
Abstract
Abstract
Background:
Pediatric obesity is recognized as a worldwide epidemic. Treatment of this problem has proven difficult, but many promising interventions exist, including immersion treatment. The purpose of this study is to examine the potential influence of psychotropic medications on immersion treatment outcomes in a real-world treatment setting.
Methods:
This study examines the prescription rates of psychotropic medications and treatment process and outcomes of 642 adolescents in ten different cognitive behavioral therapeutic immersion weight-loss camps in the United States and in the United Kingdom.
Results:
The US participants received psychotropic medications at drastically varying rates by geographical location and overall at almost ten times the rate of UK participants. Those taking psychotropic medications engaged in treatment and decreased percentage overweight at similar rates as their nonmedicated peers. The medication group reported higher initial and final rates of distress, but both groups improved their moods during camp and exhibited smaller differences in mood ratings by the end of camp.
Conclusions:
Significantly higher prescription rates of psychotropic medication, especially evident comparing the United States to the United Kingdom, were unrelated to immersion obesity treatment process and outcomes for youth. Immersion treatment for obese adolescents appears effective regardless of psychotropic medication status of the participant. This finding supports the use of cognitive behavioral immersion treatments for adolescent obesity and leads to several possible conclusions and directions for future study.
Introduction
Healthcare professionals now recognize pediatric obesity as a worldwide epidemic with adverse consequences in many aspects of life.1–3 Although effective treatments can ameliorate these problems in many cases, 4 tremendous variability characterizes the results. In fact, even with high-quality professional interventions, many, perhaps most, participants fail to benefit in the long run.4–6 Research that examines which adolescents benefit from which interventions may help decrease the variability in outcomes, in part, by suggesting ways to improve the effectiveness of treatments. 7
Immersing young people in nearly ideal weight-controlling environments for extended periods of time and providing them cognitive-behavior therapy (CBT) during immersion has produced promising results.7–9 More specifically, Kelly and Kirschenbaum's review 8 indicated that immersion plus CBT produced almost 200% greater reductions in percent overweight than those reported for either immersion without CBT or outpatient treatment. Participants who reported greater confidence and peer social support experienced better treatment outcomes. 10 However, other characteristics of participants in these CBT immersion treatments that impact outcomes are largely unknown.
Psychotropic medications are common and probably influential in obesity treatment for adolescents. Recent trends indicate an approximately fivefold increase in psychotropic medication use among all adolescents in the United States in the past 25 years. 11 Obese adolescents appear to receive nervous system medications (analgesics and psychotropics) at higher rates than their normal weight peers, 39% higher in a nationally representative sample of obese 12–19 year olds in Canada. 12 Although well intentioned and likely beneficial in some cases with significant psychological distress, prescribing psychotropic medication to obese adolescents may be problematic. Obesity predicts depressive symptoms, although not major depressive diagnoses, among adolescents, 13 but a meta-analysis 14 revealed that the most commonly prescribed antidepressant medications had no greater effect than placebo on mild and moderate levels of depression. Atypical antipsychotics could adversely affect obesity treatment outcomes due to their association with significant weight gain among adolescents. 15 Other concerning and treatment-relevant side effects of psychotropic medications include sedation, decreased motivation, and even, perhaps, a greater risk of suicide.16–18 These concerns become especially relevant for obese adolescents in CBT immersion treatment. Treatment seekers generally report greater degrees of psychological distress than obese people who do not seek treatment, 19 which may lead to even more frequent prescriptions of psychotropic medications for treatment seekers.
Current Study
The current study measures psychotropic medication prescription rates at CBT immersion obesity treatment sites across multiple geographical regions in the United States and United Kingdom. This study also attempts to evaluate the potential influence of psychotropic medications on treatment process and effectiveness. We offer the following hypotheses:
(1) Psychotropic prescription rates will be higher in the United States than in the United Kingdom. (2) Participants taking psychotropic medications will exhibit equal weight reduction from pre- to post-treatment as their nonmedicated peers. (3) Participants taking psychotropic medications will report greater psychological distress pretreatment, but will exhibit equal or greater reduction in psychological distress during treatment than their nonmedicated peers. (4) Participants taking psychotropic medications will engage in treatment at similar rates as their nonmedicated peers.
