
Abstract
Abstract
Background:
Helicobacter pylori, one of the most common bacterial pathogens in humans, is generally acquired during childhood. The inverse correlation between H. pylori colonization and obesity that was found in adults has not been investigated in depth in children. Our aim was to assess the correlation between overweight and obesity and H. pylori colonization in a pediatric population.
Methods:
H. pylori colonization in 70 symptomatic children was determined after antral biopsies during esophagogastroduodenoscopy. Data on anthropometric measurements, sociodemographic characteristics, and medical history were recorded.
Results:
The participants' mean age was 12.41 ± 3.16 years, 58% were females, and 24% were obese or overweight (BMI >85th percentile). The H. pylori colonization rate was 31%. There were no significant differences between the H. pylori-infected and H. pylori-noninfected groups in terms of age, gender, or clinical and sociodemographic characteristics. Nevertheless, the prevalence of overweight and obesity was significantly lower in children with H. pylori colonization compared to children with normal histology (31% in the noninfected group compared to 11% in the infected group, p = 0.04). The mean fat percentage was 24.3 ± 8.8 and 19.4 ± 6.9, respectively (p = 0.02).
Conclusions:
The findings of this prospective study are in agreement with previous studies and demonstrate an inverse relationship between H. pylori colonization and overweight or obesity among symptomatic children. A larger prospective, multiethnic investigation is warranted to more definitively determine the extent of this association.
Introduction
Obesity has become a major public health problem of global significance. 1 The incidence of obesity in the general population has skyrocketed during the past 20 years, and more than doubled in children and quadrupled in adolescents in the past 30 years. For example, the percentage of children aged 6–11 years in the United States, who were obese, increased from 7% in 1980 to nearly 18% in 2012. Similarly, the percentage of adolescents aged 12–19 years, who were obese, increased from 5% to nearly 21% over the same period. 2 An increasing obesogenic lifestyle of excessive caloric intake and decreased physical activity is assumed to play a central role in this epidemiologic trend. Whether there are other environmental factors likely to explain the epidemic of obesity remains to be elucidated. 3
Helicobacter pylori, a gram-negative bacillus that is usually acquired during the first years of life, has an estimated prevalence of 50% and 80%–90% among adults in developed and developing countries, respectively. 4 Children who become infected with H. pylori are infected at a very young age, and although the rate of infection declines after 5 years of age, infection nevertheless continues until adulthood.5,6 H. pylori is known to be associated with the child's household size and socioeconomic status. 6 It is an established cause of gastritis, peptic ulcer, and gastric cancer. 7 Unlike adults, most infected children remain asymptomatic, 8 few infected children will develop chronic superficial gastritis, and a minority will develop duodenal ulcers in late childhood and adolescence.5,7–9 While the prevalence of overweight and obesity substantially increases in the Western world, the prevalence of H. pylori among children is decreasing regardless of standard of living and socioeconomic conditions.9,10
The relationship between H. pylori infection and body weight was addressed in numerous reports whose findings were inconsistent.1,11–16 Most,1,11–13 but not all,14,15 studies on children found that H. pylori infection are associated with a decreased risk for obesity and is negatively associated with ponderal growth. For example, a study by Wu et al. reported an inverse relationship between morbid obesity and H. pylori seropositivity in a Chinese population. The differences in the estimated risk of the presence of H. pylori in obese children were more pronounced in those aged 10–19 years (odds ratio [OR] 0.32, 95% confidence interval [CI], 0.10–1.00; p = 0.05) compared with adults aged >40 years (OR 0.58, 95% CI, 0.33–1.00; p = 0.05). 1 These findings suggest the possibility that the absence of H. pylori infection, especially during childhood, might increase the risk of later development of morbid obesity. 1 Vo et al. also showed that H. pylori infection is associated with decreased prevalence of obesity in a cohort of North American children. Due to its retrospective design, the only available data that characterized the socioeconomic status were the patients' health insurance status. 11
Many of the investigations for diagnosing the presence of H. pylori in children were based on serology, 1 urea breath testing (UBT13,15), or stool antigen assay. 14 While those measurements are available and inexpensive, their diagnostic accuracy is low. 7 Furthermore, due to the retrospective design of some of the studies, only limited data on the socioeconomic status of the patients were available, and none had been adjusted for socioeconomic status.11,13,15
We designed this prospective histopathology-based study to examine the prevalence of H. pylori in obese and normal-weight Mid-Eastern children and to test the hypothesis that the prevalence of obesity will be lower in H. pylori-infected children. Our prospective design allowed us to collect comprehensive data on socioeconomic status and medical history of the patients to further clarify the inverse association, if any, of BMI and H. pylori colonization.
