
Abstract
Abstract
Background:
A number of research studies have demonstrated a decrease in health-related quality of life (HRQL) measures among obese children. Moreover, the causes of HRQL impairments are not completely clear. Adolescent obesity is oftentimes associated with other cardiometabolic risk factors (CRFs); hence, the aim of our research was to estimate the frequency of CRFs and to determine whether there is an association between CRFs and HRQL scores among obese adolescents.
Methods:
Our research included 92 treatment-seeking obese adolescents (11–17 years), 34 males. We looked at medical records and performed physical examinations, including anthropometry and laboratory evaluations. PedsQL™ 4.0 was used to assess the HRQL score. Logistic regression models were used to identify CRFs associated with worse HRQL scores, both in total and in each domain.
Results:
The vast majority (70.6%) of adolescents had at least one CRF in addition to obesity. A cluster of three to four CRFs was found in 23.3% and was associated with males more than with the degree of obesity [odds ratio (OR) 4; confidence interval (95% CI) 1.3–11.6, p = 0.01]. HRQL scores in emotional functioning domain and scores of HRQL total were directly associated with waist circumference Z-score (OR 4.1; 95% CI 1.1–14.9, p = 0.03 and OR 3.4; 95% CI 1–11.6, p = 0.049). Hypertension was associated with worsening HRQL scores in school functioning domain (OR 3.3; 95% CI 1–10.9, p = 0.049).
Conclusion:
Obesity in adolescents is associated with a high frequency of associated CRFs and decreased HRQL scores. Although CRFs have an influence on reducing adolescents' HRQL, they are not a determining factor.
Introduction
The obesity epidemic is a global problem. From 1980 to 2013, the global prevalence of overweight and obesity increased by 27.5% in adults and 47.1% in children. 1 Moreover, according to the results of an epidemiological survey conducted in Russia, there were 19.9% of overweight children and 5% of obese children. 2
Children diagnosed as overweight have been well tracked into adulthood. 3 An overweight diagnosis in childhood has been shown to significantly contribute to the development of cardiovascular, gastrointestinal, and skeletal disorders, type 2 diabetes, obstructive sleep apnea syndrome, and some types of cancer.4,5 Moreover, obesity during adolescence is oftentimes associated with psychological problems. For example, an association has been found between adolescent obesity and depression. 6 The health-related quality of life (HRQL) is among one of the psychosocial instruments used to assess physical and psychosocial well-being. 4
HRQL is a comprehensive multidimensional construct encompassing physical and psychosocial well-being. 7 Previous studies have shown that obese and overweight children have significantly lower HRQL scores, compared with lean children in clinical and in community-based samples.8–13 It has also been shown that HRQL scores in children diagnosed as overweight and obese are comparable to that of children with inflammatory bowel diseases, 14 and in severely obese children and adolescents HRQL scores are comparable with those having received cancer treatment. 15
In the last decade, there has been increasing interest in the investigation of factors associated with decreased HRQL scores in children with obesity. Outcome data are essential for the development of programs which address the treatment and prevention of obesity in this age group. It has been shown that worsening HRQL scores in children with obesity have been associated with increased screen time, as well as a lessened level and pattern of physical activity.16–18 Evidence points to a strong association between worsening HRQL scores and symptoms of depression in children and youth with obesity. 19 In addition, there is evidence that HRQL scores differ based on gender among obese children. The majority of studies demonstrate a connection between lower HRQL scores in obese females.11,20,21 However, other authors have found worsening HRQL scores among males 22 or the absence of any significant gender influence on HRQL scores. 9
Obesity in adolescence is associated with cardiometabolic risk factors (CRFs), such as hypertension and disorders in carbohydrate and lipid metabolism.23,24 Therefore, we can assume that CRFs influence HRQL scores in adolescents, for example, through pathophysiological mechanisms involving emotions. At the same time there are very few existing studies which have investigated the relationship between CRFs and HRQL scores among obese adolescents. Moreover, those that do exist tend to include patients with severe obesity21,24–26 and/or the results presented are contradictory. There are almost no studies which examine the relationship between CRFs and HRQL scores in nonselective samplings, including adolescents with different degrees of obesity.
