
Abstract
Abstract
Background:
There is growing evidence that attention-deficit/hyperactivity disorder (ADHD) and loss of control (LOC) eating, both prevalent in children and adolescents, may be related to one another. However, the relationship between ADHD and overeating without LOC has been largely unexamined, thus precluding an understanding of the independent contributions of LOC and episode size in these associations. The current study sought to examine associations between ADHD symptoms and maladaptive eating by evaluating three different types of eating episodes characterized by the presence/absence of LOC and the amount of food consumed: objectively large LOC episodes [objective binge eating (OBE)], subjectively large binge episodes [subjective binge eating (SBE)], and objectively large overeating episodes without LOC [objective overeating (OO)].
Methods:
Participants were 385 youth (M age = 10.89, SD = 2.25) drawn from five different research protocols at institutions across the United States. Participants and their parents completed questionnaires and semistructured interviews to assess ADHD symptoms, OBE, SBE, and OO.
Results:
As hypothesized, negative binomial regressions revealed that ADHD symptoms were significantly associated with OBE, χ2(1) = 16.61, p < 0.001, and with OO, χ2(1) = 10.64, p < 0.01. Contrary to expectations, they were not associated with SBE.
Conclusions:
These results indicate the need for future studies to explore possible shared mechanisms (e.g., impulsivity) underlying associations between ADHD symptoms, OBE, and OO. Clinical implications include support for considering ADHD symptoms in programs that target both prevention of LOC eating and obesity more generally.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a prevalent condition affecting 3–10% of school-aged children.1,2 ADHD is characterized by two categories of impairment, hyperactivity/impulsivity and inattention, and can be diagnosed in individuals who experience clinically significant symptoms in either one or both domains. 3
In addition to the impairments that are characteristic of the disorder, ADHD has been linked to a range of adverse health outcomes, including poor sleep, diabetes, and obesity. 4 In particular, an increasing number of cross-sectional studies have begun to examine the link between obesity and ADHD and have found a bidirectional relationship between the two conditions in children. 5 Furthermore, there are now longitudinal studies suggesting that ADHD symptoms in childhood may play a causal role in the development of overweight in adolescence and adulthood.6,7
Despite mounting evidence in support of a link between ADHD and obesity, the mechanisms underlying the association are less understood. ADHD symptoms have been positively linked to multiple dietary factors, such as sugar-sweetened beverage consumption and total caloric intake.8,9 Likewise, other mechanisms have been suggested, such as genetics and circadian rhythm disruption. 5 Additionally, several studies have indicated that dysregulated eating may be a significant contributor to the increased rates of obesity in individuals with ADHD. 5 More specifically, loss of control (LOC) eating has been identified as a potential mediator of the relationship between ADHD diagnosis and zBMI score in children. 10
LOC eating is characterized by the subjective experience of being unable to control what or how much food one is eating. 3 LOC, along with the consumption of an objectively large amount of food in a given period of time (i.e., objective binge eating or OBE), is the central component of binge eating disorder (BED). 3
Because it is difficult to classify what is considered an objectively large amount of food for a child, and because LOC eating in children is associated with significant distress and impairment regardless of whether an objectively large amount of food is consumed, 11 research in children has focused on the experience of LOC, irrespective of episode size. A recent review of the literature found similar levels of psychosocial impairment (e.g., anxiety, depression, internalizing, and externalizing symptoms) and BMI in youth with OBE compared with youth who experienced LOC without overeating (i.e., subjective binge eating, or SBE). 12
There is also evidence that LOC may be critically linked to obesity. LOC eating occurs in youth with overweight at greater rates than their normal weight counterparts, the likelihood of reporting LOC eating appears to increase proportionally with weight, 13 and LOC eating is a strong predictor of subsequent weight gain. 14
In addition to obesity, the few studies that have assessed LOC eating and ADHD have also found associations between the two. Reinblatt et al. found that school-aged children with an ADHD diagnosis showed a 12-fold increase in the odds of reporting LOC (with no distinction between SBE and OBE). 10 Another study that looked only at OBE found a significant positive association between OBE and ADHD symptoms in young adults. 15 However, few studies have evaluated associations between LOC and ADHD in children with obesity, despite links between obesity and both LOC and ADHD.