Methods
We prospectively recruited children aged 5–18 years who were scheduled to undergo an esophagogastroduodenoscopy (EGD) between February 1, 2015 and January 31, 2016 at the Pediatric Gastroenterology Unit, Dana-Dwek Children's Hospital of the Tel Aviv Medical Center. These children were referred for EGD by their local pediatric gastroenterologists as part of the evaluation of their upper gastrointestinal symptoms. Excluded were children who had been diagnosed with H. pylori infection in the past and had received combined eradication treatment. The study protocol was approved by the institutional review board of the medical center.
Each participant or surrogate filled in a questionnaire after signing an informed consent. Data were collected on the child's age, sex, clinical parameters (pregnancy, delivery, prior hospitalizations, medications, and current symptoms) and socioeconomic parameters (marital status of the parents, number of rooms in the house, number of siblings, and number of people living in the house), and the parents' education and occupation. We examined the patient's anthropometrics (BMI, weight, height, lean body mass, and fat percentile) using a bioelectric impedance technique (Tanita BF 689, Tokyo, Japan).
All children or surrogates filled in a dietary 24-hour recall questionnaire to examine and compare mean caloric intakes. 17 The diet recall forms were an open-ended type, which listed only whether the meal was breakfast, lunch, or dinner. The interviewers instructed the participants to report all foods and beverages that had been consumed.
All the detected macroscopic abnormalities (erythema or nodularity) were documented during the EGD studies, and two biopsies were obtained from the antrum (lesser curvature) for the purpose of identifying suspected pathology. H. pylori was diagnosed by histopathologic identification of the organism with either hematoxylin and eosin stain or immunostaining.
Determination of the BMI percentiles for age and gender was based on WHO growth charts. “Overweight” was defined as a BMI >85th percentile and “obesity” was defined as a BMI >95th percentile. “Underweight” was defined as the 5th percentile of weight-for-height or weight-for-age. 18
Statistical analyses were performed using Minitab version 16 (Minitab, Inc., State College, PA). Continuous variables were reported either by means and standard deviations or by the median and the interquartile range. A univariate analysis was used to determine the relationships between each explanatory variable (H. pylori-positive compared to H. pylori-negative groups). The Pearson chi-square test was used to compare the groups with respect to categorical variables. The two-sample t-test was used to compare two groups with respect to variables that followed a normal distribution, and the two-sample Wilcoxon test was used to compare two groups with respect to variables that did not follow a normal distribution. Multivariate logistic regression was applied to data to identify the significant independent predictors of H. pylori positivity by considering candidate variables with p values <0.05 in the univariate analysis or if the variable was thought to be clinically relevant. A p-value below 0.05 was considered to be statistically significant.
Results
The characteristics of the 70 children who were recruited into this prospective study are presented in Table 1. Twenty-four percent of the entire cohort was obese or overweight, and none was underweight. The H. pylori colonization rate was 31% (22/70 patients), of which 81% were identified by means of hematoxylin and eosin stain and 18% were identified by immunostaining. All children colonized with H. pylori had chronic gastritis by biopsy. The baseline characteristics of the patients colonized with H. pylori and those with normal biopsies (H. pylori negative) are shown in Table 2. There were no significant differences between the two groups in terms of age, gender, and clinical and sociodemographic characteristics.
All Patients' Clinical Characteristics (n = 70)
Characteristics of H. pylori-Infected Compared to H. pylori-Noninfected Children
CS, cesarean section.
According to the dietary questionnaire, all children in this study were omnivorous, with a mean caloric intake of 2082 ± 572.17 kcal in the H. pylori-positive group and 2071 ± 764.9 kcal per day in the H. pylori-negative group (p = 0.95). Fifty percent of the diet was composed of carbohydrates in both groups, while 17% and 16% were composed of proteins and 33% and 34% were composed of fat in the H. pylori-positive and H. pylori-negative group, respectively.
Although the two groups were similar in all the above-mentioned parameters, the prevalence of obesity and overweight was 31% in the noncolonized children compared to only 9% among the colonized children (OR 0.22, 95% CI 0.05–1.00, p = 0.04; Fig. 1). The mean body fat percentage was 24.32 ± 8.83 in the former group compared with 19.43 ± 6.94 in the latter group (p = 0.02). Multivariate logistic regression corrected for age and gender revealed that being colonized with H. pylori was associated with an 80% reduction in the odds of being obese or overweight (OR −0.20; 95% CI 0.04–1.00; Table 3).
