,19–21 Children and at least one of their parents or caregivers attended weekly in-person sessions, which included 30 minutes individual family sessions with a consistent interventionist and separate 45 minutes child and parent group sessions (usually 6–12 members per group). Interventionists conducted protocol-based sessions with one to three families on a treatment evening, with sessions oriented toward helping families learn and implement behavioral skills for eating and physical activity change. For both professional and peer interventionists, if the assigned interventionist for a family was absent for a treatment session other available professional or peer interventionists substituted, respectively.
Using family and group session outlines, interventionists worked with families on implementing food/activity monitoring, goal setting and rewards, and environmental control. Feedback, accountability, and problem-solving around skills use and addressing barriers were provided in individual family sessions. Changes in food and activity environment were accomplished by having parents (1) identify these environments, (2) increase healthy food and decrease unhealthy food access, and (3) increase physical activity and decrease sedentary opportunities. Both children and parents had weekly eating and physical activity goals.
The eating plan, adapted from the Stoplight Eating Plan, focused on reducing calories, fat, and sugar intake and increasing nutrient density.22,23 Foods/beverages were categorized into GREEN (Go!), YELLOW (Caution), or RED (Stop! eat sparingly) based on fat and sugar with daily calorie goal ranges based on intake needed for children and parents to lose ∼½–1 pound per week, but set no lower than 1000 kcal/day for children and 1200 kcal/day for parents. The eating plan also targeted reductions in high-calorie, low-nutrient dense food (e.g., RED foods) consumption, partially by increasing fruit/vegetable consumption. Families were encouraged to gradually increase physical activity, with the ultimate child goal being 90 minutes per day on most days of the week, given our findings that this results in greater visceral fat loss 24 and the parent goal being 60 minutes per day. Behavioral goals were standardized initially, but adapted to individual family needs and progress.
Interventionist Training and Supervision
Professional interventionists had either masters-level or doctoral degrees in a health-related field (e.g., psychology, social work), with many having been trained and delivered FBT in prior trials. Professional interventionists new to delivering FBT and all peer interventionists received 6–8 weekly training sessions (each 1.5–2 hours long) before delivering FBT. For peer interventionists in Parent Partnership, interventionist training began 4 weeks after they ended receiving treatment. Professional and peer interventionist training focused on ways to provide FBT content and cognitive-behavioral and motivational interviewing strategies. All interventionists received 1 hour of group supervision (separate professional vs. peer interventionist supervision groups) weekly when delivering FBT, with verbal and written feedback provided based on supervisors listening to prior weeks' audiotaped individual family and group sessions.
Measures
Feasibility of having peers serve as interventionists was examined by the willingness of parents in Parent Partnership to accept the peer role (if randomized) and peers' attendance at trainings and treatment sessions. After intervention training, peer interventionists also completed surveys regarding their level of confidence in treatment delivery on nine items using 11-point scales (0 = Not at all confident to 10 = Completely confident).
Treatment acceptability for families receiving treatment was examined by treatment dropout, defined as not attending >5 treatment sessions, number of sessions attended, and perceived satisfaction. Overall satisfaction for specific treatment components among families receiving treatment was evaluated via parent-report at posttreatment on 28 items using 5-point scales (1 = Not at all to 5 = Very much). To examine intervention fidelity, a trained coder blind to study purposes rated interventionists' treatment delivery among randomly selected and anonymized audiotapes of individual family sessions (EPICH—24 professionally delivered and 36 peer-delivered sessions; Parent Partnership—29 professionally delivered and 27 peer-delivered sessions). The coder used 3-point scales (1 = Not at all, 2 = Used somewhat, 3 = Definitely or a lot) to evaluate how much different interventionist strategies were used in family sessions to deliver FBT based on 21 prescribed interventionist behaviors (e.g., instructed or evaluated use of food monitoring), six proscribed/discouraged interventionist behaviors (e.g., praising weight change rather than behaviors that led to weight change), and the use of personal examples (e.g., ways that interventionist himself/herself ate healthfully). Another independent coder rated 20 of these audiotaped family sessions to examine interrater reliability, with intraclass correlations demonstrating borderline to good reliability (0.70 for prescribed behaviors scale, 0.46 for proscribed behaviors scale, and 0.47 for use of personal examples item).