Although there is a growing body of literature supporting the importance of LOC in connection with both obesity and ADHD symptoms, fewer studies have assessed the impact of overeating without LOC (objective overeating; OO). Some of the research that does exist shows that OO and OBE may lie on a continuum such that individuals who report OO experience more distress than those who do not experience OO, and individuals who report OBE, in turn, experience more distress than those with OO. 16 Other studies have found that individuals with both OBE and SBE experience more eating pathology (e.g., shape and weight concerns) than those with OO. 17
With regard to zBMI, findings are mixed, with some studies demonstrating that individuals with OO weigh significantly less than those with OBE and others finding no difference. 12 When studied longitudinally, Sonneville et al. found that OBE was uniquely predictive of weight gain in adolescents and young adults, while OO was not 18 ; however, this is the only study to date that has examined the predictive validity of OO. 12 The apparent lack of research on OO is problematic given the importance of teasing apart the effects of LOC and episode size to understand whether they are differentially associated with other negative outcomes, such as obesity and ADHD.
When considering ADHD specifically, the literature on OO is also limited. Sonneville et al. found that ADHD symptoms were associated with overeating during late childhood; however, they assessed overeating by asking children if they had ever eaten so much that they were in pain or made themselves throw up. 19 Therefore, overeating in this context is representative of more than just eating an objectively large amount of food as it also introduces the idea of compensatory behavior. Other studies have found that an ADHD diagnosis is associated with higher daily calorie consumption, but have not evaluated OO specifically. 8
Although the literature points to the idea that both LOC and overeating may be associated with ADHD symptoms, more research must be conducted to test this hypothesis with well-established definitions and measures of overeating. Furthermore, the studies that have examined associations between LOC and ADHD symptoms have done so by including both OBE and SBE in the definition of LOC 10 or by only evaluating OBE without SBE. 15 However, links between ADHD symptoms and OBE, SBE, and OO should be examined separately to avoid confounding LOC with episode size. Likewise, continuing to tease apart the distress associated with LOC vs. episode size is also important as OBE is currently required to receive an eating disorder diagnosis. 3
Finally, little attention has been given to how other demographic factors, such as age and gender, may impact the relationship between ADHD symptoms and dysregulated eating (i.e., OBE, SBE, or OO). Such factors may be important to consider given that ADHD is more often diagnosed in boys than in girls 20 and OBE appears to emerge in adolescence. 18
The current study seeks to expand the literature by evaluating the association between ADHD symptoms and both LOC and eating episode size in youth with overweight. It examines ADHD symptoms in the context of (1) OBE, (2) SBE, and (3) OO to determine whether these conditions are differentially related to ADHD symptoms.
Many studies have examined LOC eating in children meeting criteria for an ADHD diagnosis, but have not evaluated prodromal ADHD symptoms, which have important implications for prevention or early intervention programs. This study utilizes ADHD symptoms in place of a formal ADHD diagnosis to evaluate the association between attention and impulsivity on LOC eating and overeating across a spectrum of severity levels. It also examines the frequency of OBE, SBE, and OO, as opposed to presence or absence, as this appears to be of importance in youth with overweight. 21 Finally, this study investigates whether age and sex moderate the relationship between ADHD and dysregulated eating.
It is expected that ADHD symptoms will be positively associated with LOC eating episode frequency, such that OBE and SBE frequency will each be significantly associated with ADHD symptoms. Likewise, we expect that ADHD symptoms will also be positively associated with OO frequency. Finally, we hypothesize that these associations will be stronger for older children than for younger children and stronger for boys than for girls.
Method
Participants
Participants included were 385 youth who were overweight or obese (M age = 10.89, SD = 2.25). The majority of participants were female (63%) and Caucasian (60%). On average, participants had a standardized BMI score of 2.26 (SD = 0.34), which corresponds to the 97th age- and sex-adjusted percentile. See Table 1 for full participant characteristics for both the total sample and by dysregulated eating status.
Participant Characteristics by Dysregulated Eating Status
Dysregulated eating = Report of objective binge eating episode, subjective binge eating episode, or objective overeating episode.
Multivariate analysis of variance (MANOVA), including age, zBMI, ADHD symptoms, and dysregulated eating in the model.
Chi-square test of association.
ADHD, attention-deficit/hyperactivity disorder.
