
Abstract
Abstract
Background:
A short sleep duration is associated with a higher obesity risk from midchildhood onward. However, whether sleep duration in early childhood is associated with body composition and cardiometabolic health remains unclear. This study aims to examine the prospective association of sleep duration in infancy and early childhood with body composition and cardiometabolic health at 6 years of age.
Methods:
Data were available for 5161 children from a population-based cohort in the Netherlands. Sleep duration was assessed at ages 2, 6, 24, and 36 months by parental reports. When children were 6 years old, measures of body composition (iDXA), blood pressure, insulin, and lipid levels were collected. Longitudinal associations among sleep duration, body composition, and cardiometabolic health were studied with multivariable linear regression analyses. In addition, potential bidirectional associations between sleep duration and BMI were studied by using cross-lagged modeling.
Results:
Shorter sleep duration at 2 months predicted higher BMI and fat mass in 6-year-old children, accounting for confounders and BMI at 2 months (e.g., for BMI, per hour sleep, B = −0.018, 95% CI = −0.026; −0.009). No temporal relationships among sleep duration at other ages, later body composition, and cardiometabolic outcomes were found. The cross-lagged model indicated a bidirectional association between sleep duration and BMI in early life (2 to 6 months of age).
Conclusions:
Shorter sleep duration at 2 months, but not at later ages, predicted poorer body composition 6 years later. We found no clear evidence for an effect of sleep duration in early life on cardiometabolic health.
Introduction
Obesity researchers have expanded their focus to a broad spectrum of potentially modifiable factors—including the role of sleep—to restrain the obesity epidemic. 1 An association between short sleep duration and overweight in children has been indicated by several reviews, including both cross-sectional studies2,3 and longitudinal research. 4 However, most of these studies were performed in school-aged children, whereas the role of sleep duration at younger ages remains uncertain. Four longitudinal studies reported an association between shorter sleep duration in early childhood and higher BMI in midchildhood,5–8 whereas two studies found no association.9,10 Furthermore, while it is suggested that sleep affects metabolism, reversed causality cannot be fully ruled out yet, as it has hardly been examined. Another knowledge gap relates to the assumption that shorter sleep is associated with a higher BMI due to increases in fat mass. 11 However, only a few studies disentangled the different components of body composition. Taveras et al. showed an association among sleep duration at 6 months, BMI, and skinfold thickness at 3 years. 12 Moreover, Carter et al. observed a relationship of sleep with fat mass but not fat-free mass in children aged 3 to 7 years old, while Baird et al. reported an association with both fat mass and fat-free mass in children aged 3 to 4 years.11,13
Recently, sleep duration has also been studied in the context of cardiometabolic risk factors other than obesity in children. Research showed an association between short sleep duration and increased glucose concentrations or reduced insulin sensitivity,14–17 but this was not always replicated. 18 In addition, children who slept less had increased cholesterol concentrations,18,19 but again, results were inconsistent and associations with triglycerides were not found.17,20 Moreover, most studies had a cross-sectional design, making it difficult to infer a temporal relationship.
Using data from a large population-based prospective study in the Netherlands, we examined the longitudinal association of sleep duration at four timepoints in infancy and early childhood (i.e., from 2 to 36 months) with body composition and cardiometabolic health at the age of 6 years. Furthermore, the relationship between sleep duration and BMI was studied during early childhood with cross-lagged modeling to determine directionality of the association.
Materials and Methods
Study Population
This study was embedded in Generation R, a population-based, prospective cohort from fetal life onward. 21 All pregnant women with an expected delivery date between April 2002 and January 2006 living in Rotterdam, the Netherlands, were invited to participate (participation rate: 61%). Written informed consent was obtained from all participants, and the study was approved by the Medical Ethical Committee of the Erasmus Medical Center, Rotterdam.
Information on sleep duration at any timepoint was available for 6565 children (for 2220 children, sleep duration was available at all four timepoints). Of these children, 78.6% (n = 5161) participated in the follow-up study at the research center, where measurements on body composition and cardiometabolic outcomes were assessed. Blood samples were available in fewer participants reflecting lower consent rates for venous puncture (n = 3495). In the analyses, the study population varied due to missing data on determinants or outcomes (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/chi).
