
Abstract
Abstract
Background:
Women's experience of childhood adversity may contribute to their children's risk of obesity. Possible causal pathways include higher maternal weight and gestational weight gain, which have been associated with both maternal childhood adversity and obesity in offspring.
Methods:
This study included 6718 mother–child pairs from the National Longitudinal Survey of Youth 1979 in the United States (1979–2012). We applied multiple log-binomial regression models to estimate associations between three markers of childhood adversity (physical abuse, household alcoholism, and household mental illness) and offspring obesity in childhood. We estimated natural direct effects to evaluate mediation by prepregnancy BMI and gestational weight gain.
Results:
Among every 100 mothers who reported physical abuse in childhood, there were 3.7 (95% confidence interval: −0.1 to 7.5) excess cases of obesity in 2- to 5-year olds compared with mothers who did not report physical abuse. Differences in prepregnancy BMI, but not gestational weight gain, accounted for 25.7% of these excess cases. There was no evidence of a similar relationship for household alcoholism or mental illness or for obesity in older children.
Conclusions:
In this national, prospective cohort study, prepregnancy BMI partially explained an association between maternal physical abuse in childhood and obesity in preschool-age children. These findings underscore the importance of life-course exposures in the etiology of child obesity and the potential multi-generational consequences of child abuse. Research is needed to determine whether screening for childhood abuse and treatment of its sequelae could strengthen efforts to prevent obesity in mothers and their children.
Introduction
The prevalence of obesity in U.S. children and adolescents has not improved over the past decade, affecting approximately one in six. 1 Public health efforts to prevent child obesity have largely targeted exposures in childhood, but knowledge on how to prevent obesity in early childhood is limited. 2 Evidence increasingly suggests that there are intergenerational causes of child obesity. 3 Prepregnancy obesity and excessive gestational weight gain, in particular, have been consistently linked with obesity in children.4,5 In numerous additional studies, researchers have also found adverse childhood experiences (ACE) to be associated with obesity in adulthood.6–9 Most recently, adversity in childhood has been associated with high prepregnancy BMI and excessive weight gain during pregnancy10–12 as well as offspring obesity. 13
We sought to bridge the bodies of evidence connecting childhood adversity with maternal obesity and maternal obesity with child obesity.4,5,9 Findings suggest that childhood adversity may cause long-term emotional dysregulation and depression that can lead to unhealthy eating behaviors and obesity in adulthood.14–16 In turn, obesity and excessive weight gain in pregnant women may contribute to obesity in their children.4,5 If maternal adversity in childhood does contribute to offspring obesity by causing high maternal weight and weight gain, prevention of abuse, neglect, or adversity in children and screening for ACE with treatment of its psychological consequences in women could potentially help efforts to prevent child obesity. We used 33 years of follow-up data from a diverse, national cohort study to investigate whether women's experience of childhood adversity is associated with their children's risk of obesity, and, if so, whether prepregnancy BMI and gestational weight gain partially mediate the association.
Methods
Study Population
The National Longitudinal Survey of Youth 1979 (NLSY79) is an ongoing, national, prospective cohort study that is designed to represent the U.S. population of youths aged 14–21 years old in 1979. The Bureau of Labor Statistics enrolled 12,686 youths in the study in 1979 and began enrolling the biological children of female participants into the NLSY79 Child and Young Adult study in 1986. Participants were visited in person and/or received questionnaires annually until 1994 and every two years thereafter. As shown in Figure 1, 11,512 mother–child pairs (4932 individual mothers) have participated in the studies as of 2012. A total of 3191 mothers with 7894 children participated in the 2012 survey wave (69% of the original sample), which is not an uncommon participation proportion for prospective cohort studies.17,18 Custom sampling weights created by the Bureau of Labor Statistics are used to weight the sample to match the demographics of the original target population, despite differential loss to follow-up. We included mother–child pairs in the final study sample if the child was delivered as a singleton during or after 1979, and data were available on ACE and child BMI (n = 6718). The University of California, Berkeley Committee for the Protection of Human Subjects approved the study.