For the purposes of the current study, dysregulated eating is defined as reporting OBE, SBE, or OO. The current sample was drawn from a larger pool of individuals (n = 526) presenting for a number of different protocols at research institutions across the United States (Washington University School of Medicine,22,23 The University of Chicago, 24 Children's Hospital Boston, 25 San Diego State University/University of California San Diego, 26 and University of Minnesota 27 ), including nonintervention studies and weight loss treatment studies, as well as for clinic-based treatment of eating disorders or obesity. See Table 2 for detailed inclusion criteria for each site.
Participant Characteristics by Study Site
In addition to the criteria listed in Table 2, participants were included in the current study if they completed the Child Behavior Checklist (CBCL), the Eating Disorder Examination (EDE), Child or Adult Version, and had recorded height and weight measures.
Procedure
Institutional Review Board approval was obtained for the research protocols at each respective site. Informed consent was provided by each participant's parent/guardian and written assent was obtained from each child before participation in the study. The current study only includes baseline data that were collected before participation in any treatment or experimental study.
Measures
Demographics
zBMI and BMI percentile scores were calculated based on standardized height and weight measurements for age. Race was categorized as Caucasian, African American, or Other, and ethnicity was categorized as Hispanic or Non-Hispanic.
Eating Disorder Examination
Participants completed the EDE or the child EDE (ChEDE). 28 The EDE and the ChEDE are semistructured interviews used to diagnose eating disorders and assess related symptomatology. The two interviews are nearly identical, but differences between the ChEDE and the EDE include modifications to simplify language and complex concepts (e.g., overvaluation of shape and weight) for children. Higher scores represent more severe eating disorder psychopathology.
The EDE and ChEDE define OBE as eating episodes characterized by both LOC and consumption of an objectively large amount of food according to clinical rating standards, and SBE as LOC eating episodes in which the respondent considers the amount of food eaten to be excessive, but that amount is not considered objectively large by clinical rating standards. OO is defined as consumption of an objectively large amount of food without LOC. OBE, SBE, and OO frequencies were recorded for the past 28 days. Both the EDE and ChEDE have good reliability and validity.28,29
Child Behavior Checklist/6-18
The CBCL is a 113-item caregiver report measure used to assess problematic behavior in children. 30 The CBCL has several behavioral subscales, including an Attention Subscale, as well as a total score that represents global behavioral issues. Respondents report their agreement with how much each item describes their child now or in the past 6 months on the following three-point scale: 0 [Not True (as far as you know)], 1 (Somewhat or Sometimes True), and 2 (Very True or Often True). The 10-item Attention Subscale was used for the current study to assess for ADHD symptoms. Items include statements asking how much the child is “Impulsive or acts without thinking” and “Inattentive or easily distracted.” T-scores range from 0 to 100, and scores greater than 65 are considered to be in the clinical range. The CBCL has good reliability and validity,30,31 and the Attention Subscale has been found to have excellent discriminating power for detecting ADHD. 32 Continuous t-scores were used in all analyses.
Statistical Analyses
All analyses were conducted using SPSS, Version 24.0. Preliminary analyses were conducted using analyses of variance to characterize the sample (Table 1). The primary study analyses were then conducted in two phases, adjusting all models for study site, as well as race, age, gender, and zBMI, as is customary in the literature. 10
A series of negative binomial regression models were used to examine relationships between ADHD symptoms and dysregulated eating. Negative binomial regression was used due to the existence of count data for all dependent variables (OBE, SBE, and OO). Negative binomial regression differs from normal (ordinary least squares) regression, in that it does not allow for negative integers, accounts for a distribution skewed toward zero, as is often the case with count data, and allows for overdispersion of the model (i.e., the variance exceeds the mean). 33 It is a generalized linear model in which predicted scores are expressed as natural logarithms. Before conducting the analysis, all variables were centered to avoid multicollinearity. 34
In the first model, OBE frequency was entered as the dependent variable. Study site was entered as a covariate to adjust for any confounding effects. In addition, race, age, gender, and zBMI were also entered into the model as covariates, and ADHD symptoms were entered in as the independent variable of interest. Additionally, the age × ADHD symptom and gender × ADHD symptom moderators were entered. In the second and third models, respectively, SBE and OO frequencies were analyzed separately using the same approach.