Undoubtedly, the problem warrants further investigation; hence, the aim of our research was to determine the estimated frequency of CRF and its association(s) with HRQL total scores and HRQL scores in each domain in a nonselective sample of adolescents of different genders within a cohort of Russian adolescents diagnosed with obesity.
This information is important, as it will provide further insights into the physical and mental health risks, as well as associated factors among obese and overweight children.
Methods
Participants
We conducted an observational cross-sectional study. Participants were recruited from a sample of adolescent children between the ages of 11 and 17, identified as having been diagnosed as obese, and hence referred to the Pediatric Unit Clinic of the Scientific Centre for Family Health and Human Reproduction Problems (Irkutsk, Russia).
Inclusion criteria were as follows: (1) 11–17 years of age; (2) a BMI ≥95 percentile for relevant age and sex 27 ; and (3) evidence of a written informed consent from parents/primary caregivers and participants.
Exclusion criteria were as follows: (1) presence of an acute or chronic disease other than obesity that could affect the HRQL score of the patient; (2) a documented and/or determined genetic, for example, Prader–Willi syndrome and secondary condition(s), for example, Cushing syndrome, hypothyroidism, and so on causes of obesity; (3) marked cognitive impairment; (4) documented/discovered use of drugs which influence emotions; and (5) participation in a weight control, weight-loss, or weight management program.
Upon study enrollment, during their initial study visit, a medical history, physical examination, and laboratory evaluation(s) were performed. At the end of the initial study visit, a follow-up visit was scheduled for each adolescent. During the follow-up visit, each study participant completed a questionnaire to estimate his/her HRQL score. At the close of the follow-up visit, the physician provided recommendations on how to lose weight.
The total participant study duration was ∼4 days.
Measurements
A qualified pediatrician took anthropometric measurements in the morning. Adolescents were lightly dressed and wore no shoes. Weight and height were measured using a stadiometer and an electronic scale. BMI was calculated from height and weight, and BMI Z-scores and percentiles were calculated to standardize BMI measurements for age and sex. 27 Waist circumference (WC) was measured with a nonflexible measuring tape during minimal respiration, at the midpoint between the lowest rib and the iliac crest to the nearest 0.1 cm. Abdominal obesity was diagnosed when WC was ≥95 percentile for this sex, height, and age. 28
Systolic blood pressure and diastolic blood pressure were measured with an automated blood pressure monitor (Omron Healthcare Co., Ltd, Japan) thrice using appropriate cuff size after the patient was sitting for 10 minutes. BP estimation was made using sex and height percentile-based tables and recorded on the fourth report upon diagnosis, evaluation, and treatment of high BP in children and adolescents. 29
Laboratory Tests
Blood samples were obtained after an overnight fast to measure lipid spectrum, glucose, insulin, and liver transaminases: alanine aminotransferase (ALT) and aspartate aminotransferase (AST). Homeostasis model assessment for insulin resistance (HOMA-IR) was calculated using the following formula: fasting plasma insulin (μU/L) × fasting glucose (mmol/L)/22.5. Insulin resistance was determined using the following recommended cutoff points for participants in the pubertal stage: 5.22 in males and 3.82 in females. 30
To determine glucose tolerance, participants were given oral glucose doses in the amount of 1.75 g/kg body weight (up to a maximum of 75 g). Glucose levels were measured and documented at 0 and 120 minutes.
When estimating thresholds of lipid and glucose levels we followed criterion ascribed for children and adolescents as set forth by the International Diabetes Federation (2007). Total cholesterol was considered increased when serum concentrations were ≥5.20 mmol/L, triglycerides ≥1.70 mmol/L, high-density lipoprotein (HDL) cholesterol <1.03 mmol/L, low-density lipoprotein (LDL) cholesterol ≥3.36 mmol/L, and fasting glucose ≥5.60 mmol/L. 31
Measurement of HRQL
The Paediatric Quality of Life Inventory (PedsQL™ 4.0, Lyon, France) was used in the present study, with the Russian Generic Version. Total self-reporting scale scores for children 8–12 and 13–18 years of age have been demonstrated to exceed a Cronbach α reliability coefficient of 0.90. For physical functioning subscale scores and the psychosocial health summary scores were greater than 0.8. The emotional, social, and school functioning subscale scores had the lowest reliability coefficients of all the HRQL inventory scores, although in general they exceeded the minimum 0.70 recommendation for group analysis. 32
PedsQL measures a multidimensional construct and includes a 23-itemized survey instrument composed of four domains. The four domains assessed include physical, emotional, social, and school performance. From the calculated domain score, a total score was calculated. Items were linearly transformed to a 0 to 100 scale, so that the higher the score, the better the HRQL.
