
Abstract
Abstract
Background:
Pediatric obesity is a public health concern related to multiple negative physical and psychosocial problems. While behavioral weight control (BWC) interventions are generally effective in decreasing pediatric weight status, these interventions are not able to reach the third of U.S. children currently classified as overweight or obese.
Method:
This review and meta-analysis examined the overall effectiveness of mobile health (mHealth) technologies employing self-monitoring, a central component of change within BWC, to decrease pediatric weight status.
Results:
Overall, a small, but significant overall effect size (d = 0.42) was found with the inclusion of nine eligible studies examining the effect on weight status. However, the quality of studies included within this weight status meta-analysis was weak, therefore limiting the interpretability of results. Analyses were also conducted examining the effect of mHealth technologies employing self-monitoring on secondary behavioral outcomes of physical activity and diet. Results indicated a small to medium, but nonsignificant effect (d = 0.41; four samples) on physical activity and a small, but significant effect on diet (d = 0.10; eight samples).
Conclusions:
Overall, the articles included in behavioral outcomes were of generally moderate quality. More work is needed to better identify the utility of mHealth and specific treatment components (such as self-monitoring), for pediatric weight management.
Pediatric obesity is a large public health concern within the United States, with approximately one-third of children being classified as overweight or obese. 1 Obesity puts children at risk for multiple negative physical and psychosocial outcomes.2–5 Due to the high rates and health implications associated with obesity in childhood, many researchers have examined effective interventions for pediatric weight management. Multifaceted standard behavioral weight control (BWC) intervention has been shown to be fairly successful in decreasing weight status of children and adolescents. 6
Self-monitoring is a central component of change within BWC7–9 and is likely the most effective technique for long-term weight loss and maintenance.9,10 In the context of BWC, self-monitoring has been shown to be an important predictor of improved weight outcomes in both children and adults.7,10,11 Self-monitoring within BWC commonly involves recording dietary intake, physical activity, and self-weighing 11 so that individuals are more aware of their current behaviors. 12 BWC and self-management strategies are effective for weight loss in children and adolescents; however, weight loss maintenance and long-term outcomes for children following standard BWC are limited. 13 Therefore, more emphasis on alternative treatment platforms may increase the number of children able to access appropriate interventions for weight status.
Growing availability of technology has increased the opportunity to use mobile health (mHealth) to aid in self-monitoring within pediatric obesity interventions. mHealth technologies include applications for smartphones, tablets, and other handheld devices, as well as sensors, short message service (text messaging), and wearable devices.14,15 Technology use for BWC may decrease burden of treatment on children, with electronic monitoring likely being less obtrusive and more novel for children. 16 A previous systematic review found that mobile technologies for pediatric obesity are generally acceptable and feasible; however, the effects on weight status and behavioral outcomes (e.g., dietary changes and physical activity) remain unclear. 17 No quantitative review has been conducted to examine the overall effectiveness of the growing field of mHealth technologies for pediatric obesity. Furthermore, previous studies have not yet examined mHealth technologies employing specific techniques previously found to be effective in pediatric weight control intervention. Thus, this study focused upon mHealth interventions utilizing self-monitoring as a primary agent of change in pediatric BWC.
Although tens of thousands of health and fitness apps are available, 18 the majority of these have not rigorously assessed the effectiveness for improvement in the target behaviors within weight control intervention. 19 Turner et al., conducted a qualitative systematic review of mobile and wireless technologies developed to address pediatric obesity. 17 This study qualitatively examined all mHealth technologies that addressed any facets of weight status, physical activity, or dietary outcomes. However, this study lacked the examination of specific behavior change strategies employed and did not include a quantitative (e.g., meta-analysis) component. 17 Despite these limitations, this qualitative review suggested that mobile and wireless technologies had positive effects on adherence to treatment, self-monitoring, physical activity, and eating outcomes (e.g., eating breakfast and fruit and vegetable consumption). 17
The goal of this systematic review and meta-analysis is to examine whether mHealth technologies for self-monitoring impact pediatric weight management outcomes. This review seeks to overcome limitations of previous reviews by taking a quantitative approach to examining studies employing self-monitoring through mHealth technologies. The primary goal of the study is to examine the use of mHealth technologies on weight status. Only studies including overweight and obese children and adolescents will be used within analyses examining the impact of mHealth on pediatric weight status, as it is not appropriate to expect weight loss within healthy weight populations. Secondary outcomes include dietary (e.g., consumption of fruits and vegetables or sugar-sweetened beverages) and physical activity (e.g., steps taken daily or number of active minutes) behavioral change-associated healthy weight management. Exploratory outcomes of physical activity and dietary changes will be examined within both healthy and overweight/obese children, as these behavior changes are appropriate across children of all BMI categories.