Methods
Participants
Participants were attendees of therapeutic weight-loss camps operated by Wellspring Camps in North Carolina, Washington DC, Florida, Georgia, California, New York, Pennsylvania, Texas, Wisconsin, and the United Kingdom during the summer of 2012. A total of 642 campers participated in the study, 69.0% female, 30.7% male, and 0.3% did not report a gender. Table 1 presents camp attendance by location and gender. Not all camps collected data on race and ethnicity. Of those that did (N = 255), 73.3% of the participants reported that they were white, 10.2% African American, 6.3% Hispanic, 2.0% Asian, and 8.2% “other.” Only campers <19 years of age participated. Mean age = 14.85 (SD = 20.08); initial BMI = 34.51 (SD = 6.96); initial percent overweight = 74.86% (SD = 35.29%); and mean number of weeks attended = 5.06 (SD = 2.28) ranging from 3 to 10 weeks. Four hundred ninety six participants (77.3%) took no psychotropic medication (ADHD stimulants nor mood regulating medications). One hundred twenty eight participants (20.0%) took mood regulating medications. Eighteen (2.8%) participants took only ADHD stimulant medication, and 39 (6.1%) took both ADHD and mood regulating medications.
Participants by Gender and Camp Location
Wellspring camps' immersion program
Wellspring's approach to weight loss and healthy lifestyle change focused on several key ingredients.5,8 These included consistent self-monitoring of all food consumed and all physical activity, the use of a very low fat diet, the planning and execution of target behaviors to reach a healthy goal, and long-term social support to promote adoption of the program at home. While at camp, participants attended four CBT sessions per week (two individual, two group), weekly nutrition and culinary education, and substantial daily physical activity. Camp clinical staff (therapists and clinical directors) were trained at several sites by an experienced clinical psychologist, the second author, who designed the program. Staff received a 240-page spiral bound book that outlined the rationale for all aspects of the program, as well as electronic copies of about 100 handouts; staff were also provided with the books used by all campers; and staff were also required to answer accurately dozens of detailed questions about the materials and the approach (generally amounting to a 30+ page set of responses). Thus, clinical staff were trained to conduct individual and group sessions according to the treatment program in a consistent manner. This supervising psychologist and another experienced therapist engaged in weekly phone and/or in-person supervision of camp clinical staff at every location, as well as in-person visits throughout the summer (including sitting in on numerous group sessions), to ensure that the immersion treatment program was being conducted properly at all treatment sites.
Materials
Informed consent
In precamp paperwork, parents signed informed consent forms that provided permission for Wellspring researchers to include their children's data at camp and at follow-ups in evaluation studies. In addition, this study was approved by an Institutional Review Board in Wellspring's parent company, CRC Health Group. All data were coded to prevent identification of individual campers' identities throughout the research process. Parents and children's physicians provided data about all medications, as well as demographic information.
Height and weight
During camp, camp staff completed weekly weigh-ins to measure weight and they measured height pre- and postcamp. Due to the limitations of using BMI with children and adolescents, percent overweight was used to define and measure weight change. Percent overweight was calculated as:% overweight = ([BMI/50th percentile BMI]–1)*100.8,20
Treatment Engagement/process measures
Engagement in treatment was defined by therapist-recorded number of days the campers self-monitored each week, average number of steps per week, and the average number of written comments in self-monitoring journals.
Clinical assessment of depression
The Clinical Assessment of Depression (CAD) is a 50-item self-report questionnaire. Its structure parallels the criteria for depression defined by the DSM-IV-TR 21 for children, adolescents, and adults. The total score, a standardized score with a mean set at 50, provides a valid measure of psychological distress for ages 8–79 years. 22 In past studies, the CAD has exhibited good test-retest reliability (r = 0.96) and also been validated in samples similar to that of the current study. 23
Procedure
Participants and parents completed informed consent followed by the demographic questionnaires and medication information before attending camps. Throughout camp, medical staff confirmed and managed participant's medications. The researchers coded the medications using the National Alliance on Mental Illness (NAMI) list of Commonly Prescribed Psychotropic Medications. 24 Medications and supplements (214 agents in total) were initially coded as “psychotropics” or “other/nonpsych” (e.g., allergy medications, analgesics). This differentiated those medications that were prescribed for psychological uses. Researchers further classified the medications in the “psychotropics” category into ADHD stimulant medication and non-ADHD “mood regulating” medication categories. With input from an experienced psychologist, two graduate student researchers reviewed every case and formed consensus on the categorization. This procedure placed all campers in one of four medication categories: no psychiatric medication, mood regulating psychotropics, ADHD stimulants, and a combined mood regulating/ADHD medication group.