For the purposes of this study, and in an effort to assess HRQL scores, we relied on self-reported measures.
Ethical Considerations
The study was performed according to the Declaration of Helsinki (II) and followed guidelines for the ethical conduct of medical research involving children. The study protocol has been approved by the Ethics Committee Federal State Public Scientific Institution, Scientific Centre for Family Health and Reproduction Problems.
Statistics
Statistical data analysis was conducted utilizing the program package STATISTICA 12.5 (StatSoft, Inc.). The Mann–Whitney U test was used to assess differences between genders in continuous variables. The chi-square test was used to assess differences among discrete variables, for example, differences in hypertension, dyslipidemia, impaired fasting glucose between subgroups, and so on. We calculated the Spearman correlation coefficient to examine connections between quantitative variables. To compare HRQL scores in adolescents within our study to HRQL scores within a community-based sample of Russian adolescents, we estimated whether published community-based mean values included 95% confidence intervals (CIs) calculated for scoring total HRQL and HRQL in each domain of our sample. 33 A logistic regression analysis was used to estimate associations between HRQL total score and within each domain score with characteristics of obesity (BMI Z-score and WC Z-score), each of the CRFs (hypertension, dyslipidemia, and impaired fasting glycemia and/or after glucose loading), and clustering of three to four CRFs [metabolic syndrome (MetS) 31 ]. Because there is no reference range for HRQL scoring, we dichotomized scores of total HRQL and in each of the domains, relevant to values of 25 percentiles, and characterized HRQL scores as worsening when scores fell below this point. All regression models were adjusted by sex and age. A p-value below 0.05 was considered statistically significant.
Results
A total of 92 adolescents diagnosed as obese between 11 and 17 years of age were included in our study. The group consisted of 34 boys and 58 girls. Thirty-two (34.8%) patients were documented as severe obesity (BMI Z-score ≥3). Sixty-nine adolescents (75%) were diagnosed with abdominal obesity. Sixty-five (70.6%) obese adolescents had at least one CRF (in addition to obesity): hypertension [n = 44 (47.8%)] with significant prevalence in boys (χ2 = 25.8; p = 0.0001); impaired glucose metabolism [n = 28 (30.4%)]; and dyslipidemia [n = 21 (22.8%)]. Dyslipidemia was characterized by a decrease in HDL cholesterol levels (13%) and an increase in triglycerides (10.9%) and plasma LDL cholesterol (4.3%) levels. Insulin resistance was found in 50 (54.4%) adolescents. Hepatic steatosis was diagnosed in 16 (17.4%) adolescents. We found that a cluster of three to four CRFs corresponded to MetS in 19 (20.6%) adolescents. More often than in females, such CRF clustering was found in males (χ2 = 7.1; p = 0.008).
General study group characteristics, as well as separate gender-based characteristics for males and females, are shown in Table 1. In Table 2 there are significant correlations between the characteristics of the participants and proxies of obesity (BMI Z-score and WC Z-score), concluded from the mono-factor analysis. We discovered that males had more significant correlations of BMI and WC Z-scores with parameters characterizing cardiometabolic risk in comparison with females.
Characteristics of Adolescents and Health-Related Quality of Life Scores by Sex
Data are presented as mean ± SD or median (interquartile range).
ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBP, diastolic blood pressure; HDL, high-density lipoprotein; HOMA-IR, Homeostasis model assessment for insulin resistance; HRQL, health-related quality of life; LDL, low-density lipoprotein; MBP, mean blood pressure; OGTT, oral glucose tolerance test; SBP, Systolic blood pressure; WC, waist circumference.
Significant Correlations between the Characteristics of the Participants and the Degree of Obesity
r = Spearman's correlation coefficients.