Method
Literature Search
Preferred Reporting Items for Systemic Reviews and Meta-Analyses (PRISMA) guidelines were followed within this systematic review and meta-analysis.20,21 For initial literature search, two electronic databases (Pubmed and PsychINFO) were systematically searched by the first author using the following search criteria: (BMI OR weight OR obesity OR overweight) AND (mHealth OR eHealth OR technology OR mobile OR electronic) AND (pediatric OR child OR adolescent). Initial search of these databases was conducted in October 2016. A total of 14,467 articles were identified through initial database searches and 1888 more articles were identified through previously published review articles, book chapters, and meta-analyses, and from forward and backward search strategies of relevant articles (see Fig. 1 for PRISMA Flow diagram). Review protocol with specific study inclusion and exclusion criteria was established before screening of articles and is available upon request.
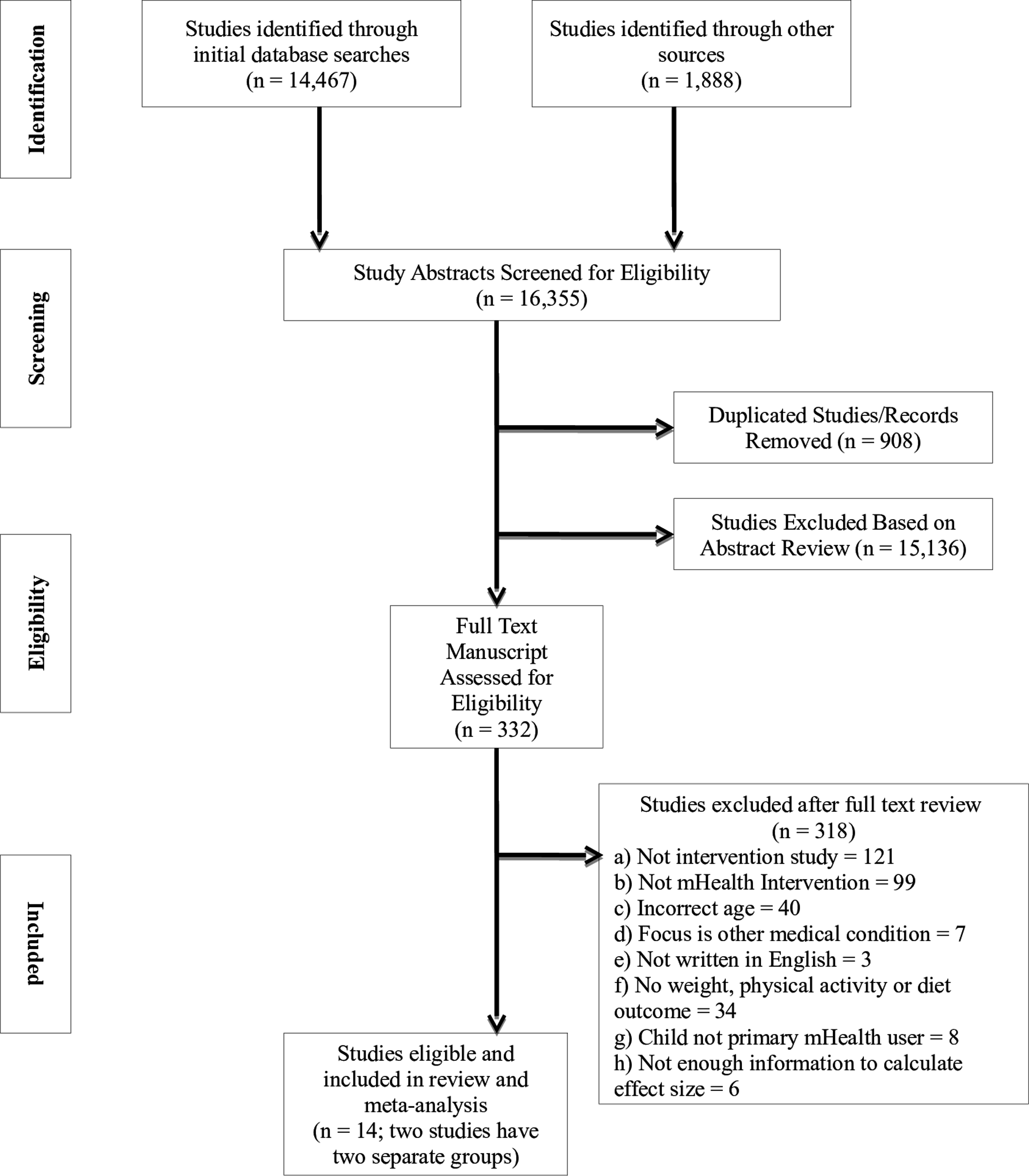
PRISMA flow diagram.