Within the first 24 hours of camp attendance, participants completed the first CAD and had their height and weight measured by camp staff. Weight was measured weekly by trained camp staff. Height was measured a second time during the final week of camp. Finally, participants completed the CAD a second time within 24 hours of the end of camp.
Statistical Analyses
Statistical analyses were performed with SPSS version 22. The relationship between geographical camp location and medication use was analyzed with a chi-square. Potential gender differences were analyzed with t-tests. Two repeated measures ANOVAs and a MANOVA were utilized to test the relationships between treatment completion and weight changes, psychological distress, and engagement in treatment, respectively.
Weight status was operationalized as percentage overweight, but due to the importance of accurately representing weight status in the current study, preliminary analyses, including weight, were performed again with additional measures of this variable. Two analyses, one utilizing simple BMI and one BMI standard deviation scores, revealed no significant differences compared to the analysis using percent overweight. Therefore, results utilizing percent overweight are presented. Due to the likelihood of ADHD stimulant medications reducing appetite, 25 participants taking only these medications (2.8%) were removed from primary analyses. Those taking both ADHD stimulant medications and mood regulating medications (6.1%) were placed in the “psychotropic” medication group. This resulted in two medication groups used for statistical analyses, those who did not take any psychotropic medications (mood regulating nor ADHD), n = 496 (79.5%), and those who did take mood regulating psychotropics (regardless of ADHD stimulant medication status), n = 128 (20.5%). To confirm that inclusions of participants taking both mood regulating and stimulant ADHD medications in the “psychotropics” group did not affect results, all primary analyses were conducted excluding any participant taking an ADHD stimulant medication. These sets of analyses showed no significant differences. Therefore, participants taking both mood regulating and ADHD medications were left in the “psychotropics” group to improve generalizability and statistical power.
Results
Medication Use