HRQL total scores, as well as scores of each domain, were compatible in obese adolescents of both sexes and significantly decreased compared to the large community-based sampling of Russian adolescents matched by age mainly in the physical functioning domain (Fig. 1). 33
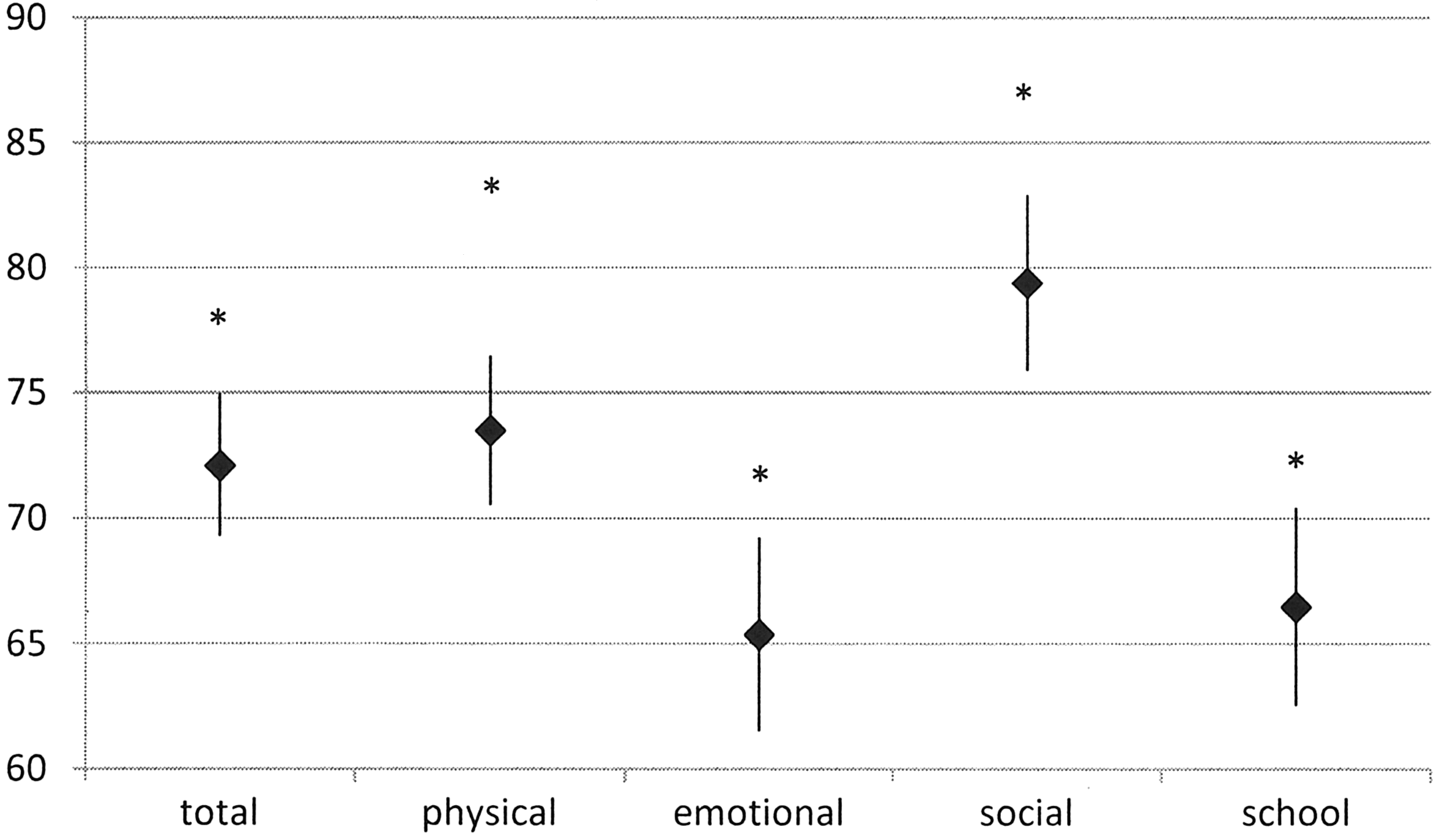
HRQL scores in adolescents with obesity compared to in population. *Common population mean values (adapted from published data 33 ). ♦Mean values for the group of adolescents with obesity, with 95% confidence intervals. HRQL, health-related quality of life.