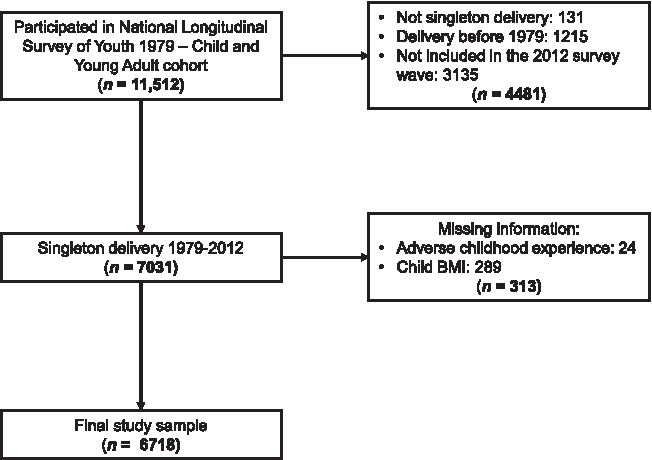
Selection flowchart of mother–child pairs for the study. Participants not included in the 2012 survey wave were intentionally dropped from the original cohort due to funding constraints, lost to follow-up, or died.
Measures
Maternal measures
In the 2012 wave of data collection, the survey administered three ACE questions, which were selected from the 11-item US Behavioral Risk Factor Surveillance System (BRFSS) questionnaire based on prioritization by a panel of child development specialists.
19
We were unable to use the full set of BRFSS ACE questions because of questionnaire length limitations. Participants were asked to recall their experience of physical abuse, household alcohol abuse, and household mental illness before the age of 18 years with the following questions:
1. How often did a parent or an adult in your home ever hit, beat, kick, or physically harm you in any way? Do not include spanking. Would you say never, once, or more than once? 2. Did you live with anyone who was a problem drinker or an alcoholic? 3. Did you live with anyone who was depressed, mentally ill, or suicidal?
Ninety-nine percent of the respondents in 2012 answered the ACE questions. We dichotomized the history of physical abuse responses as “yes” if abuse was reported as two or more times and “no” if otherwise to capture recurrent physical abuse.
The NLSY79 collected data on weight and height at each wave beginning in 1981. Prepregnancy weight and delivery weight were self-reported in the first survey postpartum starting in 1986. Specifically, within 2 years of delivery, women reported their weight “just before [they] became pregnant” and “just before [they] delivered.” We regression-calibrated height data by using error data from the National Health and Nutrition Examination Survey. The reliability of recalled prepregnancy weight and the weight reported at the closest survey before that pregnancy was 0.9. 10 Prepregnancy BMI was calculated from prepregnancy weight and height (kg/m2). Gestational weight gain was defined as the difference between delivery weight and prepregnancy weight. We converted gestational weight gain into weight gain-for-gestational age z-scores by using prepregnancy BMI-specific z-score charts previously created by our team using serial prenatal weight measurements from women in Pennsylvania with healthy, term, singleton births.20,21 Use of the z-scores accounts for the inherent link between duration of pregnancy and weight gain during pregnancy.22,23 Prepregnancy BMI and gestational weight gain were tested as mediators of any associations between maternal ACE and child obesity.4,10,11,13
Confounding maternal characteristics were selected by using theory-based causal diagrams based on prior evidence (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/chi). 24 Confounding variables included early life characteristics (race/ethnicity, born in the United States, born in the southern United States, urban/nonurban childhood home at age 14, and maternal grandmother's education level)3,13 and prenatal characteristics (age, education level, employment status, household income in year 2000 dollars and equivalized for household size, race/ethnicity, marital status, parity, and cigarettes smoked during pregnancy).4,25
Child measures
Child BMI values were calculated by using weight and height measurements that were either made in person by trained study interviewers (74% of weight and 82% of height measurements) or reported by the mother. We used the CDC growth chart SAS program to calculate age- and sex-specific BMI percentiles and to identify biologically implausible values for exclusion. 26 We assessed whether a child was ever obese (BMI ≥95th percentile) in early, middle, or late childhood (ages 2–5, 6–11, and 12–19 years, respectively), in accord with the age groups used by national child BMI surveillance methods. 1
Statistical Analysis
All statistical analyses accounted for the complex sampling design (“survey” package in R) 27 of the NLSY79 studies and family-level clustering. We first characterized the study sample and compared all variables between included, ineligible, and excluded mother–child pairs. The distributions of covariates were also compared across outcome groups to detect any patterns in the missingness of child BMI information. Multiple imputation with chained equations (“mice” package in R) 28 was used for missing covariate data. 29 The percentage of missing observations for each covariate ranged from 0% to 15%, with a median of 3%.