Of the 6565 children with at least one assessment of sleep duration, 1404 children had missing data on all outcomes. These children (n = 1404) were more often of non-Dutch origin (p < 0.001) and had lower educated mothers (p < 0.001). There were no differences in birth weight (p = 0.32) or maternal BMI (p = 0.96).
Measures
Sleep duration
Sleep duration was assessed by questionnaires filled out by the parents at four different timepoints during infancy and early childhood, that is, when the children were 2, 6, 24, and 36 months of age. Parents were asked to write down the usual bedtimes and wake times of their child at that moment. Daytime sleep was assessed categorically with answering options ranging from <30 minutes to >2.5 hours. For each timepoint, sleep duration was calculated as hours of sleep per 24 hours by adding nighttime and daytime sleep.
Body composition
At the age of 2, 6, 24, 36, and 48 months, child growth characteristics were obtained at the Municipal Child Health Centers, where trained staff measured children's height and weight by standard procedures. At the age of 6 years, children were invited to our research center for detailed measurements. Height and weight were measured without shoes and heavy clothing. Height was measured by a stadiometer (Holtain Limited, Crosswell, Crymych, United Kingdom) to the nearest 0.1 cm. Weight was measured to the nearest 0.1 kg using an electronic scale (Seca 888; Almere, The Netherlands). BMI (kg/m2) standard deviation (SD) scores were calculated by adjusting BMI for age and sex of the child using the Dutch reference growth curves (www.growthanalyser.org). 22 Body composition was measured by a dual energy X-ray absorptiometry (iDXA, 2008; GE-Lunar, Madison, WI). Children were positioned in horizontal position on the table without shoes, heavy clothing, and metal objects. Fat mass index (FMI) was calculated as total fat mass/length (kg/m2) and fat-free mass index (FFMI) as total fat-free mass/length (kg/m2). FMI and FFMI were transformed into sex- and age-specific SD scores, calculated by internal standardization with the residual method in all participating children who had measures of body composition available.
Cardiometabolic health
At the age of 6 years, systolic- and diastolic blood pressure were measured four times with one-minute intervals at the right brachial artery using the automatic sphygmomanometer Datascope Accutor Plus™ (Paramus, NJ). While measuring blood pressure, children were lying supine. For each child, the mean value of the last three measurements was calculated to determine systolic- and diastolic blood pressure. Thirty minute fasting blood samples were collected to measure total cholesterol, high-density lipoprotein (HDL)-cholesterol, triglycerides, and insulin concentrations, using Cobas 8000 analyzer (Roche, Almere, the Netherlands). Intra- and interassay coefficients of variation in quality control samples ranged from 0.77% to 1.39% and 0.87% to 2.40%, respectively.
Covariates
Information on sex and birth weight of the children was obtained from medical records. Children's age at outcome assessment was derived from the date they visited the research center. Child ethnicity was based on the country of birth of the parents, which was assessed by prenatal questionnaire. In the same questionnaire, information on maternal educational level and maternal psychopathology symptoms was obtained. Maternal psychopathology symptoms were assessed during the first trimester of pregnancy with the Brief Symptom Inventory (BSI). The BSI is a validated 53-item questionnaire assessing a broad spectrum of psychopathology, including depression, somatization, anxiety, and psychotic symptoms. 23 Postnatal parental questionnaires were used to assess duration of breastfeeding (in months) and duration of television watching (in hours, at age 36 months). Height and weight measurements in early pregnancy (<14 weeks of pregnancy) were used to calculate maternal BMI.
Statistical Analyses
Correlations between sleep duration and metabolic risk factors were tested using Pearson and Spearman rank correlation techniques. Associations among sleep duration at four different timepoints, body composition, and cardiometabolic health at 6 years were examined by multiple linear regressions. Analyses were first adjusted for age and sex and in a second step for confounders that changed the effect estimates by 5% or more. To examine the temporal relationship, analyses with body composition were additionally adjusted for BMI at the age sleep duration was measured, when model 2 was significant. Baseline BMI was used as a proxy for FMI and FFMI, since FMI and FFMI were not measured before 6 years of age.