Children and parents were weighed in triplicate in light clothing without shoes using a digital Scaletronix scale, with additional measurements until three of four consecutive were within 0.1 kg and then averaged. Child and parent height were measured with a Heightronic stadiometer. Height was measured in triplicate, with further measurements until three of four consecutive were within 0.5 cm and then averaged. BMI was calculated as kg/m2. Children's zBMI, the primary outcome, was calculated using U.S. Centers for Disease Control and Prevention growth charts for age- and sex-specific median, standard deviation, and distribution skewness correction, and the LMS (lambda-mu-sigma) method. 18 Changes in child weight, height, BMI, and percent overweight are provided for assessment completers (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/chi). Anthropometrics were not assessed among professional interventionists or among the EPICH peer interventionists at any point in either of the present trials.
Parents reported on the demographics of their child and themselves through surveys at baseline.
Health and Behavioral Outcome Analysis
Differences in treatment feasibility and acceptability between families receiving professional- and peer-delivered intervention in EPICH were examined via analysis of variance (ANOVA). Repeated measures ANOVA was used to evaluate baseline to posttreatment change in child zBMI in both trials, with the interaction between condition (receiving professional- vs. peer-delivered intervention) and time examined in EPICH. Both posttreatment assessment completer analysis and intent-to-treat analysis for families enrolled (baseline carried forward for missing) were conducted, with all families attending one or more treatment sessions considered enrolled. Enrollment targets were based on resources available to recruit for and conduct the trials, but sample sizes were lower than expected. Very small sample sizes precluded statistical comparisons for follow-up assessments in Parent Partnership, so only descriptive statistics are provided.
Economic Analysis
The costs of delivering treatment in both trials were assessed in 2015 U.S. dollars from the payer perspective, excluding any out of pocket or indirect time costs incurred by peers. All costs were calculated from a payer perspective with total costs calculated by multiplying a unit cost for each component of resource use (i.e., interventionist time). Peer time is not measured using a microcosting approach, as costs for peers included the $400 stipend provided to each peer for training/supervision and delivering FBT and costs of professionals to provide training and supervision to peers (estimated at same cost as professional interventionists). 25 The time spent by professionals and peers receiving training and supervision and delivering FBT was tracked in 15-minute increments. Professionals' hours were multiplied by their hourly wage, which averaged $32.50/h and cost approximately $62/h total, including fringe (26%) and overhead (51%). Families were not provided any compensation for receiving treatment.
Results
Feasibility in Serving as a Peer Interventionist
For EPICH, 50 parents from prior FBT trials were contacted to gauge interest in being a peer interventionist. Among these, 28 expressed interest and 10 participated as EPICH peer interventionists, with scheduling conflicts being the primary reason that interested parents did not become peer interventionists. In Parent Partnership, only first generation parents who attended at least 70% of sessions when receiving FBT were included in randomization to be a subsequent peer interventionist or not (n = 9 of 11), with no other selection criteria (e.g., treatment success). In Parent Partnership, five of the nine eligible first generation parents were randomly assigned to be peers, but one parent refused randomization due to a scheduling conflict, resulting in four peer interventionists who treated second generation Parent Partnership families. All peers who entered training went on to serve as peer interventionists.
Feasibility and Acceptability
Both EPICH and Parent Partnership peer interventionists reported high levels of confidence in delivering FBT (Supplementary Table S2). Peers had high attendance at intervention training sessions (mean = 88% of training sessions attended). Peer interventionists always delivered parent and child group sessions when expected in EPICH and Parent Partnership. Across all individual family sessions in both trials, 99.7% were delivered by peers when expected and 100% delivered by professionals when expected. When examining interventionist substitution for another interventionist (e.g., due to illness, vacation, or schedule conflict) in individual family session delivery, 7% of professionally delivered sessions had a substitute professional, and 12% of peer-delivered had a substitute peer.
Attrition and treatment session attendance among families receiving treatment did not differ significantly based on professional versus peer delivery. Among enrolled EPICH families (n = 29), 9.1% and 11.1% of families receiving professionally and peer-delivered treatment dropped out of treatment, respectively, with no significant difference in number of treatment sessions attended [professionally delivered mean = 13.7 sessions out of 20, standard deviation (SD) = 5.8; peer-delivered mean = 12.7 sessions, SD = 5.3]. Among enrolled Parent Partnership families (n = 30), 35.3% and 30.8% of families receiving professionally delivered (first generation) versus peer-delivered (second generation) intervention dropped out of treatment, respectively, with no significant difference in number of sessions attended (professionally delivered mean = 11.1 sessions, SD = 7.3; peer-delivered mean = 12.4 sessions, SD = 7.2).