Hypothesis one was supported. Rates of psychotropic medication use varied greatly across camps, χ2(9, N = 623) = 28.23, p = 0.001. Post hoc Z-tests revealed statistically significant differences between the UK camp and all US camps, as well as smaller individual differences among the US camps (Table 2 and Fig. 1, different superscript letters indicate that groups differ at p < 0.05). The highest rates of psychotropic medication use were found in Wisconsin (32.0%), North Carolina (27.5%), San Diego (26.3%), and New York (25.3%). The lowest rates were found in the United Kingdom (2.6%), followed by Texas (12.1%), Georgia (15.8%), and Florida (16.7%). In support of the first hypothesis, all US camps had statistically significantly higher usage of psychotropics than the UK camp (2.6%). Even the US camp with the lowest usage, Texas (12.1%), showed far greater rates than the campers in the United Kingdom (2.6%).
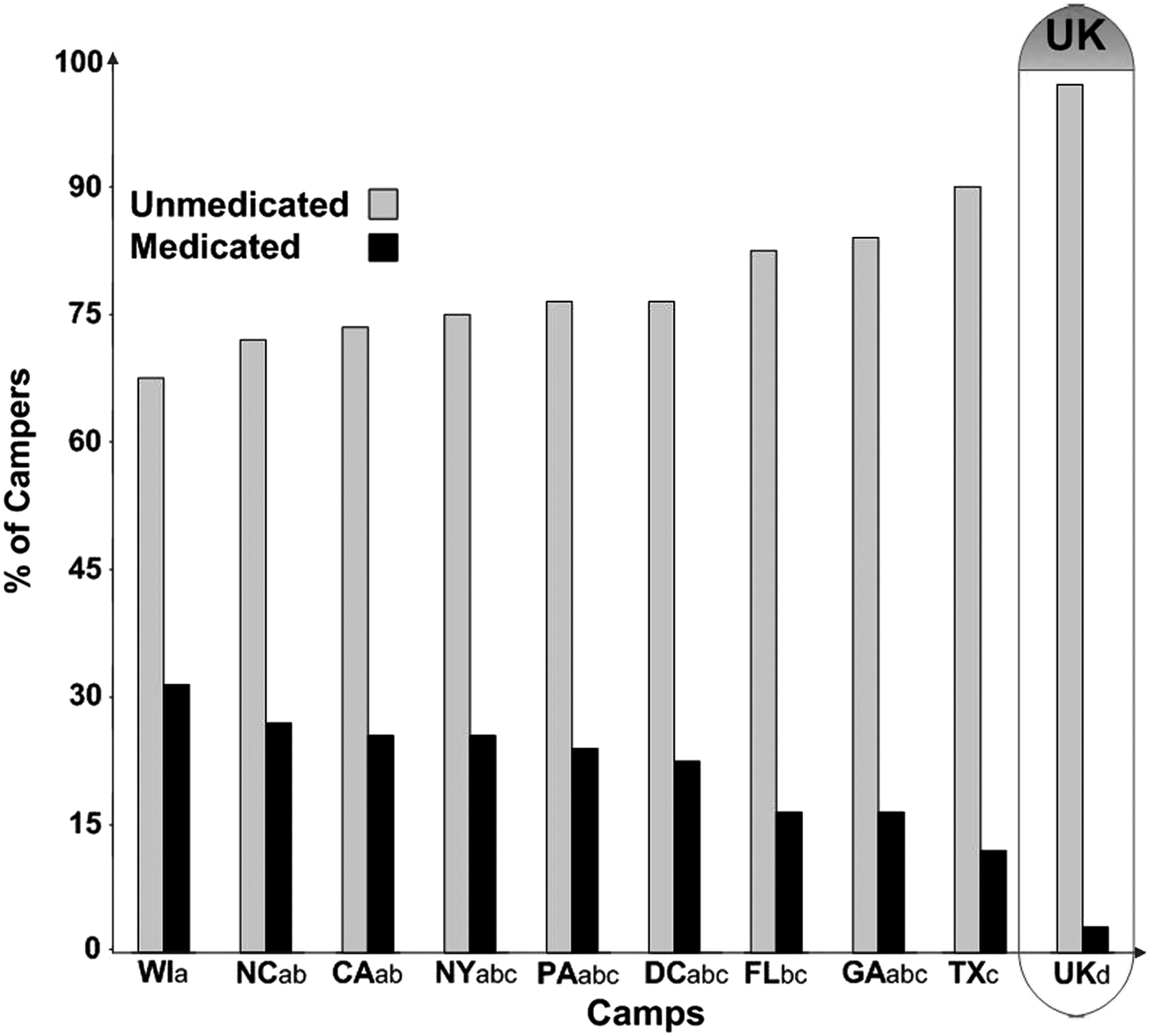
Medication Group by Camp Location. WI, Wisconsin; NC, North Carolina; CA, California; NY, New York; PA, Pennsylvania; DC, Washington DC; FL, Florida; GA, Georgia; TX, Texas; UK, United Kingdom. Different superscript letters indicate that groups differed at p < 0.05.
Psychotropic Medication Use by Camp; n (%)
Different superscript letters indicate that groups differ at p < 0.05.
Gender
In the current study, gender had the potential to exhibit important differences on study variables and the potential to influence the primary analyses. Independent samples t-tests revealed that depressive symptoms did not significantly differ between males and females precamp (males M = 49.01, SD = 10.90, females M = 49.23, SD = 10.69), t(320.44) = 0.22, p = 0.827, postcamp (males M = 44.36, SD = 9.97, females M = 44.33, SD = 8.73), t(280.89) = −0.29, p = 0.977, or depressive score change scores from pre- to postcamp (males M = −4.85, SD = 8.26, females M = −4.87, SD = 7.65), t(285.46) = −0.03, p = 0.980. Genders differed modestly on treatment engagement variables of self-monitored food intake (males M = 70.86%, SD = 25.49, females M = 80.95%, SD = 18.84), t(289.72) = 4.95, p < 0.001, average words per week in journal (males M = 173.55, SD = 390.86, females M = 89.91, SD = 128.85), t(208.149) = −2.89, p = 0.004, and average steps per day (males M = 22443.91, SD = 7415.95, females M = 21139.26, SD = 4433.18), t(248.32) = −2.250, p = 0.025. The medicated and nonmedicated groups did not have different percentages of male and female participants, χ2 (1, N = 494; Table 3) = 0.84, p = 0.358. Preliminary analyses conducted with genders separated did not differ significantly from analyses with genders combined. Therefore, data from genders combined are reported.
Baseline Characteristics; M(SD)
p < 0.01.
CAD, clinical assessment of depression.