Results
Descriptive Information
Means, standard deviations, and correlations are presented in Table 3. Overall, participants had an average CBCL Attention Problems score of 55.05 (SD = 7.01), which fell in the nonclinical range. Eleven percent of participants (n = 45) met criteria for clinically significant ADHD symptoms (CBCL scores greater than or equal to 65). As can be seen in Figure 1, about 1/3 of youth (n = 125) in our sample endorsed at least one dysregulated eating episode (OBE, SBE, or OO). Of those, 72% reported had at least one LOC episode (n = 89). Overlap between OBE, SBE, and OO was also examined (Fig. 1). Eighty percent of youth who had a dysregulated eating episode only endorsed one type. SBE was the most common, followed by OO, and then OBE. The largest amount of overlap was between OBE and SBE, with 11 participants endorsing both. Only 2% of all participants reported having all three forms of dysregulated eating.
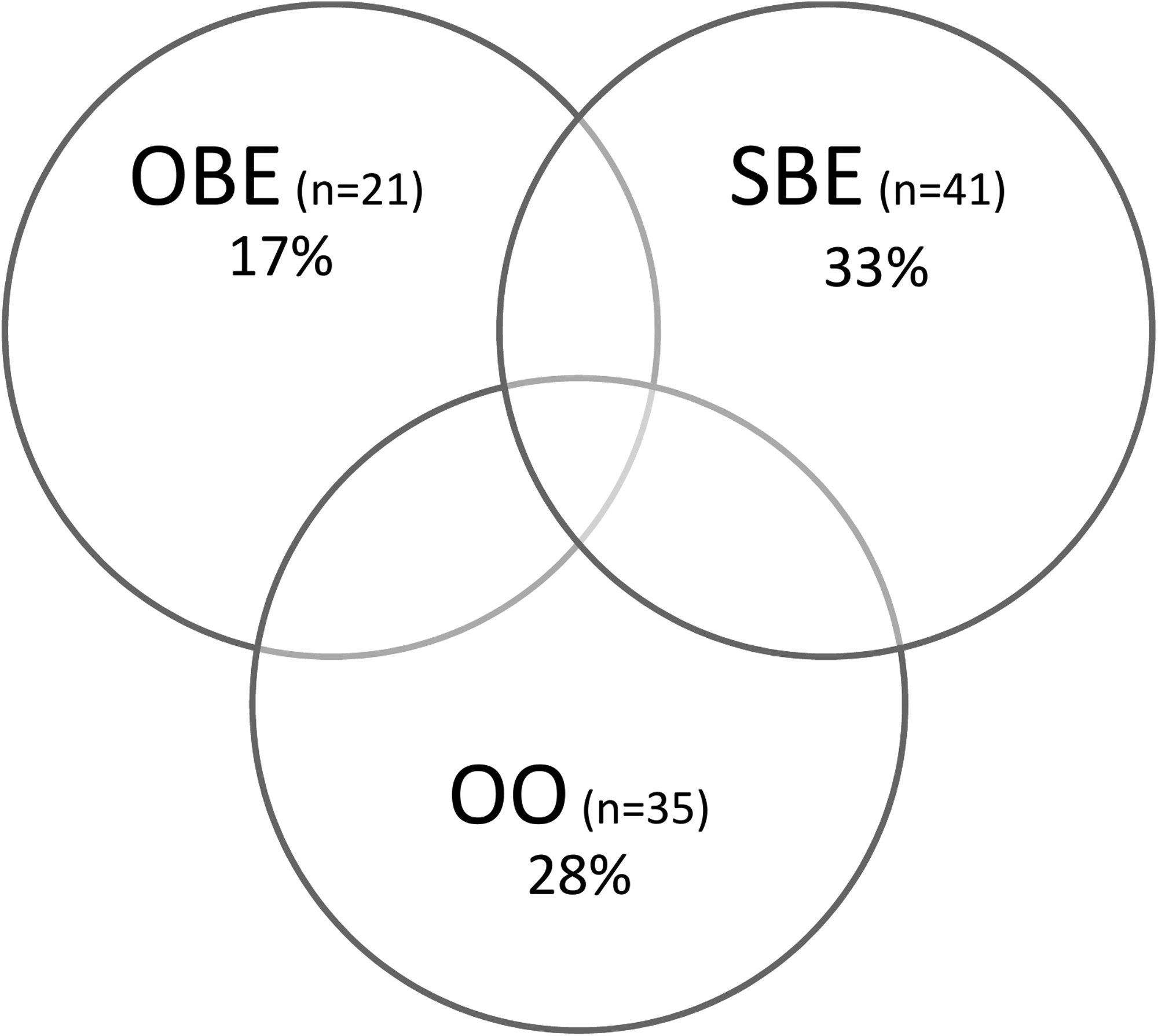
Venn diagram of prevalence rates of objective binge eating (OBE) episodes, subjective binge eating (SBE) episodes, and objective overeating (OO) episodes. Of 385 total respondents, 124 exhibit at least one OBE, SBE, or OO episode. Percentages shown in this diagram are based on n = 124 as the divisor.