Intervention fidelity ratings of family sessions within EPICH suggested no significant differences between professional and peer intervention delivery in prescribed or proscribed interventionist behaviors. Peer interventionists (mean = 2.3 ± 0.9) were significantly more likely to use personal examples about their own families' health behavior changes than professional interventionists (mean = 1.2 ± 0.5; p < 0.001). In Parent Partnership, professional interventionists (mean = 1.9 ± 0.2) engaged in significantly more prescribed interventionist behaviors during family sessions than peer interventionists (mean = 1.7 ± 0.3; p < 0.004), but they did not differ on proscribed interventionist behaviors. Peer interventionists (mean = 2.2 ± 1.0) again were significantly more likely to use personal behavior change examples than professional interventionists (mean = 1.2 ± 0.5; p < 0.001).
Treatment satisfaction was consistently high, with no significant differences in EPICH between families who received professional- and peer-delivered treatment. In Parent Partnership, the professionally delivered parent group sessions received significantly higher satisfaction ratings than peer-delivered parent group sessions (p < 0.007; Fig. 3), with no differences in overall treatment satisfaction or satisfaction with the individual family or child group sessions. Neither parents nor children reported any adverse events attributable to either the professional- or peer-delivered treatment in either trial.
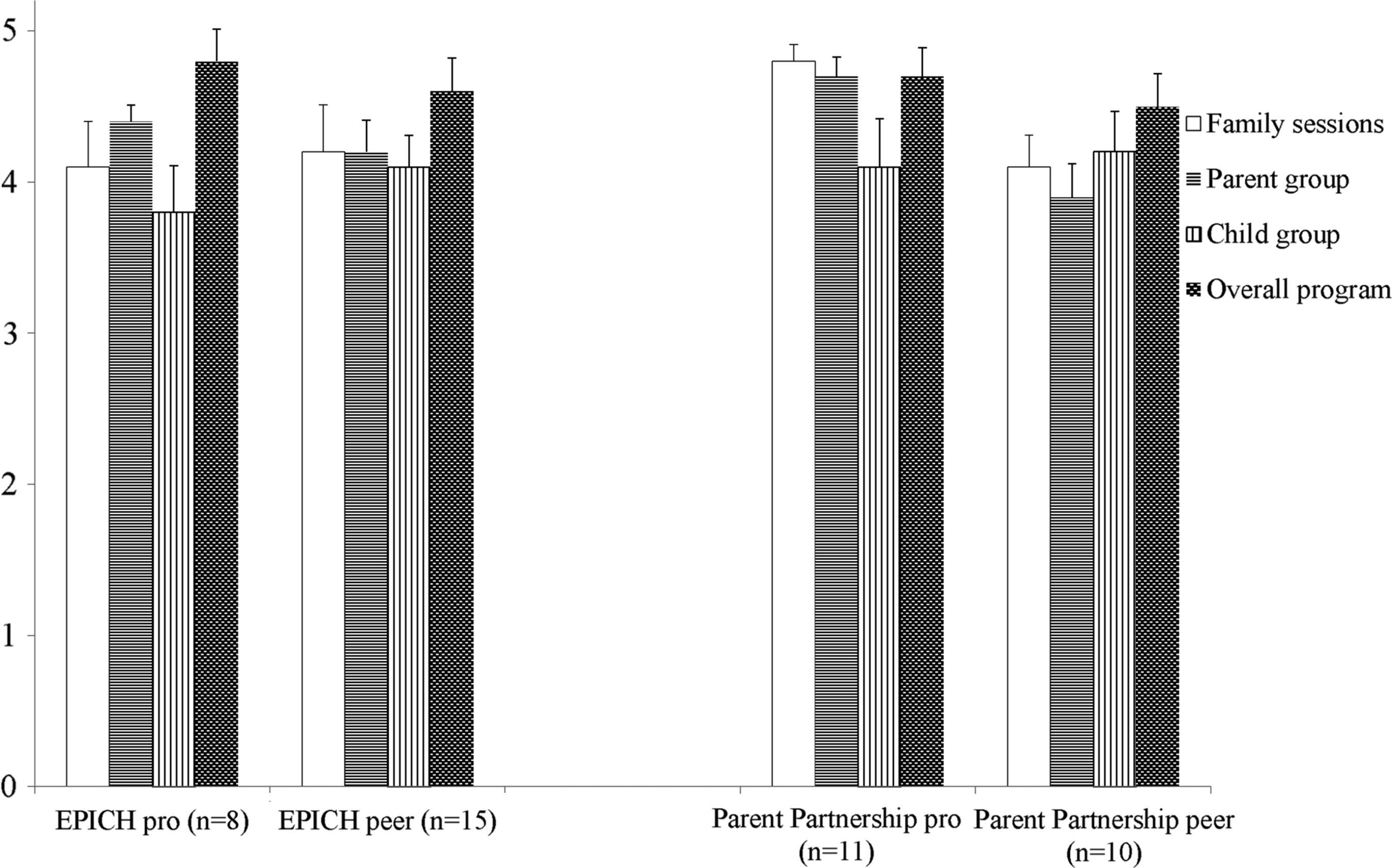
Parent-reported treatment satisfaction overall and by treatment components by interventionist type (1 to 5 point Likert scale) (mean ± standard error).
Efficacy for Change in Child and Parent Weight Status
In EPICH, child zBMI decreased from baseline to posttreatment among families provided either professionally or peer-delivered intervention (both p = 0.001), with no significant difference in change over time between these conditions among posttreatment assessment completers [condition by time interaction F(1, 22) = 1.27, p = 0.27; Fig. 4] or in intent-to-treat analysis [F(1, 27) = 2.01, p = 0.17; Supplementary Fig. S1]. Similarly, parent BMI decreased significantly with treatment (p < 0.001), with no significant differences in parent BMI change between professionally (32.2 ± 5.4 to 30.2 ± 4.7) and peer-delivered (34.0 ± 5.1 to 31.6 ± 5.5) intervention among assessment completers [F(1, 22) = 0.44, p = 0.52] or in intent-to-treat analysis [F(1, 27) = 0.26, p = 0.62].
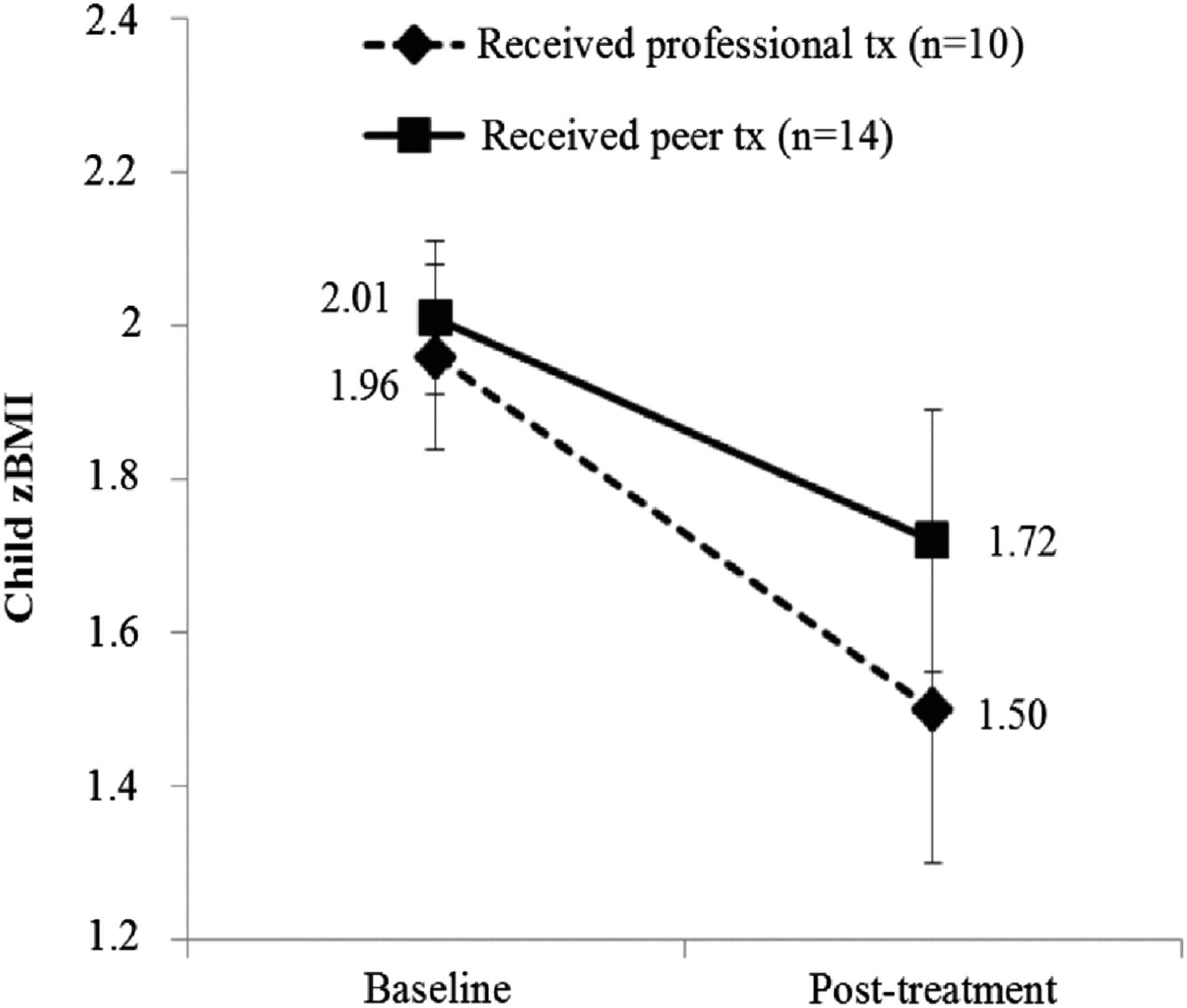
Change in child zBMI from baseline to posttreatment by interventionist type among assessment completers in the EPICH parallel randomized trial (mean ± standard error).