Weight Changes
Hypothesis two was supported. Across all camps, from the beginning of camp to the end, participants' percent overweight decreased dramatically from 74.76% (SD = 34.97%) to 56.11% (SD = 29.68%), an average reduction of 18.65% overweight (Table 4). Participants taking and not taking psychotropic medications did not differ in percent overweight at baseline, t(618) = 0.308, p = 0.758. Participants lost a significant amount of weight from pre- to postcamp, F(1,617) = 1299.17, p < 0.001,
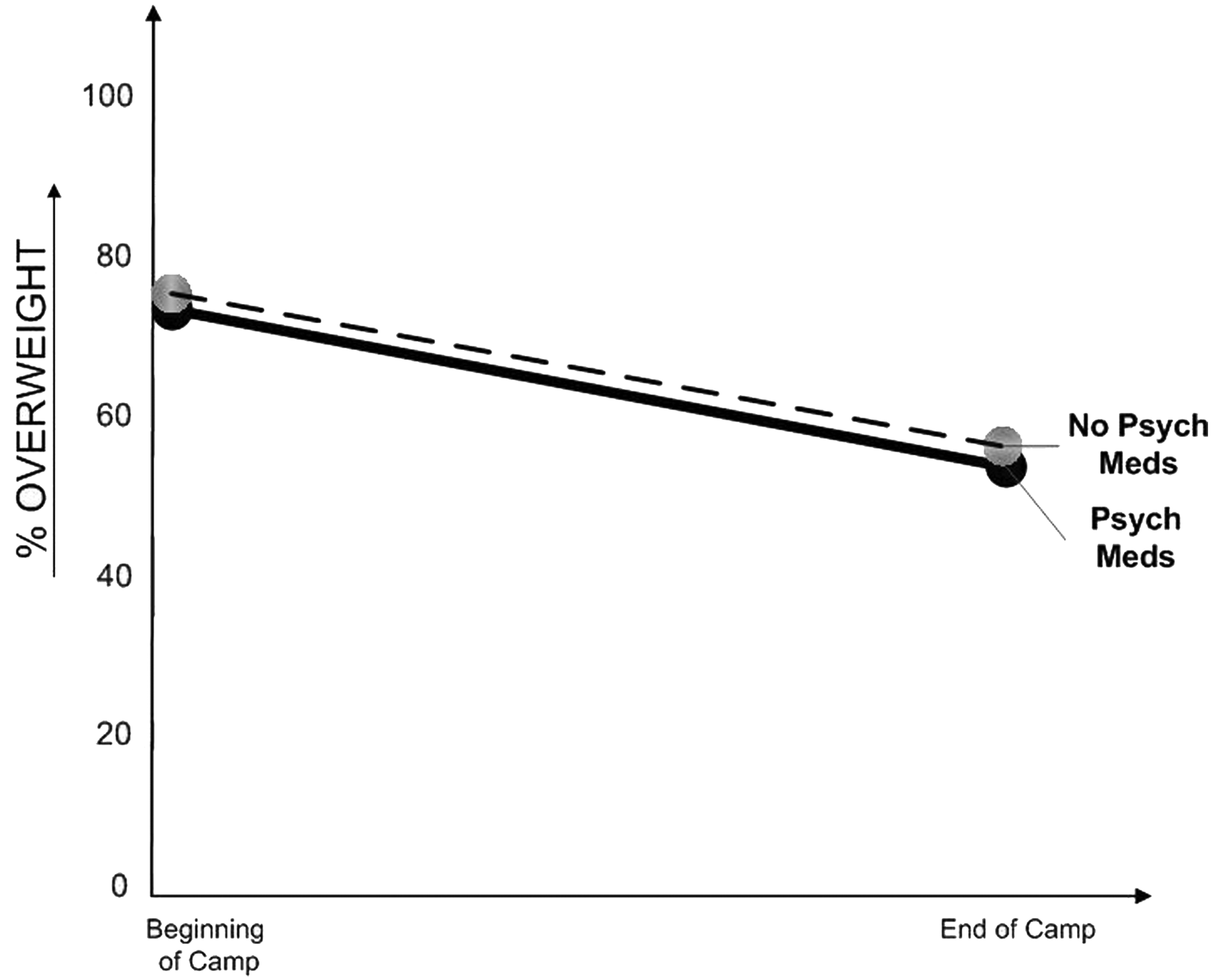
Percent Overweight by Pre-Post Camp and Medication Group.