To test our hypothesis, we first estimated the total effect of each maternal ACE exposure (physical abuse, household alcohol abuse, and household mental illness) on child obesity in each age group (2–5, 6–11, and 12–19 years) by using log-binomial regression models, unadjusted and then adjusted for maternal early life characteristics. Because there was an overall association observed between maternal history of physical abuse and early childhood obesity in 2–5 year olds only, we limited further assessment of mediation by prepregnancy BMI and gestational weight gain to this age group. We followed the methods of Petersen et al. 30 to assess mediation, which we describe step by step in Supplementary Appendix A. In short, we applied the parametric g-formula to estimate the effect of childhood physical abuse in mothers on early childhood obesity in offspring if prepregnancy BMI and/or gestational weight gain were unrelated to childhood physical abuse. This estimate, the natural direct effect, assumes the maternal weight values to be those that mothers would have attained in the absence of physical abuse. We adjusted these analyses for the covariates previously described. Statistical analyses were conducted in R version 3.1.1. 31
Sensitivity Analyses
We prespecified several sensitivity analyses to determine the robustness of the main results to methodological changes. (1) We added interaction terms between physical abuse and each mediator to models to detect effect modification. (2) We tested joint mediation by prepregnancy BMI and gestational weight gain. (3) We changed the outcome to childhood overweight or obesity (BMI ≥85th percentile for age and sex). (4) We evaluated mediation by estimating controlled direct effects instead of natural direct effects. Natural direct effects provide estimates of the effect of maternal physical abuse on early childhood obesity if one were to intervene to prevent maternal physical abuse, thereby changing prepregnancy BMI or gestational weight gain. In contrast, controlled direct effects estimate the effect of maternal physical abuse on early childhood obesity if one were to intervene directly on prepregnancy BMI or gestational weight gain, setting them to prespecified values.
Results
The mothers of 17.3% of children in the study reported physical abuse in childhood, 11.0% reporting living with someone in their childhood home who was mentally ill, and 22.2% reported living with someone who was a problem drinker or an alcoholic. Overall, mothers were mostly non-Hispanic white, born in the United States, and had at least a high school education (Table 1). Compared with other mothers in the sample, a higher proportion of those who reported physical abuse as children were born to a mother who did not complete high school, did not complete high school themselves, had a low household income, and smoked during pregnancy. Consistent with previous findings in this sample, 10 prepregnancy obesity and high gestational weight gain were more prevalent in women who experienced physical abuse, alcohol abuse in the household, and mental illness in the household, with the strongest association being between physical abuse and prepregnancy obesity. Compared with mother–child pairs in the final sample, those ineligible for the study (nonsingleton birth, delivery before 1979, or not included in the 2012 survey) and those excluded for missing exposure or outcome data delivered in earlier years at younger ages and had lower prevalences of prepregnancy obesity and child obesity (Supplementary Table S1). Ineligible mother–child pairs reported a higher prevalence of physical abuse (21.3%) and alcohol abuse (25.7%), but they had a lower prevalence of household mental illness (7.8%) than those included in the final sample. There were no patterns detected in the missingness of child BMI information among the age groups.
Maternal and Child Characteristics in Total Sample and by Maternal Adverse Childhood Experiences
Percentages are weighted for the survey sampling design. Sample sizes are not weighted and refer to the number of mother–child pairs.
Child obesity percentages include children who had an obese BMI at least once during the specified age range.
Prepregnancy BMI and gestational weight gain were assessed as mediators. All other maternal characteristics in pregnancy were treated as confounding variables.
Based on the Institute of Medicine 2009 recommendations.