Means and Correlations of Variables of Interest
p < 0.05; **p < 0.01.
ADHD Symptoms and Associations with Dysregulated Eating
ADHD symptoms were then specifically evaluated using negative binomial regression. Full results of the regression analysis are presented in Table 4. First, associations between ADHD symptoms and OBE were evaluated. The likelihood ratio for the full model was χ2(9) = 129.44, p < 0.001, indicating model significance. Adjusting for study site, race, age, gender, and zBMI, Wald chi-square analyses indicated that ADHD symptoms were positively associated with OBE frequency χ2(1) = 16.61, p < 0.001, such that there was a 6% increase in OBE frequency for every one-point increase in ADHD symptoms. Next, SBE frequency was evaluated. The likelihood ratio for the full model was χ2(9) = 189.88, p < 0.001, which indicated that the overall model was significant. However, Wald chi-square analyses revealed that ADHD symptoms were not significantly associated with SBE frequency χ2(1) = 1.30, p = 0.25.
Summary of Three Negative Binomial Regression Analyses for Variables Predicting Objective Binge Eating Episodes, Subjective Binge Eating Episodes, and Objective Overeating (n = 385)
All models adjusted for study site.
p < 0.05; **p < 0.01; ***p < 0.001.
Finally, OO frequency was evaluated. The likelihood ratio for the full model was χ2(9) = 88.63, p < 0.001, indicating model significance. Wald chi-square analyses indicated that adjusting for study site, race, age, gender, and zBMI, ADHD symptoms were also positively associated with OO frequency χ2(1) = 10.64, p < 0.01, such that there was a 5% increase in OO for every one-point increase in ADHD symptoms. Contrary to hypotheses, age and gender were not significant moderators of the relationship between ADHD and OBE, SBE, or OO.
Discussion
The current study assessed the relationship between ADHD symptoms and three types of maladaptive eating, LOC with overeating, LOC without overeating, and overeating without LOC, in a sample of youth with overweight. This study sought to examine whether the relationship between ADHD symptoms and eating behavior differed by episode size (objectively or subjectively large) and by the presence/absence of LOC. We found that OBE and OO frequencies were both associated with ADHD symptoms. However, there was no significant association between ADHD symptoms and SBE frequency, indicating that associations between ADHD symptoms and dysregulated eating behavior may be better accounted for by variations in episode size, rather than the presence of LOC.
This study contributes to the literature in several ways. First, it builds upon previous findings that ADHD symptoms are significantly associated with LOC eating in youth. 10 Moreover, this study also builds on the literature by showing that when OBE and SBE are considered separately, ADHD symptoms are only associated with OBE frequency. Although previous research has found few differences in psychopathology between youth with OBE and with SBE, 12 most studies have not examined ADHD symptoms specifically. It is possible that OBE and SBE are differentially related to some forms of psychopathology, but not others. This study also found that in addition to OBE, ADHD symptoms are associated with OO in youth with overweight.