Percent Overweight Pre- and Postcamp by Psychotropic Medication Status
Different superscript letters indicate that groups differ at p < 0.05.
Psychological Distress
Hypothesis three was supported. Participants' CAD scores decreased significantly from 49.21 (SD = 10.73) at the start of camp to 44.24 (SD = 9.07) at the end of camp, F(1, 537) = 196.38, p < 0.001,
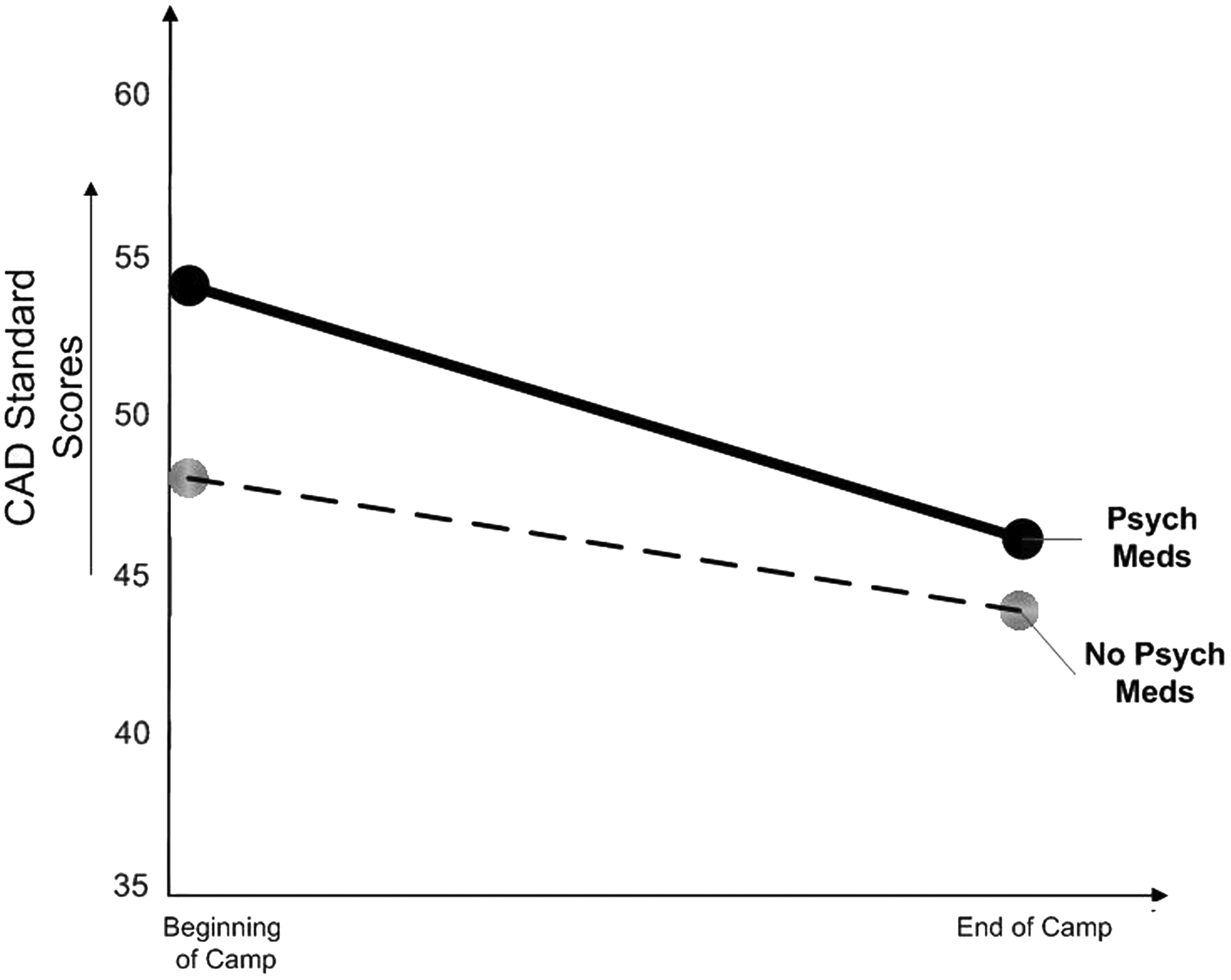
CAD by Pre-Post Camp and Medication Type. CAD, clinical assessment of depression.