Physical abuse in a woman's childhood was associated with a higher risk of her child being obese at 2–5 years old (Fig. 2, panels A and B). After adjusting for maternal early life characteristics, children who were 2–5 years old with mothers who reported childhood physical abuse were 21% more likely to be obese. Among every 100 mothers who were physically abused, there were 3.7 excess cases of early childhood obesity compared with mothers who were not physically abused. The predicted probability of early childhood obesity was 0.21 (95% confidence interval [CI]: 0.18–0.25) if women experienced physical abuse and 0.17 (95% CI: 0.16–0.19) if women did not experience physical abuse.

Diagrams of estimates of unadjusted (A) and adjusted (B) total effects of maternal history of physical abuse in childhood on risk of obesity in children aged 2–5 years, and natural direct effect estimates for mediation by prepregnancy BMI (C) and gestational weight gain (D). RR and RD with 95% CI shown correspond to each emboldened pathway. CI, confidence intervals; RD, risk differences; RR, risk ratios.
After accounting for mediation by prepregnancy BMI, the association between maternal physical abuse and early childhood obesity was attenuated (Fig. 2, panel C). Differences in prepregnancy BMI between physically abused and not physically abused mothers accounted for 25.7% of the excess cases of early childhood obesity that occurred among mothers who reported physical abuse. Accounting for mediation by gestational weight gain, without changing prepregnancy BMI, minimally attenuated the association between maternal physical abuse and early childhood obesity (Fig. 2, panel D). Differences in gestational weight gain between mothers who reported physical abuse and those who did not were estimated to account for 5.7% of the excess cases of child obesity among mothers who reported physical abuse.
In the sensitivity analyses, adding multiplicative interaction terms between physical abuse and the mediators to the models did not change the results (Supplementary Table S2). In addition, joint mediation by prepregnancy BMI and gestational weight gain resulted in slightly smaller effect estimates as for mediation by prepregnancy BMI alone (Supplementary Table S2). Using child overweight or obesity (BMI percentile ≥85th percentile) as the outcome instead of obesity (BMI percentile ≥95th percentile) yielded attenuated effect estimates (Supplementary Table S2). Finally, controlled direct effects estimates were nearly identical to the natural direct effect estimates (Supplementary Table S3).
Physical abuse was not associated with obesity in 6–11 or 12–19-year-olds. Mental illness and alcohol abuse in a mother's childhood home were not associated with child obesity in any age group.
Discussion
We found in a diverse, national sample that maternal history of physical abuse in childhood was related to obesity in the next generation of preschool-age children. Specifically, reporting one or more episodes of physical harm from a parent or an adult in the mother's childhood home was associated with 3.7 excess cases of early childhood obesity per 100 mother–child pairs—a 21% relative increase in risk. This relationship was partially mediated by maternal prepregnancy BMI, but not gestational weight gain. Although we found no evidence of a similar relationship for older children, or for two other ACE markers, our results shed light on a possible intergenerational pathway contributing to obesity in childhood.
Abuse in childhood may lead to obesity before pregnancy through a constellation of factors, including emotional eating that is used to cope with anxiety and depression,14–16 dysregulated cortisol response and chronic inflammation,15,16 and obesogenic behaviors and environments related to socioeconomic disadvantages.6,16 In turn, obesity in pregnancy may contribute to obesity in childhood through shared genetic predispositions, epigenetic effects on offspring metabolic regulation, and shared lifestyle factors.4,5 This hypothesis is supported by recent findings in a large, national study of female nurses and their children, in which researchers reported a total association between a composite measure of physical, emotional, and sexual abuse in childhood and self-reported high BMI in adolescent offspring. 13 This association was largely attenuated by adjusting for mother's concurrent BMI but unaffected by adjustment for the child's own exposure to abuse. Our study expands previous findings to include an overall association between physical abuse and early childhood obesity and a mediating role of maternal weight before conception in a diverse study population with mostly measured child weights and heights.
The results of this study may be informative for future interventions and research. Trials that aim to promoting healthy weight gain during pregnancy have been conducted, in part, to hopefully reduce risk for child obesity.32,33 Such interventions, however, have been met with limited success in preventing excessive gestational weight gain and large-for-gestational age births, and they have not demonstrated an effect on child obesity.2,32–34 For this reason, it has recently been suggested that interventions should target maternal weight before conception, although no such randomized trials have been conducted. 35 Our results underscore the need for preconception interventions for women who are overweight or obese and suggest that incorporation of childhood abuse screening and management could bolster effectiveness in reducing maternal and child obesity.