The assessment completer analysis in Parent Partnership revealed significant decreases in child zBMI from baseline to posttreatment among families receiving professional treatment (first generation) and among families receiving peer treatment (second generation; both p < 0.006; Fig. 5), with similarly significant decreases observed in intent-to-treat analyses (both p < 0.009; Supplementary Fig. S2). Parent BMI decreased significantly from baseline to posttreatment in Parent Partnership among assessment completers receiving professionally delivered intervention (first generation; 34.5 ± 6.1 to 31.4 ± 6.0; p < 0.003) and those receiving peer-delivered intervention (second generation; 33.6 ± 4.5 to 32.1 ± 5.0; p < 0.003), with both changes remaining significant in intent-to-treat analysis (both p < 0.026). Among second generation follow-up assessment completers (n = 9), the mean child zBMI at 6-month follow-up was 2.10 ± 0.3, and mean parent BMI was 32.2 ± 6.2.
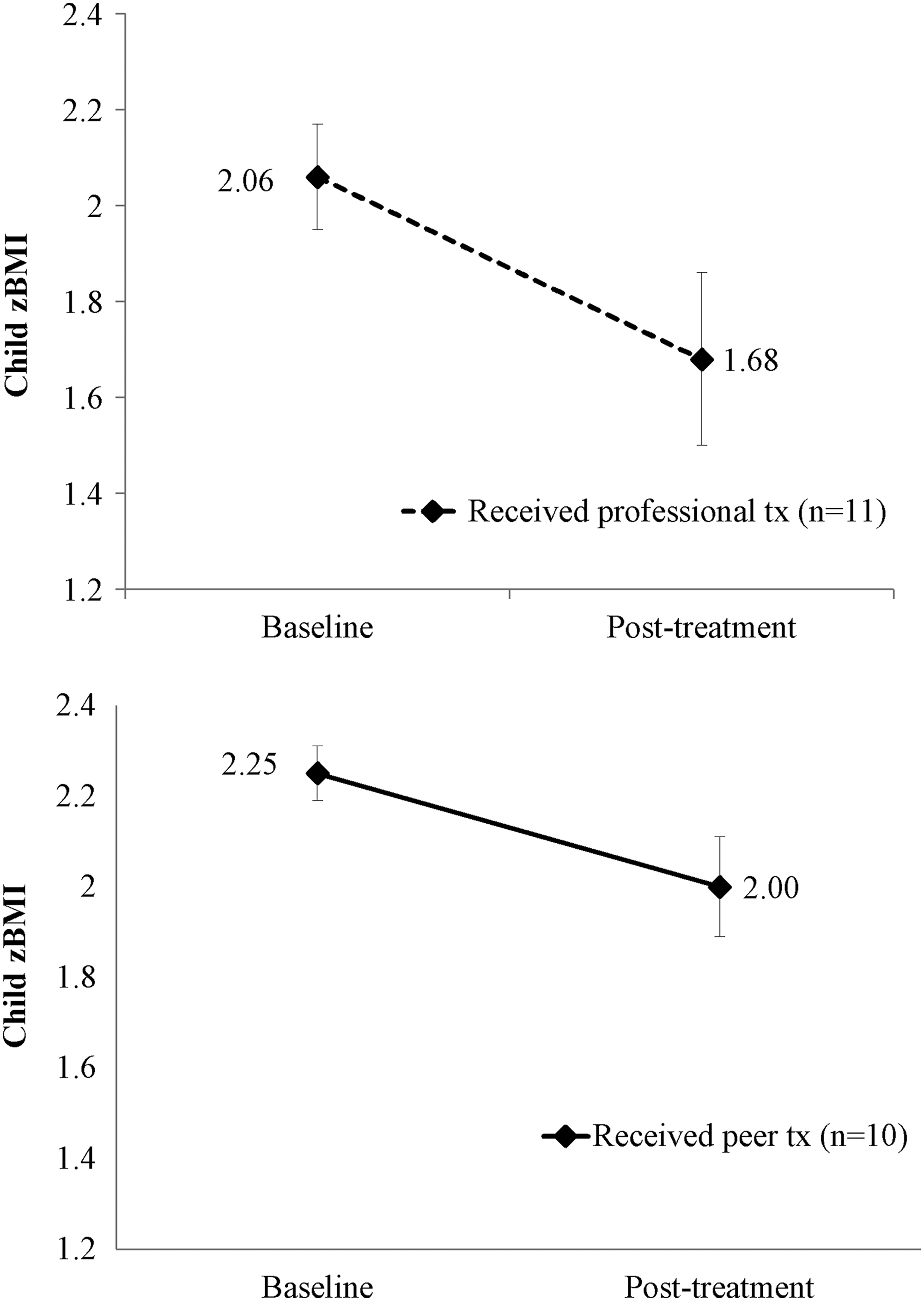
Change in child zBMI from baseline to posttreatment by interventionist type among assessment completers in the Parent Partnership trial (mean ± standard error).
Treatment Costs
Estimated costs associated with professional- versus peer-delivered training, supervision, and providing intervention are provided in Table 2. Across trials, professionals spent an estimated 1232 total hours receiving training, being supervised, and delivering intervention. This resulted in an estimate total of $4235 per family receiving professional intervention among the 18 families completing this treatment. Peers spent an estimated 1044 hours receiving training, being supervised, and delivering intervention to 24 families who completed treatment. Peers received 198 hours of training and supervision from professional trainers/supervisors. This resulted in estimates of $679 per family completing treatment delivered by peers.
Costs Associated with Professional- and Peer-Delivered Family-Based Pediatric Weight Management Treatment
Costs calculated by multiplying hours spent by average professional hourly wage ($61.88) which includes fringe (26.1%) and overhead (51%). Numbers may not add up perfectly due to rounding.
Includes family sessions and group sessions.
Includes travel time, other contact with families, etc.
Effects on Long-Term Weight Status of Delivering Peer Intervention
Among the parents from the first generation families in Parent Partnership who were peer interventionists (n = 4) to second generation families, there appeared better sustaining of one's own and one's child's weight status, relative to those who did not serve as peer interventionists. No statistical tests were conducted given the small sample size, but the strongest effects for being a peer seemed to occur while serving as a peer interventionist compared to the subsequent 6 months (i.e., 6-month to 1-year follow-up; Fig. 6).