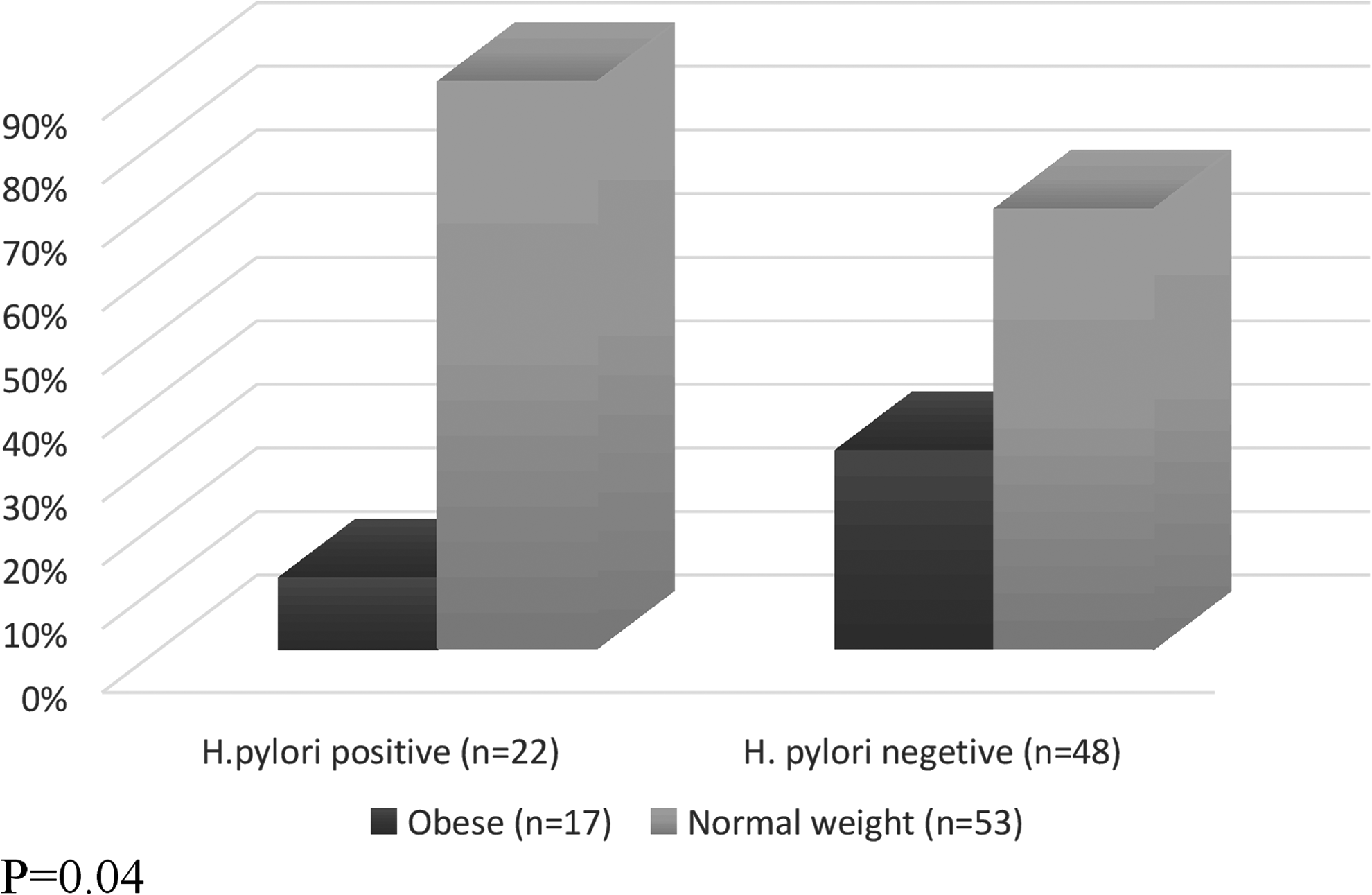
The proportion of obese or overweight patients compared to normal-weight patients in Helicobacter pylori-infected and Helicobacter pylori-noninfected children (p = 0.04).
The Association between BMI and H. pylori Colonization Using Multiple Logistic Regression Adjusted for Age and Gender
CI, confidence interval; OR, odds ratio.