Finally, a cross-lagged modeling approach was used to examine the possible bidirectional association between sleep duration and BMI from infancy to 6 years of age. To establish this, we included all sleep duration timepoints (at age 2, 6, 24, and 36 months) and BMI measurements at the same timepoints, as well as at age 48 months and 6 years in one model. First, wave-on-wave associations within each of the two key variables (stability paths) and cross-sectional relationships between the sleep assessments and the BMI assessments were included in the model, with confounders regressed on the baseline assessments of sleep duration and BMI at 2 months of age. Next, we included lagged associations from each sleep duration assessment to all following waves of BMI assessments and in the opposite direction, lagged associations from each BMI assessment to all following waves of sleep duration assessments. This way, the cross-lagged model estimates the relationship between sleep duration and BMI in both directions over time, while accounting for the continuity of sleep duration and BMI over time and the cross-sectional associations at each timepoint.
Insulin and triglycerides were non-normally distributed and, therefore, square-root transformed. Standardized scores for cardiometabolic outcomes were used to improve comparability between effect estimates. Missing values of covariates ranged between 0.5% for birth weight and 22.8% for maternal psychopathology symptoms and were estimated using multiple imputation techniques. Pooled results of 20 imputed datasets were reported. All statistical analyses were performed using SPSS 21.0, except for the cross-lagged analysis, which was conducted in Mplus version 7.11.
Results
Child and maternal characteristics are shown in Table 1. At the age of 2 months, children slept on average 14.7 hours (SD = 3.0) per 24 hours. This decreased to a mean sleep duration of 12.6 hours (SD = 1.1) per day at age 36 months. Most children were of Dutch origin (62.4%), and most mothers were highly educated, with higher vocational education or university education (53.2%). Correlation coefficients among sleep, body composition, and cardiometabolic outcomes are shown in Supplementary Table S1.
Child and Maternal Characteristics
Values represent mean (SD), medians (IQR) or percentage of subjects, derived from the unimputed dataset.
FFMI, fat-free mass index; FMI, fat mass index; HDL, high-density lipoprotein; IQR, interquartile range; SD, standard deviation.
Table 2 presents the associations of sleep duration with body composition at 6 years of age. After adjustment for covariates, shorter sleep duration at 2, 24, and 36 months was associated with a higher BMI SD score at age 6 years (per hour sleep at 2 months, B = −0.015, 95% CI = −0.024 to −0.007), but there was no association between sleep duration at 6 months and BMI SD score. Adjusted for BMI at the same age as sleep duration, only sleep duration at 2 months of age remained associated with a higher BMI at 6 years of age (per hour sleep, B = −0.018, 95% CI = −0.026 to −0.009).
Associations of Sleep Duration at Different Timepoints with Body Composition at 6 Years
Values are linear regression coefficients (95% CI). Model 1 is unadjusted and model 2 is adjusted for ethnicity, birth weight, duration of television watching, duration of breastfeeding, maternal educational level, maternal BMI, and maternal psychopathology symptoms. Model 3 is additionally adjusted for baseline BMI SD score, when Model 2 showed a significant association.
p < 0.05.
p < 0.01.
p < 0.001.
CI, confidence interval; NA, not applicable; FFMI, fat-free mass index; SD, standard deviation.
Adjusted for covariates, short sleep duration at 2 months was associated with higher fat mass at 6 years of age (per hour sleep, B = −0.012, 95% CI = −0.020 to −0.003), whereas shorter sleep duration at 24 and 36 months was associated with a higher fat-free mass. After including BMI at the same age of sleep duration in the model, shorter sleep duration at 2 months remained associated with higher fat mass at 6 years (per hour sleep, B = −0.013, 95% CI = −0.022 to −0.044), but the associations of sleep duration at 24 months and 36 with fat-free mass attenuated to nonsignificance.