Quality Analysis
Quality ratings of studies included within final meta-analyses were scored based on the GRADE working group estimates. 22 Within this methodology, randomized trials typically start with a grade of high quality (⨁⨁⨁⨁), meaning that we are very confident that the estimate of the effect is very close to the true effect. Studies that do not include randomization begin with an initial rating of low quality (⨁⨁OO). From this point, studies may be rated down due to risk of bias, inconsistency, indirectness, imprecision, and publication bias. Therefore, four quality ratings exist: high quality (⨁⨁⨁⨁), moderate quality (⨁⨁⨁O), low quality (⨁⨁OO), and very low quality (⨁OOO).
Inclusion Criteria
Studies were included in this review if they (1) used mHealth technology to self-monitor physical activity, dietary changes, or weight status, (2) measured outcome of weight status (zBMI, BMI percentile, weight, and BMI), physical activity, or nutrition goal, (3) were written in English, and (4) identified the child or adolescent as the primary user of the mobile technology.
Exclusion Criteria
Studies were excluded from this review if they met criteria for one or more of the following: (1) article was not an intervention study, (2) the study did not fit within the scope of mHealth intervention (e.g., internet-delivered interventions), (3) mean age of participants was greater than 18 years of age, (4) primary focus of intervention was another medical condition (e.g., type 2 diabetes and asthma) or included children with an underlying medical condition leading them to gain weight (e.g., Prader-Willi Syndrome and thyroid disease), and (5) not written in English. In addition, for the primary outcome (weight status), the study was excluded if not all children were overweight (BMI percentile greater than or equal to the 85th percentile and less than the 95th percentile) or obese (BMI percentile greater than or equal to the 95th percentile) at the start of treatment, as currently healthy weight (BMI percentile greater than or equal to the 5th percentile, and less than the 85th percentile) or under weight (BMI percentile less than the 5th percentile) children are not expected to lose weight. For the exploratory aims, studies involving healthy weight youth were not excluded as these behavioral changes are appropriate for these youth.
Data Analysis Plan
If data at the same time point and from the same sample appeared within more than one study, data were only included as one effect size (this occurred for one study). 23 In addition, articles that reported upon two independent samples were both included and treated as independent samples. Analyses were conducted separately by outcome (weight status, physical activity, and dietary changes). Any findings described as nonsignificant without further statistical values were assigned an effect size of zero. 24 For the purpose of meta-analysis, a change in variables that are associated with positive health outcomes were coded as positive effect sizes (i.e., decreased weight status, improved dietary intake, and increased physical activity).
Effect sizes were converted to Cohen's d to compare between effect sizes. Guidelines for interpretation of Cohen's d are as follows: 0.20–0.49 as small, 0.50–0.79 as medium, and 0.80 and greater as large. 25 A weighted mean effect size was calculated to reflect how well the standard error estimated population parameters. The random effects model was used to account for random differences among samples. 24
Results
Search Results
Three meta-analyses were conducted for the following: weight status, physical activity, and dietary outcomes. Through literature search, seven articles with nine overall effect sizes (two articles had two separate samples) were eligible for inclusion (see Fig. 1 for PRISMA flow diagram) in examining weight status as the primary outcome. Eight overall effect sizes (from seven separate articles) were calculated to find the approximate effect of self-monitoring through mHealth technologies on dietary outcomes. Finally, only four studies (with four separate effect sizes) were eligible for a meta-analysis examining the impact of mHealth on physical activity outcomes. Please see Table 1 for description of included studies.