CAD Score Pre- and Postcamp by Psychotropic Medication Status
Different superscript letters indicate that groups differ at p < 0.05.
Engagement in Treatment
Hypothesis four was supported. To test this hypothesis, we computed a MANOVA with Medication group as the independent variable and self-monitoring consistency, journaling, and step counts as the dependent variables. As hypothesized, this analysis revealed no significant differences between Medication and No Medication groups, F = 0.69, p = 0.559,
Geographical Differences in Medication Prescription Rates
The drastic differences in psychotropic medication use between geographic locations merited further analyses regarding reported levels of psychological distress. Therefore, we compared pretreatment CAD scores between the United States (M = 48.86, SD = 10.80) and United Kingdom (M = 51.19, SD = 10.21), revealing no significant differences, t (572) = −1.75, p = 0.08, d = 0.147. We also used a 2 (Camp: US, UK) × 2 (Time: pre vs. post) ANOVA. This analysis revealed that the campers from the United States and United Kingdom exhibited equivalent reductions in psychological distress from pre- to postcamp, Time F(1,554) = 100.27, p < 0.001,
Discussion
The first aim of the current study was to measure the prevalence of psychotropic medication use in a sample of obese youth seeking immersion weight-loss treatment. Results revealed that rates of psychotropic medication prescription differed greatly across geographic locations. More specifically, almost 10 times as many campers in camps in the United States (22.3%) used psychotropics compared to those in the United Kingdom (2.6%). This result should be interpreted in the context of greater overall psychotropic prescription rates to all adolescents in the United States compared to the United Kingdom. 26
The second aim was to determine if campers who took psychotropic medications differed from unmedicated campers in terms of weight change, psychological distress, or engagement in treatment. Results revealed that psychotropic medication use was not related to treatment engagement or treatment effectiveness. Psychotropic use was related to higher ratings of pre- and post-treatment psychological distress, but by the end of camp, participants taking psychotropic medications decreased these relatively distressed mood ratings more than those not taking these medications—without changing their use of medications during camp.
CBT immersion obesity treatment appears equally effective at reducing percent overweight for adolescents who take psychotropic medication as it is for those who do not. It appears effective at reducing psychological distress among youth taking psychotropic medication. Although data comparing psychotropic prescription rates between obese and nonobese adolescents are limited, 12 especially in the United States and United Kingdom, the existing data and current results reveal an interesting pattern. Not only are psychotropic prescription rates among adolescents increasing in recent years according to prior research,27,28 but the present results suggest that healthcare providers appear to prescribe these medications to obese adolescents at much higher rates in the United States. In the current sample, obese adolescents in immersion treatment received prescribed psychotropic medications at far higher rates than the best available estimates for their normal weight peers. 12 More specifically, based on a nationally representative sample from 2005 to 2010 (i.e., a sample that included both normal weight and overweight teens), average usage of psychotropics by teenagers in the United States was 6.0%. 29 That's almost three times higher usage than we observed for campers (in 2012) from Wellspring UK; campers from the United States (also in 2012) averaged 3.7 times higher rate of usage than average teenagers in the United States. Despite these drastic differences between Wellspring UK and Wellspring USA, adolescents engaged in treatment equally and saw similar results in weight and mood improvement. These results lend themselves to several possible interpretations and important avenues for future research.
Psychotropic Medications and Behavioral Treatment Outcomes
The only differences between the Medication and No Medication groups in this study were modest differences in reported levels of psychological distress at the beginning of camp and an even smaller difference at the end of camp. The Medication group's psychological distress decreased more than the No Medication group's, possibly due to treatment having a greater effect on those with higher distress or possibly due simply to higher scores having greater range to decrease. This result suggests that many of the medicated adolescents may have demonstrated more distress in their everyday lives before treatment. This in turn would make them more likely to receive a psychotropic medication prescription 11 due to evidencing emotional distress and obesity. This is problematic given the lack of efficacy of medications for less-than-severe depression 13 and the association of these medications and side effects such as weight gain and sedation.15–17
The current study did not include measurement of prepsychotropic medication mood assessment due to the fact that, in most cases, the participants had been taking the psychotropic medication for a significant amount of time before participating in the study. Therefore, we are unable to assess the effects of the medications on the obese adolescents' moods. It is possible that the current study suffers from sampling bias in that it may be missing a significant number of depressed obese adolescents who did not receive psychotropic medication and were therefore less likely to attend treatment. Perhaps regions with lower psychotropic prescription rates simply missed these adolescents. This possible explanation implies that psychotropic medications were effective for obese adolescents suffering from emotional distress, which in turn resulted in medicated and nonmedicated campers attending treatment and evidencing similar mood and response to treatment. However, the pattern of results of the current study, specifically the drastic differences in psychotropic prescription rates without notable effect on treatment process or outcome, questions this sampling bias explanation. Certainly psychotropic medications helped improve some of the more significantly depressed participants' moods, perhaps enabling them to attend immersion treatment. However, given the relatively low distress reported by all participants, this explanation does not account for the greater than 10-fold difference in prescription rates across geographical regions without effect on treatment.