Figure 1 shows the significant pathways from the cross-lagged model. Both sleep duration and BMI showed moderate to high consistency between subsequent assessments. The longitudinal pathways indicated that a shorter sleep duration at age 2 months predicted a higher BMI at ages 6 months and 6 years. Reverse associations were also found: a higher BMI at 2 months predicted shorter sleep duration at 6 months, and a higher BMI at 24 months predicted shorter sleep duration at 36 months.
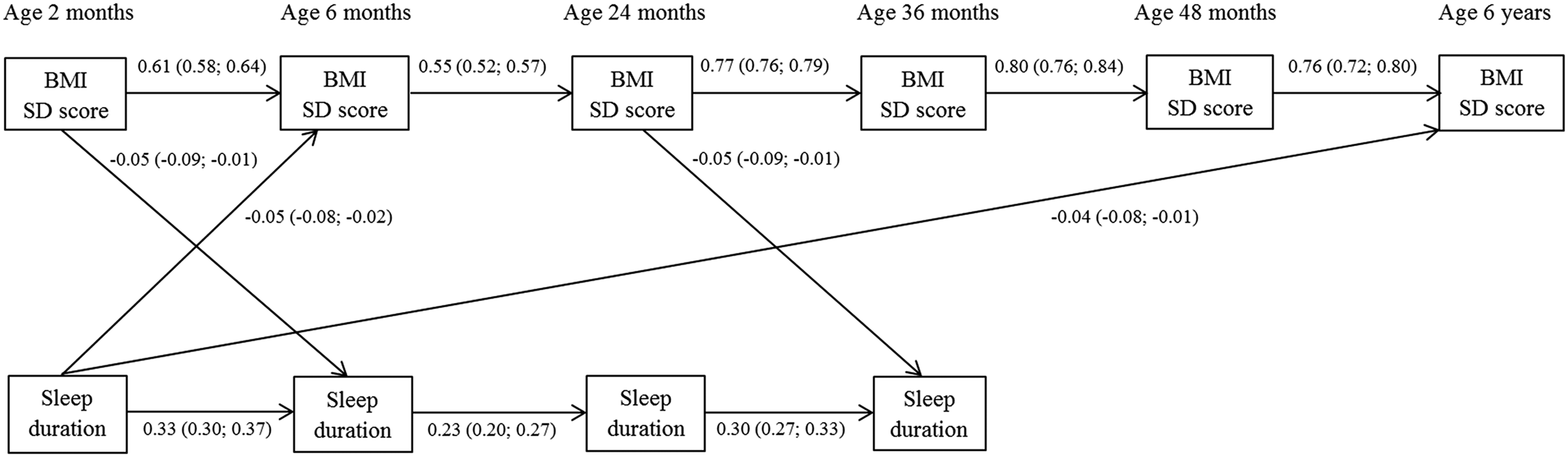
Cross-lagged model of associations between sleep duration and BMI (N = 5161). Values represent standardized linear regression coefficients (95% confidence intervals); only significant cross-lagged associations are depicted. Model fit indexes were considered as good (Comparative Fit Index: 0.867, Root Mean Squared Error of Approximation: 0.068). This model was adjusted for ethnicity, maternal education, maternal BMI, maternal psychiatric symptoms, birth weight, duration of breastfeeding, and TV watching.
Table 3 presents the associations between sleep duration and the different cardiometabolic health outcomes. Adjusted for covariates, sleep duration at 6 months was associated with higher HDL-cholesterol concentrations, while sleep duration at 2 months was inversely associated with systolic blood pressure (B = −0.013, 95% CI = −0.024 to −0.003). This association disappeared after adjustment for BMI at age 6 years (B = −0.010, 95% CI = −0.020 to 0.000; not tabulated). There were no significant associations between sleep duration at 24 and 36 months and cardiometabolic risk factors at the age of 6 years.
Associations of Sleep Duration at Different Timepoints with Cardiometabolic Health Outcomes at 6 years
Values are linear regression coefficients (95% CI). All metabolic risk factors represent standardized scores. Model 1 is adjusted for sex and age, and model 2 is additionally adjusted for ethnicity, birth weight, duration of television watching, duration of breastfeeding, maternal educational level, maternal BMI, and maternal psychopathology symptoms.
p < 0.05.
p < 0.01.
p < 0.001.