Description of Studies Included in Meta-Analyses
AOM, American on the Move; BWC, behavioral weight control; EFT, episodic future thinking; mHealth, mobile health; SD; zBMI, body mass index z-score.
Overall Effect on Weight Status
The overall random-effects weighted mean effect size of mHealth technologies employing self-monitoring on pediatric weight status was statistically significant (d = 0.42, 95% CI [−0.66 to −0.19]). This indicates a small, but significant effect of self-monitoring using mHealth technologies on decreased weight status in children and adolescents. 25 All studies had either null or positive effect sizes, indicating that participants within the study either decreased in weight status throughout the course of intervention (positive) or there was no effect of intervention on weight status (null). The overall quality of studies included within the BMI analysis was low, although all studies did employ objective calculation (in person) of weight status measurement (e.g., BMI, BMI percentile, and % overweight).
Two studies included within the main analyses examining the impact of self-monitoring through mHealth on BMI outcomes were randomized controlled trials. de Niet et al. 23 examined the impact of self-monitoring through text message on weight status. The intervention group was asked to send weekly text messages indicating their exercise, eating behavior, and mood for the week, following an in-person behavioral lifestyle intervention. Although self-monitoring through text messages was found to be feasible for overweight and obese children, this study did not find a significant effect on weight. 23 This may be due to the relatively low frequency of requested messages (once per week), as it does not require children to be closely self-monitoring these behaviors daily.
The second randomized controlled trial included in this study examined a multifaceted intervention, partially delivered through mHealth technologies and partially delivered through in-school intervention. 26 This study included physical activity sessions delivered by teachers, pedometers provided to students for self-monitoring, parental strategies encouraged through newsletters, and a smartphone application. Similar to de Niet et al., 23 there were no significant changes in weight status over the course of the 8-month intervention period. 26 This is surprising as this study included treatment components that have shown to be effective within past studies (e.g., school-based intervention components). 27
Overall Effect on Dietary Behavior
Eight samples (from seven articles) were eligible for a meta-analysis examining the effect of self-monitoring through mHealth on dietary behavior change. The overall random-effects weighted mean effect size of mHealth technologies employing self-monitoring on dietary outcomes (e.g., sugar-sweetened beverages, fruit and vegetable consumption) was statistically significant (d = 0.10, 95% CI [0.002–0.024]). This indicates a very small, but significant effect size. 25 Overall, the quality of studies included within this meta-analysis was moderate.
Overall Effect on Physical Activity
A third and final meta-analysis was conducted to examine the effect of interventions employing self-monitoring through mHealth on physical activity outcomes. Only four articles were eligible for this meta-analysis (Table 1). The overall random effects weight-mean effect size was not statistically significant (d = 0.489, 95% CI [−0.322 to 1.299]). This indicates a small to medium effect size, however, likely due to the small sample size of articles included; a large standard error (0.414) does not allow us to draw accurate conclusions about the impact of self-monitoring through mHealth on physical activity behaviors. Studies within the physical activity meta-analysis generally demonstrated moderate quality.
Discussion
Conclusions that may be drawn from this meta-analysis are limited due to the low to moderate quality of studies that have examined self-monitoring through mHealth and the small number of randomized controlled trials that show the impact of these interventions on weight change, dietary, and physical activity outcomes. However, overall, results showed that self-monitoring techniques using mobile technologies have a small, but significant effect on weight status in children and adolescents. This finding is consistent with previous meta-analyses in standard BWC not involving mHealth, in that, small to medium effects for improvement of weight outcomes are likely to occur following BWC interventions.28–30
Primary Outcome: Meta-Analysis Examining Pediatric Weight Status
As shown within the table, most studies included within the primary meta-analysis examining weight status outcomes were pre-post in design, examining the weight status of children over the course of intervention.31–34 While pre-post designs are able to show that children lost weight over the course of the treatment, they do not provide any comparison group, and therefore, we are unable to attribute the changes in behaviors or weight status to the intervention being examined.