One explanation for our findings may lie in shared mechanisms underlying ADHD symptoms, OBE, and OO. The literature has shown that children with ADHD have more difficulty inhibiting their desire for immediate small rewards in favor of long-term large rewards and that they make more impulsive errors on tasks measuring inhibitory skills.35,36 Likewise, problems with impulsivity have also been found in youth with and without overweight who also endorse LOC eating, using both objective and self-report measures.10,37,38
Given these findings one hypothesis is that overeating (with or without LOC) may be a behavioral manifestation of the impulsivity that is also characteristic of ADHD. This is supported by the adult literature, which has found that individuals who experience OBE have significantly more problems with impulse control than those who only experience SBE. 39 Likewise, greater levels of impulsivity may explain why some individuals act upon feelings of LOC by overeating, while others can experience those feelings, but not engage in OBE. While no study to our knowledge has evaluated impulsivity in youth who experience OO, it is possible that these individuals also demonstrate diminished levels of inhibitory control. OO and OBE both share a central component—overeating.
While individuals with OO do not endorse losing control over how much they are eating, they may still be eating impulsively due to internal or external cues (e.g., boredom or environmental cues). However, this theory should be tested by empirical research on the mechanisms underlying OO.
In addition to theoretical implications, this study's evaluation of prodromal symptoms of ADHD has important implications for prevention, namely that OBE and OO may be problems even for children who do not meet full criteria for ADHD. While the inclusion of participants with a full spectrum of ADHD symptoms is a strength of the study, it is not possible to distinguish whether including children who were symptomatic for ADHD, but did not meet full criteria for the disorder, might have impacted the findings. It is possible that in children who have a diagnosis of ADHD, symptoms would be more strongly related to OBE than to OO. However, the results of this study show that at subclinical levels of ADHD, children with overweight may be susceptible not only to OBE but also to OO.
This study has several strengths, including a large sample comprising both treatment-seeking and nontreatment-seeking participants. As noted above, an additional strength of this study is the emphasis on prodromal symptoms of ADHD and implications in the context of prevention. Finally, this study used well-validated semistructured interviews to evaluate LOC eating and OO.
Limitations of the study include the cross-sectional nature of the data as well as the lack of diversity of the sample given that all participants were overweight, which precludes generalizing the findings to normal weight youth. The restricted zBMI range of the sample may explain our findings that zBMI was not significantly associated with OBE, SBE, or OO and that it was not correlated with ADHD symptoms. Additionally, ADHD symptoms were identified using a caregiver report questionnaire, without corroborating neuropsychological testing or direct observation. Such questionnaires may be subject to the bias of a single reporter, which could have impacted the results.
Finally, in the current sample, the mean age of participants was just under 11 years. Although (consistent with previous literature) participants who endorsed dysregulated eating were older than those who did not (Table 1), the mean age was still under 12 years. Thus, the age of the sample may have impacted our findings as research has found that ADHD symptoms in early childhood are associated with overeating in middle childhood, and then finally OBE in adolescence. 19 As such, it is possible that more participants would have endorsed OBE had the sample been older.
In summary, ADHD symptoms appear to be associated with overeating in youth both with and without LOC. However, LOC without overeating does not appear to be linked to ADHD symptoms. These findings suggest that both OBE and OO may be linked to impaired impulsivity/inattention. Future studies should examine potential underlying mechanisms explaining associations between OBE/OO and ADHD symptoms in children and explore possible associations between these forms of dysregulated eating and specific symptoms of ADHD (e.g., hyperactive vs. inattentive symptoms).
Future research should also be conducted to examine the relationship between OO/OBE and ADHD symptoms in a longitudinal manner to assess whether youth with subthreshold ADHD symptoms are more likely to develop BED in adulthood. Finally, the findings of this study demonstrate the importance of conducting longitudinal research on all types of overeating and LOC eating among youth to elucidate the prospective impact and overlap of these different conditions.
Footnotes
Acknowledgments
The authors wish to acknowledge the following funding sources: NIH grants T32-MH082761 (Dr. Le Grange), R01-HD036904 (Dr. Wilfley), K24-MH070446 (Dr. Wilfley), P30-DK50456 (Drs. Peterson, Zucker, and Boutelle), F31-MH071019 (Dr. Eddy), and K23-DK105234 (Dr. Goldschmidt); a National Science Foundation Graduate Research Fellowship (Ms. Egbert); an Academy for Eating Disorders Graduate Student Research Grant (Dr. Goldschmidt); an American Psychological Association's Division 38 Student Research Award (Dr. Celio Doyle); and an RGA/Washington University Longer Life Foundation Research Award (Dr. Wilfley).
Author Disclosure Statement
No competing financial interests exist.