CI, confidence interval; HDL, high-density lipoprotein.
Discussion
Findings from this longitudinal population-based study suggest that a shorter sleep duration in infants as young as 2 months of age was associated with a higher BMI and higher fat mass 6 years later, with each hour less sleep predicting a 0.018 higher BMI SD score. Moreover, the cross-lagged model indicates a bidirectional relationship between sleep duration and BMI, starting already at 2 months of age. Sleep duration at later ages was neither associated with body composition after adjusting for baseline BMI nor with cardiometabolic health at the age of 6 years.
This is one of the first studies examining the prospective relationship of sleep duration in infancy and early childhood with later body composition. Although our results initially showed that sleep duration at three timepoints was related to body composition, the effects of sleep duration of 24 and 36 months on BMI and fat-free mass attenuated after adjustment for BMI at the same age as sleep. This suggests that at these ages, there was no temporal association between sleep duration and body composition. This might be due to the BMI trajectory decline and rebound that occurs between 2 and 7 years of age. 24 However, the cross-lagged model shows that the association between sleep duration and BMI appears at 2 months toward 6 months and 6 years, but not at other ages. This might indicate that this association might continue over time conditionally on the baseline relationship, since BMI and sleep duration are both reasonably stable over time, without an additive effect of sleep duration at later ages. This finding is not consistent with some other studies that reported a relationship between sleep duration in early childhood and later BMI,5–8 although two studies also found no association.9,10 None of these studies, however, examined sleep duration as early as 2 months of age. Our study suggests that infant sleep is important and might indicate a critical period for weight development with possible long-lasting effects. Therefore, this adds new evidence to previous research showing that from middle childhood onward, sleep duration is a risk factor for obesity.2–4
Different pathways could explain the observed association among short sleep duration at 2 months, higher BMI, and fat mass at 6 years of age. First, short sleep inevitably leads to having more time to eat, or at this age, to be fed by parents. Indeed, shorter sleeping children consume more calories during the night. 25 Second, it has been proposed that shorter sleep duration disturbs appetite regulation. Studies found that shorter sleep is associated with reduced leptin and increased ghrelin levels, two crucial hormones in appetite regulation, resulting in increased appetite. Third, a short sleep duration may also influence other hormonal regulations related to metabolic disturbances similar to a disturbed secretory profile of growth hormone and cortisol. 26 However, we found no support for this mechanism in children, given the lack of an association between sleep duration and insulin levels. Alternatively, both a relatively high BMI and poor sleep might be indicative of certain households characterized by a lack of regularity and unhealthy lifestyle habits.
Results from the cross-lagged model indicated that there might be a bidirectional relationship between sleep duration and BMI in early childhood, since we found an association in the opposite direction: higher BMI SD scores at the ages of 2 and 24 months predicted shorter sleep duration at the ages of 6 and 36 months, respectively. It has previously been reported that obese children sometimes suffer from sleep apnea and therefore experience poor sleep. 27 However, this is unlikely for our finding, given the young age of the children and the low prevalence of obese children in our sample. A more likely explanation is that infants with a higher BMI are perhaps less active, which might result in a decreased need for sleep. As stated above, other covariates characterized by unhealthy lifestyle habits might play a role in this association. However, these explanations are speculative and should be examined in future studies.
In this study, sleep duration in early childhood was not clearly associated with cardiometabolic risk factors in middle childhood. The observed association of shorter sleep duration at 2 months with higher systolic blood pressure and of shorter sleep duration at 2 months with higher HDL-cholesterol must be interpreted cautiously, since they were not consistent and not reflected in diastolic blood pressure or other cholesterol concentrations. Our findings contrast with other studies reporting a relationship between shorter sleep duration and a disturbed glucose homeostasis, insulin insensitivity and higher cholesterol profiles.14–16,18,19 However, in line with our results, some of these studies reported that the sleep duration-cardiometabolic health association was not independent of child BMI or was particularly evident in obese children.14,17 This suggests that the cardiometabolic changes are a consequence of obesity rather than a direct effect of short sleep duration. For instance, Cespedes et al. found that chronic sleep curtailment in early childhood was related to a higher combined metabolic risk score in midchildhood, but not after adjustment for BMI. 28 This was also partly reflected in our results, since the association between sleep duration and systolic blood pressure was not independent of BMI.