It is unknown why our findings are limited to physical abuse and early childhood obesity. However, our results are consistent with other findings of only physical abuse being associated with adult obesity and that other ACE exposures may confer different effects than physical abuse.6–8,12 The prevalence of physical abuse in this study was similar to that among women in the BRFSS, but the prevalences of household mental illness and alcoholism were lower by 8.1 and 4.6 percentage points, respectively, suggesting that our study group may have underreported these exposures 36 ; therefore, we cannot confidently rule out their importance. We were also unable to assess other types of abuse and neglect, which could confound the association between physical abuse and early childhood obesity or be independent risk factors. Future studies that comprehensively assess abuse and neglect are needed. In addition, an association of maternal physical abuse with offspring obesity limited to preschool-age children may be due to their younger age and closer proximity to pregnancy. Exposure to both positive and negative lifestyle factors at preschool ages may overshadow the effects of prenatal risk factors in school-age children and adolescents, although we did not study this possibility. 37
Several factors limit the results of this study. Mothers self-reported all their characteristics, which may have led to some misclassification. We regression-calibrated maternal height, but lacked calibration data for maternal weight. Although self-reported weight can be prone to error, a recent systematic review concluded that self-reported prepregnancy and delivery weight do not bias associations with perinatal outcomes in most studies. 38 ACEs were recalled much later in life, although validation studies on retrospective ACE measurement suggest that our measures would likely result in false negatives and weaker associations than if ACE measures were collected earlier in life. 39 We were also only able to study three ACE exposures because of questionnaire length limitations. We were, therefore, unable to use the full set of 11 ACE questions and could not assess the severity of ACE or other ACE exposures, which would better inform the relationships between ACE, maternal obesity, and child obesity. The validity of our approach could not be tested, but shortened ACE assessment has been shown to be appropriate. 40 In addition, the available data lacked information on several factors that are likely to confound the associations studied, including psychological measures, family history of obesity, paternal characteristics, pregnancy complications, and the child's exposure to ACE. The prevalences of prepregnancy obesity and preschool-age obesity were lower in NLSY mother–child pairs ineligible for this study, which could have inflated effect sizes in the included sample. The NLSY also only collected child weight and height measurements from 1986 to 2012, resulting in measurements not being recorded at certain ages if a child was born close to the beginning or the end of the study period.
A number of strengths counterbalance this study's limitations. The NLSY79 was designed to be nationally representative of youths and adolescents in 1979 and prospectively followed participants for 33 years, including 26 years of measuring the weights and heights of female participants' children. In addition, trained study staff made 74% of weight and 82% of height measurements in person. These attributes strengthen both the internal and external validity of our results. Our mediation findings are strengthened by clear temporality, z-scores that standardized gestational weight gain for gestational duration, 20 and mediation analysis methods that improve on the conventional adjustment approach, which is often severely biased. 30
Conclusion
In conclusion, maternal physical abuse in childhood was associated with a modest increase in children's risk of obesity at preschool ages. Prepregnancy BMI explained approximately a quarter of this association. In contrast, weight gain during pregnancy explained a very small portion of the association. No associations were found with later childhood obesity or with maternal experience of mental illness or alcohol abuse in the childhood household. The results of this study expand our limited knowledge of intergenerational contributors to obesity in young children and the importance of efforts to prevent childhood abuse. In addition, they suggest that interventions to promote healthy weight before pregnancy and prevent childhood obesity should consider evaluating the impact of screening and management of maternal ACEs, particularly physical abuse.
Footnotes
Acknowledgments
The authors acknowledge the families who participated in the NLSY79 studies. This research was conducted with restricted access to Bureau of Labor Statistics (BLS) data. The views expressed here do not necessarily reflect the views of the BLS. This project was supported by the National Institutes of Health grant R01MD006014. D.H.R. is supported by the National Institute on Aging (K01AG047280).
Author Disclosure Statement
B.A. has received personal fees as a reviewer for UpToDate. The remaining authors have no financial relationships to disclose that are relevant to this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.