Discussion
In this study, we found an inverse association between H. pylori colonization and prevalence of overweight or obesity in children. Our inclusion of a control group of symptomatic children from a similar socioeconomic background provided a broader picture of the impact of H. pylori on weight in a pediatric population. This work supports the findings of previous publications and is the first to demonstrate an inverse relationship between H. pylori infection and pediatric obesity in Mid-Eastern children, an observation that had been noted in Asian, European, and Afro/Caribbean American children.1,11,12
Most studies in pediatric populations that investigated the association between H. pylori infection and obesity in children were retrospective.1,13–15 One recognized limitation of retrospective studies is the lack of complete epidemiological data crucial for the analysis of H. pylori, which is known to be associated with living in crowded and low socioeconomic conditions. In this prospective study, data on socioeconomic status included the number of rooms and siblings, the academic education, and the marital status of the parents. Moreover, we examined other factors that might affect BMI or H. pylori colonization, such as the type of delivery and a history or not of breastfeeding. We found no significant differences between the H. pylori-infected and H. pylori-noninfected groups, except for the prevalence of overweight and obesity, thereby strengthening the inverse association between H. pylori colonization and obesity.
In this study, H. pylori colonization was determined as recommended in the clinical guidelines published by the H. pylori working groups of the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. 8 In addition, two antral biopsy samples were taken for every patient, a method that had been shown to be extremely sensitive for detecting H. pylori infection. 19 Interestingly, the prevalence of H. pylori in our cohort was lower than the value that was found in Israel 10 years ago in a study that examined growth indices among children of school age (up to 9 years) based on stool antigen. Fifty-three of those children were H. pylori positive at baseline (compared to 31% in our study), and the adjusted mean Z score of height for age at follow-up was significantly lower among the H. pylori-infected children than the uninfected ones, although no connection to ponderal growth had been found. 20 Differences in prevalence between those two studies can be secondary to different diagnostic procedures, differences in the population that had been examined, or improvement in standard of living and socioeconomic conditions during that time. The correlation to body weight that was found in our study as opposed to the study by Muhsen et al. 20 may be attributed to a decrease in the prevalence of H. pylori colonization. 21
Many potential explanations for this inverse correlation have already been published in the literature, the simplest one being that colonization produces an inflamed and sensitive gastric mucosa and the resulting postprandial pain decreases appetite, compromises caloric intake, and thus prevents obesity. 22 However, support for this hypothesis has been inconsistent. 15 We believe that this is the first investigation to include an attempt to collect data on caloric intake. In this study, all the children were symptomatic, had presented with abdominal pain, and had the same daily caloric intake, yet there were differences in the prevalence of obesity, thus indicating that it was not the pain alone that made the difference in obesity prevalence between the two groups. An alternative speculation, although not substantiated in this study, could be that H. pylori-induced gastritis may modulate the levels of gastric hormones that influence eating behavior, such as ghrelin.12,15,23
Another potential factor that needs to be considered is the gastrointestinal microbiome. Recent studies demonstrated a correlation between microbiomes and metabolism, obesity, and health. The gastrointestinal microbiome might be different in subjects with and without H. pylori infection. 24 Subjects with H. pylori infection may have been exposed to different species of bacteria compared to H. pylori-negative subjects and may consequently have a different gastrointestinal microbiome that can theoretically contribute to the development of obesity. 25 Fundamental changes in the microbiota, which occur at different ages, may possibly explain why H. pylori colonization influences metabolic parameters differently in children and adults.
Our study is limited by its relatively small cohort. An additional limitation is our use of a 24-hour dietary recall. While the 24-hour dietary recall is a frequently used tool for assessing nutrient intake, both overreporting and underreporting of the consumed foods limit the sensitivity of this tool for detecting changes in intake. 26 Further studies with more detailed questionnaires, such as the 3-Day or Food Frequency questionnaires, are needed to assess chronic obesity and differences in caloric intake in greater depth.
In conclusion, the results of this prospective study demonstrated an inverse relationship between biopsy-confirmed H. pylori colonization and overweight/obesity among symptomatic children from similar socioeconomic and geographic backgrounds. A larger, multiethnic prospective investigation is warranted to more definitively determine the extent of this association. There is also a need to further investigate the potential influence of H. pylori infection on stool microbiomes and caloric intake based on more longitudinal dietary/caloric information, as well as to identify the variables that lead to the apparent “protective” effect of H. pylori colonization upon body weight in childhood.
Footnotes
Acknowledgment
Esther Eshkol, the institutional medical and scientific editor, is thanked for editorial assistance.
Author Disclosure Statement
No competing financial interests exist.