Strengths of this study were the large number of children, the repeated assessments of sleep duration starting at 2 months after birth, and the detailed measurements on cardiometabolic health. There are, however, also limitations that should be discussed. First, sleep duration was not objectively measured, but reported by parents in postal questionnaires. Parents tend to overestimate the sleep duration of their child. 19 Therefore, we tried to minimize this effect by asking parents to report the bedtimes and wake times, which previously showed good agreement with accelerometer-estimated sleep. 29 However, information on nighttime awakenings was lacking and only limited information on infant sleep during the day (categorical data only) was available. This source of imprecision might affect the infant sleep duration estimates, and ideally future studies would include more objective sleep measures in this age group. Moreover, sleep duration was not measured at the age of 6 years, when cross-sectional associations among sleep, body composition, and cardiometabolic health at this age might have influenced our findings. Another limitation was the use of 30-minute fasting blood samples instead of completely fasting blood samples, which might have reduced the accuracy of our measurements. It has previously been shown that nonfasting lipid levels may change after food intake, although this change is only minimal. 30 Furthermore, we performed a large number of statistical tests, which may have led to false-positive associations. However, applying a Bonferroni correction to our analyses based on four determinants and four grouped outcomes, namely body composition, blood pressure, lipids, and insulin, did not change our conclusions. Finally, due to loss of follow-up, Generation R participants were relatively highly educated and more often of Dutch origin, making generalizations more difficult.
Conclusion
Results from this prospective population-based study show that parent-reported shorter sleep duration as early as 2 months after birth may affect the child's body composition at the age of 6 years. Moreover, a bidirectional relationship between sleep duration and BMI was shown in infancy. Whereas effect estimates of these associations were rather small, these might reflect larger individual differences. Sleep duration in infancy is determined by intrinsic, biological factors as well as parental influences, such as bedtime interactions and soothing methods. 31 Therefore, staff members of baby-well clinics and general practitioners should inform parents about the importance of healthy sleep routines for their infant. Future research should incorporate studies with repeated assessments of sleep duration, body composition, and cardiometabolic health from birth until adulthood to monitor possible long-term effects.
Footnotes
Acknowledgments
The Generation R Study is conducted by the Erasmus Medical Center in close collaboration with the Erasmus University Rotterdam, School of Law and Faculty of Social Sciences, the Municipal Health Service Rotterdam area, Rotterdam, the Rotterdam Homecare Foundation, and the Stichting Trombosedienst and Artsenlaboratorium Rijnmond, Rotterdam. We gratefully acknowledge the contribution of general practitioners, hospitals, midwives, and pharmacies in Rotterdam. This study was granted by the Dutch Diabetes Foundation (Grant number 2013.81.1664). Prof. H. Tiemeier was awarded with a Netherlands Organization for Scientific Research grant (NWO-VIDI 017.106.370). Prof. O.H. Franco works in ErasmusAGE, a center for aging research across the life course funded by Nestle Nutrition (Nestec Ltd.), Metagenics, Inc. and AXA. Prof. V.W.V. Jaddoe received a grant from the Netherlands Organization for Health Research and Development (VIDI 016.136.361) and a Consolidator Grant from the European Research Council (ERC-2014-CoG-64916) and funding from the European Union's Horizon 2020 research and innovation program under grant agreement No. 633595 (Dynahealth). Prof. M. Wake was supported by the Australian National Health & Medical Research Council (Senior Research Fellowship 1046518) and Cure Kids New Zealand. Research at the Murdoch Childrens Research Institute is supported by the Victorian Government's Operational Infrastructure Support Program. The funders had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.