Our logistic regression analysis demonstrated that regardless of the presence of any CRF, female sex was associated with lower HRQL scores in the physical functioning domain [odds ratio (OR) 3.1; 95% CI 1.03–9.5, p = 0.04]. We did not show independent predictive significance in the degree of obesity, fat distribution, presence of any CRF, and MetS for HRQL scores in the physical functioning domain (Table 3).
Adjusted Odd Ratios (95% Confidence Interval) for Having a Poor Score on Each Domain of Health-Related Quality of Life According to Cardiometabolic Risk Factors
p < 0.05.
Bold indicates significant associations.
EF, emotional functioning; PH, physical functioning; ScF, school functioning; SF, social functioning.
HRQL scores in the emotional functioning domain and HRQL total scores did not depend on sex, age, or degree of obesity; however, they were associated with WC Z-score. The presence of CRFs and MetS was not associated with a worsening total HRQL score or emotional domain.
HRQL scores in the social domain did not have significant associations with the proxy of obesity and CRFs.
For the scores in the school functioning domain, we did not find any association between obesity characteristics; however, hypertension in adolescents was significantly associated with a worsening HRQL score in this domain.
Discussion
We demonstrated that 70.6% of all participants had at least one CRF in addition to being obese. The most common CRF was hypertension. Lipid and carbohydrate metabolism disorders were diagnosed less often.
The prevalence of CRFs among obese adolescents has been shown in other research studies.23–25,34,35 Lafortuna et al. found similar results as our sample—obese adolescents were diagnosed at a higher frequency with hypertension. 34 It is worth noting that wherein other surveys have found a diagnosis of dyslipidemia more often in obese adolescents, the frequency of hypertension diagnosis was consistent with that of our survey.24,25 The higher frequency of dyslipidemia diagnosis as observed in the aforementioned research studies may possibly be connected to the inclusion of adolescents with severe obesity, whereas our sample mainly included adolescents diagnosed with a moderate degree of obesity. It is also worth noting that the percentage of obese adolescents among our study population that also had at least one CRF (in addition to obesity) was comparable with the selective samples of adolescents with severe obesity, indicated by the study results of other researchers.24,25 This indicates that any degree of obesity can be characterized by an elevated risk of cardiometabolic complications.
A cluster of CRFs, responding to MetS, was found in 20.6% of our sample adolescents, which is compatible with the frequency evidenced in previously published research.24,25,34 However, CRF clustering was associated with male sex more than the degree of obesity (OR 4; 95% CI 1.3–11.6, p = 0.01) because males were diagnosed with hypertension more often than females, whereas the frequency of dyslipidemia and impaired glucose levels in males was consistent. The high frequency of hypertension in male adolescents compared to female adolescents was demonstrated by Zeller et al. among a group of adolescents with severe obesity 25 —this finding has also been replicated in community-based studies. 36 A possible explanation for this could lie in elevated levels of testosterone found in adolescent boys. It was shown that a functional variant in the androgen receptor gene, which mediates androgenic effects of testosterone, has been associated not only with higher levels of visceral fat but also with higher sympathetic vasomotor tone and BP in adolescent males but not females. 37
HRQL scores in our sample of treatment-seeking obese adolescents were significantly lower than the one in the Russian community-based sample. 33 This finding was consistent in both HRQL total scores and HRQL in all domains. Emotional and school domains appeared to be the most vulnerable, which has since been confirmed by other research studies.19,38,39 Lower scores in the physical domain were associated with the female sex and remained consistent with the results evidenced by earlier studies,26,40–43 but HRQL total scores, as well as scores in other HRQL domains, did not show a dependence on sex.
By studying associations of CRFs with HRQL scores, we showed that the BMI Z-score significantly influences neither HRQL total score nor any of the domains while the degree of abdominal obesity was an independent predictor of worsening HRQL total scores with the worst scores in the emotional domain, regardless of adolescent sex and age.