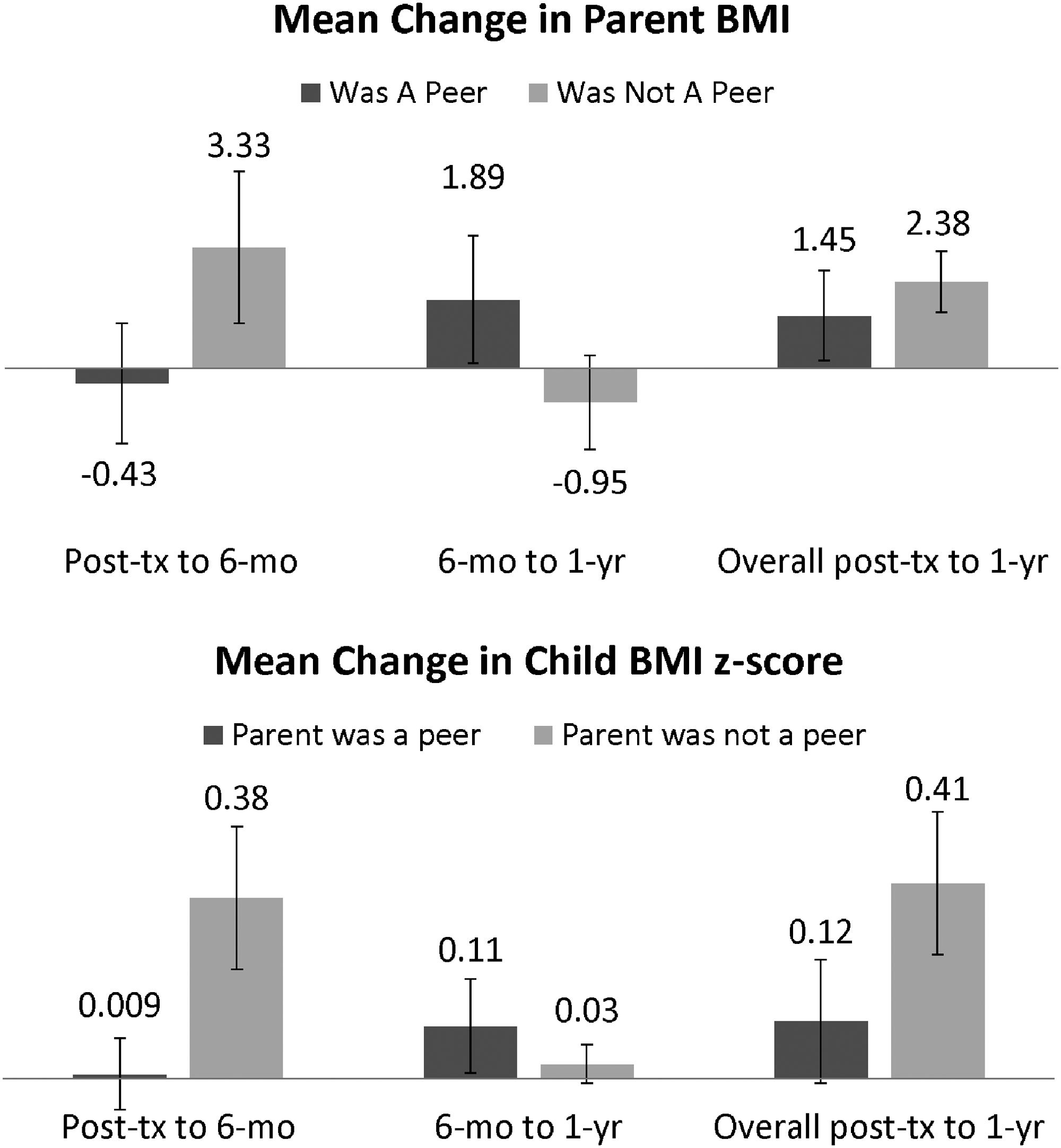
Descriptive change in child and parent relative weight status through follow-up among families whose parent served (n = 4) or did not serve (n = 4) as a peer interventionist to second generation families in Parent Partnership; no statistical testing done given small sample size (mean ± standard error).
Discussion
The EPICH and Parent Partnership trials suggest that parents previously treated within FBT may be able to subsequently provide acceptable and efficacious treatment to other families. However, given the pilot nature and sample size of these trials, findings should be interpreted cautiously and larger and more comprehensive examination of this and other peer models is warranted. Peer interventionists were highly engaged in receiving training and were thereafter confident in treatment delivery. Families receiving peer-delivered FBT rated treatment highly, mostly similar to professionally delivered FBT, and with no evidence of differential engagement in treatment. Treatment satisfaction ratings point to the potential need for some additional training in prescribed treatment-delivery behaviors and parent group delivery for peer interventionists.