Although more research is needed before drawing firm conclusions, a probable explanation of the current results is that in the United States, obese adolescents are more likely to be perceived as being depressed and receive psychotropic medications ostensibly to treat their depressed mood and/or their obesity. The current results also suggest behavioral therapies for weight loss as efficacious regardless of medication status. Given the apparent weight-related prescription bias, 11 the problematic side effects,15–17 and the lack of efficacy for mild to moderately depressed mood, 13 behavioral interventions should be utilized more frequently.
Limitations of This Study
This study does have some notable limitations. Despite the evidence that psychotropic medication use was unrelated to mood improvement and weight loss, we cannot infer causality due to the lack of experimental methodology. Because we do not have data on the participants before they began their psychotropic medication regimen, we cannot rule out potential improvements in moods due to the medications before camp and during camp. Those potentially enhanced moods may have allowed some campers to fare as well as their unmedicated peers. 12 It is also possible that the relatively mild depressive symptoms observed in the current sample of participants taking psychotropic medications were mild because their medications had effectively reduced previously high levels of depression. In addition, the current data were collected in a specialized immersion treatment environment and may not generalize to noncamp, routine outpatient environments. In addition, although the sample size of the current study was quite large, it was not large enough to allow for comparisons to be made among specific psychotropic drug classes (e.g., antidepressants vs. antipsychotics vs. combination of the two) or types (e.g., S.S.R.I. vs. S.N.R.I. medications). A more detailed analysis of drug class and type could determine if these various medications differentially affect the impact of treatment for obese youth. Finally, a minor limitation, due to hand scoring during clinical use, is that only CAD total scores were reported to the researchers. Therefore, the internal consistency reliability of the CAD in the current sample could not be computed.
The current study leads to several important avenues for future research. First, long-term follow-up data from the current sample could provide information regarding potential differences (or lack thereof) between the participants taking versus not taking psychotropic medications over time. To truly test the effects of psychotropic medications, a randomized-controlled trial (RCT) would prove informative. Ideally, this RCT would obtain a sample of obese youth who used psychotropic drugs. It would then randomly assign them to one of two conditions, a condition in which they engage in immersion CBT while remaining on the psychotropic medications, and one in which they stop taking these medications. This would allow for powerful conclusions to be drawn about the effects of psychotropic medications in relation to weight loss and mood among obese youth. This RCT would also have at least a 1-year follow-up beyond the initial immersion treatment experience. To further explore and generalize the results beyond the current population of immersion treatment, similar studies are needed in outpatient samples. The number of adolescents receiving immersion treatment is relatively small, and due to its intensity the effects of immersion treatment are likely larger than outpatient treatments. For these reasons, it would prove useful to examine outpatient samples for differential use of psychotropic medications and interaction with outcomes.
Conclusions
Psychotropic medication prescription rates among obese adolescents appear to differ significantly across geographical regions, especially comparing the United States to the United Kingdom. These prescription rates were unrelated to process and outcomes of CBT immersion obesity treatment among adolescents. Immersion treatment for obese adolescents appears to result in significant weight reduction and mood improvement regardless of psychotropic medication status. This finding questions the use of psychotropic medication at the observed rates in some regions and supports the use of cognitive behavioral immersion treatments for adolescent obesity.
Footnotes
Acknowledgments
The authors gratefully acknowledge the valuable contributions of Zac Bruback to this project, particularly for his contribution to the development of an effective method to classify medications. The cooperation of the camp directors and clinical staff at Wellspring's camps in 2012 is also very much appreciated.
Everyone who contributed significantly to the work is listed as an author.
Author Disclosure Statement
Drs. Krawczyk, Kirschenbaum, and Caraher have nothing to disclose.