Secondary Outcomes: Meta-Analyses Examining Dietary Intake and Physical Activity
We found a very small effect size for the impact of self-monitoring through mHealth on children's dietary behaviors. The primary behaviors that were examined were sugar-sweetened beverage consumption26,35 and fruit and vegetable consumption.36–39 One study included both outcomes. 40 These studies demonstrated moderate quality overall; however, only two of the included studies were high-quality studies.35,40 Because the majority of articles included with pre-post design, it is difficult to accurately understand the true effect that self-monitoring through mHealth may have on dietary outcomes in healthy weight or overweight youth.
This research also highlights the need for high-quality research examining the impact of self-monitoring through mHealth on children's physical activity behaviors. We were unable to make accurate conclusions about the impact of self-monitoring through mHealth techniques due to the small number of studies eligible for these analyses and the ongoing need for larger randomized controlled trials. While an overall moderate effect size was detected for the effect of self-monitoring through mHealth on pediatric physical activity, this was not a significant effect. The research that does exist within this area appears to be of moderate quality, showing the promise of using mHealth technologies to affect physical activity behavior changes, although more research is needed.
Limitations
Although this review improves the understanding of how mobile technologies employing self-monitoring may impact pediatric weight management intervention, these findings should be considered within the context of several significant limitations. Primarily, a small amount of studies were eligible for inclusion in these meta-analyses and those included were generally low to moderate quality studies, decreasing the statistical power associated with primary and secondary analyses. Furthermore, there was considerable variability in the specific components within each study, which precludes the ability to isolate self-monitoring as the only agent of change. Another limitation of this review is the limited availability of research on mHealth technologies as a stand-alone treatment, without other in-person treatment components, as some studies included within this review employed mHealth technologies in addition to in-person components or directly following standard in-person BWC.31–33
No dismantling studies currently exist to examine the effectiveness of self-monitoring through mHealth alone compared to self-monitoring as part of a larger treatment. Specifically, although self-monitoring was the primary mHealth component within each of these studies (Table 1), the consistency between how self-monitoring was employed varied considerably between studies. For example, some studies included self-monitoring through text messaging to researchers 38 and others used smartphone applications to have participants track behaviors. 32 Furthermore, some studies employed self-monitoring as a modality to have children change behavior (e.g., decreasing snacking), 33 whereas other studies included self-monitoring alone as the primary treatment component following standard BWC. 23
Future Directions
Due to the lack of consistency in included components between studies and the lack of dismantling studies available, self-monitoring cannot be isolated as the agent of change within included studies. Therefore, these meta-analyses should be used as a starting point for future research. Specifically, dismantling studies should be conducted to identify specific agents of change that may be impacting these findings. Future research should focus on randomized controlled trials examining mHealth techniques compared to traditional in-person BWC interventions. Randomized controlled trials should also examine multiple behavioral outcomes associated with pediatric weight management, as it is not clear from this research whether mHealth technologies may be differentially effective for certain behavioral targets (i.e., dietary vs. physical activity). Researchers should also seek to understand the context in which mHealth is most effective for behavioral weight management. For example, it remains unclear whether mHealth interventions are most effective when used in conjunction with in-person BWC, when used to contact providers, or when used as independent treatment modalities. Overall, understanding specific components and contexts for mHealth may help to broaden the accessibility of BWC interventions.
Overall, this review and meta-analysis sought to show the effectiveness of employing mHealth technologies utilizing self-monitoring techniques to produce beneficial outcomes in pediatric obesity intervention. However, more research is needed to draw appropriate conclusions about the use of mHealth technologies on pediatric obesity outcomes. mHealth is a novel and possibly powerful resource, but more research is required to understand the ways that mHealth can be best employed to address high rates of pediatric obesity. This review and meta-analysis furthers the literature by quantitatively demonstrating some positive effects of mHealth technologies. Findings highlight the need for future collaborations among technology developers, researchers, and BWC interventionists to develop mobile technologies that can be used to reach the substantial number of children and adolescents affected by pediatric obesity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.