With regard to the influence of the degree of obesity on HRQL scores, the literature gives contradictory results. In several studies, including ours, links between BMI Z- and HRQL scores in children with obesity were not shown,19,24 but in other studies, associations were demonstrated. The majority of the surveys report weak negative associations between BMI Z- and HRQL scores in the physical and social PedsQL domains.15,38,44 One study showed a negative relationship between BMI Z- and HRQL scores in all five domains of the PedsQL. 8 In another study, it was determined that a greater degree of obesity was associated with lower scores on the subscales Moods and Emotions and Self-Perception. 45
These contradictions could plausibly be explained by the peculiarities in which study populations were formed and various ranges of BMI Z-score in each. In studies verifying the existence of significant associations between BMI Z- and HRQL scores, both patients with obesity and children with normal weight were included.8,15,44 Surveys such as ours, which do not corroborate such associations, were conducted with homogeneous clinical samples, including only children with excess weight, that is, ≥95 percentiles.19,24 Along with this, there are studies conducted in a cohort of children with obesity and that corroborated the negative relationship between HRQL scores and BMI Z-score,26,42,45 in one of which obesity-specific instrument for HRQL assessment was used. 26
Riazi et al. showed interesting results in their study in which the association between BMI Z- and HRQL scores was studied first for the total sample, including both obese and nonoverweight children, and then included samples of only obese children. They demonstrated that in the total sample, BMI Z-score was significantly associated with all PedsQL subscales except school functioning. However, in the obese group, BMI Z-scores were not significantly associated with any of the PedsQL subscales. 39 These results argue for the theory that the disappearance of the relationship between the degree of obesity and HRQL scores in samples of obese children could be attributed to the narrowness of BMI Z-score value range.
There are few research studies currently available which estimate associations between WC and HRQL scores' among children and adolescents.
Radhakishun et al., demonstrated that lower scores on the subscale for physical well-being were significantly associated with higher WC. 45 However, according to the results of a community-based survey conducted in Germany, central obesity in primary school aged children was inversely associated with HRQL total scores and also with scores in the domains of psychological well-being, family, and friend(s), but not in the domain of physical well-being. 46 However, our research has shown a significant association between the degree of abdominal obesity and worsening emotional functioning scores. This conclusion is further substantiated by the literature, in which an association between visceral fat and disorders in emotional spheres has been reported.19,47 In the study conducted by Aparicio et al., resultant data demonstrate that emotional psychopathology in preadolescence is associated with increased weight gain and abdominal fat in adolescence. 47 There are two plausible rationales which explain this association: (1) emotional disorders are often accompanied by binge eating and (2) the conceivable presence of a shared neurobiological mechanism between emotional psychopathology and obesity. Emotional psychopathology affects the hypothalamic–pituitary–adrenal axis, leading to increased cortisol secretion. High cortisol levels are associated with obesity, especially abdominal obesity. Dysregulation of the central serotonin, norepinephrine, and dopamine neurotransmitter systems and elevated leptin can play a definite role. 48
We, as well as the majority of researchers, did not find any association between the degree of obesity and HRQL score in school functioning.19,24,26 Presence of this association, although weak, was shown only in one research study. 44 Of noteworthy mentioning—throughout the course of our investigation, regardless of the degree of obesity, the worst HRQL scores in school functioning were associated with hypertension. Possibly, this association was determined by hypertension conjugation with chronic drug intake and feeling unwell, which could consequently affect class attendance and cause the need to visit specialists more regularly as to control effectiveness and safety of treatment.
Conclusion
Our study indicates that there is a strong association between obesity and CRFs in a nonselective sample of treatment-seeking obese adolescents. Moreover, we demonstrated a high disposition to clustering and interdetermination of different risk factors in male adolescents, but we did not find gender differences in either total HRQL scores or in any of the domains. We also demonstrated that the presence of CRFs can possibly contribute to a reduction or worsening in the HRQL scores among obese children—worsening HRQL total and emotional functioning were associated with the degree of abdominal obesity and depressed school functioning with comorbid hypertension—but they do not determine it.
Limitations
This study has some limitations. First, this is a cross-sectional analysis therefore assumptions about causality cannot be made. Second, this investigation was conducted among Caucasian, treatment-seeking obese adolescents; therefore, results cannot be extrapolated on all obese adolescents. One other limiting factor of this study includes the lack of consideration of social and psychological characteristics of adolescents. We did not consider these domains when drawing inferences about associations between HRQL scores and CRFs.
The absence of reference range for HRQL scores also imposes some limitations. Finally, in assessing HRQL scores, we used a general inquirer; perhaps had we utilized a specific instrument (e.g., instrument IWQOL-Kids© 49 or Sizing Me Up©50,51), we could have uncovered more significant associations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.