The change from baseline to posttreatment in child and parent relative weight status through treatment was similar for families randomly assigned to receiving peer- versus professionally delivered treatment in EPICH. Both in EPICH and Parent Partnership, the average change in child relative weight status for those receiving peer-delivered treatment is consistent with effects reported for similarly intensive pediatric weight management interventions delivered by trained professionals. 13 Although a small sample, the second generation of Parent Partnership children and parents, who were all treated by peer interventionists, demonstrated some maintenance of their relative weight status changes 6 months after ending treatment.
Peer treatment delivery was estimated to be about 1/6th the cost to deliver than professional delivery. The majority of the peer delivery costs were the costs of training and supervision by professionals of peer interventionists. Furthermore, follow-up suggested that serving as a peer interventionist helped parents themselves and their children with better weight management, especially while parents were actively engaged in treatment delivery. There was some evidence of larger relapse thereafter to the 1-year follow-up relative to parents who were not peer interventionists and their children. Children whose parents did not become peers had unexpectedly higher average relapse in weight status over this follow-up relative to prior treatment interventions of similar length and follow-up. 21 These data in particular should be interpreted very cautiously given very small samples.
Numerous aspects of the peer intervention model used herein for FBT could have contributed to its preliminary success. As described by Simoni et al., 26 dynamic social impact theory and other social comparison theories postulate that the similarity between peers and those receiving treatment (i.e., peers and families they treat alike in that both are pursuing better weight management) helps to facilitate better uptake of and translation of information into behavior change. As expected, peer interventionists more often provided personal examples of their own behavior change strategies and successes for weight management with families to whom they were providing treatment than did professionals. Indeed, such examples provided by peers may more successfully change the perceived norms for such behaviors and parenting around children's eating and physical activity than any suggestions by professionals who themselves may not struggle with their own or their children's (if they have any) weight issues. It is noteworthy that many commercial weight management interventions rely on peer-based delivery. The treated parent-then-peer model for FBT may be among a variety of possible options for better engaging other nonprofessionals' help in family weight management and wellness. Most child-to-child interventions for healthy eating and physical activity have been school-based and not limited to children with overweight/obesity, demonstrating modest, if any, effects on child weight.27–31 Unlike some adult peer intervention models, in which training empowers and motivates adult peers to help other adults to engage in healthier behaviors, 32 the complexity of changing weight-related behaviors may make child-as-peer interventionist delivery difficult and more costly than peer interventions for other health behaviors. 33 On-going trials are examining the impact of the likely more tenable paraprofessional and other parent delivery models for childhood obesity prevention and treatment.34,35
The limitations of the present trials include small sample sizes, the English language-only treatment, the lack of an inert or waitlist or other control condition, and other factors that might affect broader generalizability (e.g., excluding those taking weight affecting medications). Furthermore, EPICH was likely biased from the self-selection of peers into this role from among a pool of parents who previously had received FBT. Some families could have self-selected out of participating in either present trial because of not being interested in being possibly treated by a nonprofessional or not enrolled in Parent Partnership because they were not willing to possibly be randomized to serve as a peer after receiving treatment. Also, these moderate to high income and mostly white samples may respond to receiving and providing peer intervention differently than other populations. However, peer-based interventionists may more readily be able to integrate cultural, regional, or other population-specific considerations than professionals. Finally, costs for maintaining a peer- versus professional-delivery model of intervention may start to converge as new peers each intervention generation would require similar levels of training and supervision, but the same professionals would likely need less training and supervision over time. Future research is warranted to more robustly examine peer intervention feasibility for pediatric weight management (e.g., what percentage of parents would be willing to deliver peer intervention?), acceptability, training and supervision needs of peers, efficacy equivalence to professional and other paraprofessional delivery models, model suitability and sustainability across different populations, and to comprehensively explore the impacts of serving as a peer interventionist.
Footnotes
Acknowledgments
Thank you to families participating in EPICH and Parent Partnership, both those receiving and delivering treatment. Research reported in this publication was supported, in part, by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under award number R21DK095676 (Parent Partnership trial) and by the Safeway Foundation (EPICH trial). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Safeway Foundation.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.