
Abstract
Abstract
Background:
While short and poor quality sleep have been associated with childhood obesity, no known studies have examined social jetlag. Social jetlag is the discrepancy between an individual's circadian clock and social rhythms, and is measured as the difference in hours between the midpoint of sleep during work/school days and on free (weekend) days. This study investigated the independent associations between sleep duration, sleep disturbances, and social jetlag with adiposity in children.
Methods:
A cross-sectional study, including 341 children (50% female) aged 8–10 years. Five dependent variables: body fat (%), fat mass (kg), fat mass index (FMI, kg/m2), waist to hip ratio, and body mass index (kg/m2). Three independent variables: average sleep duration, sleep disturbances, and social jetlag.
Results:
Following adjustment for confounders, sleep duration was not associated with any variable, and sleep disturbances were associated with FMI (β = 0.047, 95% CI: 0.002, 0.093 kg/m2), while social jetlag was associated with all five adiposity variables, including an absolute 3% greater body fat (β = 2.963, 95% CI: 0.40, 5.53%) per 1 hour of social jetlag.
Conclusions:
Social jetlag may be an important and measurable public health target in children.
Introduction
Short and poor quality sleep, along with physical inactivity and poor diet, have been associated with childhood obesity.1–3 Several aspects of sleep may be important, including sleep disturbances, sleep duration, and social jetlag. Social jetlag is the discrepancy between an individual's circadian clock and social rhythms, and is measured as the difference in hours between the midpoint of sleep during work/school days and on weekend free days. 4 Studies have reported an association between sleep disturbances and obesity in children.2,5 Similarly, a recent meta-analysis of 11 longitudinal studies (total n = 24,821 participants) reported that children sleeping for a short duration, defined as 30–60 minutes less than a “long” duration, had twice the risk of being overweight/obese (2.15, 95% CI: 1.64–2.81). 1 However, the importance of social jetlag in children is unknown. In adults, social jetlag has been associated with obesity,6,7 with one longitudinal cohort study, including 815 non-shift workers, reporting that each hour of social jetlag was associated with a 0.10 kg (0.48) increase in fat mass and 0.12 kg/m2 (SE: 0.24) increase in body mass index (BMI). 6 Similarly, at least one study of 77 adolescents has reported an association between social jetlag with BMI and waist-to-hip ratio (WHR). 8 However, while previous studies have investigated the association between sleep timing and adiposity among children,9–11 no known studies have specifically examined social jetlag, nor has any study simultaneously examined the importance of sleep duration, sleep disturbances, and social jetlag.
Sleep–wake and metabolism cycles are regulated by the circadian clock. 12 In modern society, the rhythmicity of the circadian clock is often disrupted by social obligations, including work and school schedules. 13 Social jetlag is simple to measure, and may be a simple target for public health policy. However, while national guidelines in New Zealand 14 and Canada 15 recommend that children aged 6–13 years sleep for 9–11 hours and that bed and wake-up times should be consistent, the evidence for regulating the sleep–wake cycle is limited. This study investigated whether sleep duration, sleep disturbances, and social jetlag are independently associated with adiposity in preadolescent children.
Methods
Study Design
This cross-sectional study was carried out in accordance with STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 16 Details of the wider study, Pre-Adolescent Cardio-Metabolic Associations and Correlates (PACMAC), have been previously published. 17 Adiposity was assessed in the schools between the hours of 9:00 and 12:00. Participants were asked to ensure adequate hydration, but fast for at least 3 hours, and refrain from exercise for 24 hours. Within 7 days of the adiposity assessments, sleep habits and demographic data were collected using a questionnaire completed at home by the primary caregiver. Only children with complete adiposity and sleep data were included in the analyses.
Participants
Children aged 8–10 years were recruited from schools in three major cities across New Zealand (Wellington, Christchurch, and Dunedin), between April 2015 and April 2016 (Fig. 1). For each region, schools were stratified by socioeconomic status (SES) and randomly invited to participate. All children were eligible to participate unless they had an orthopedic injury/surgery that prohibited full function within the previous 4 weeks or were prescribed any cardiovascular medications. Parental or guardian consent and child assent were obtained before participation, in accordance with the requirements of the New Zealand Health and Disability Ethics Committees (HDEC:14/CEN/83).
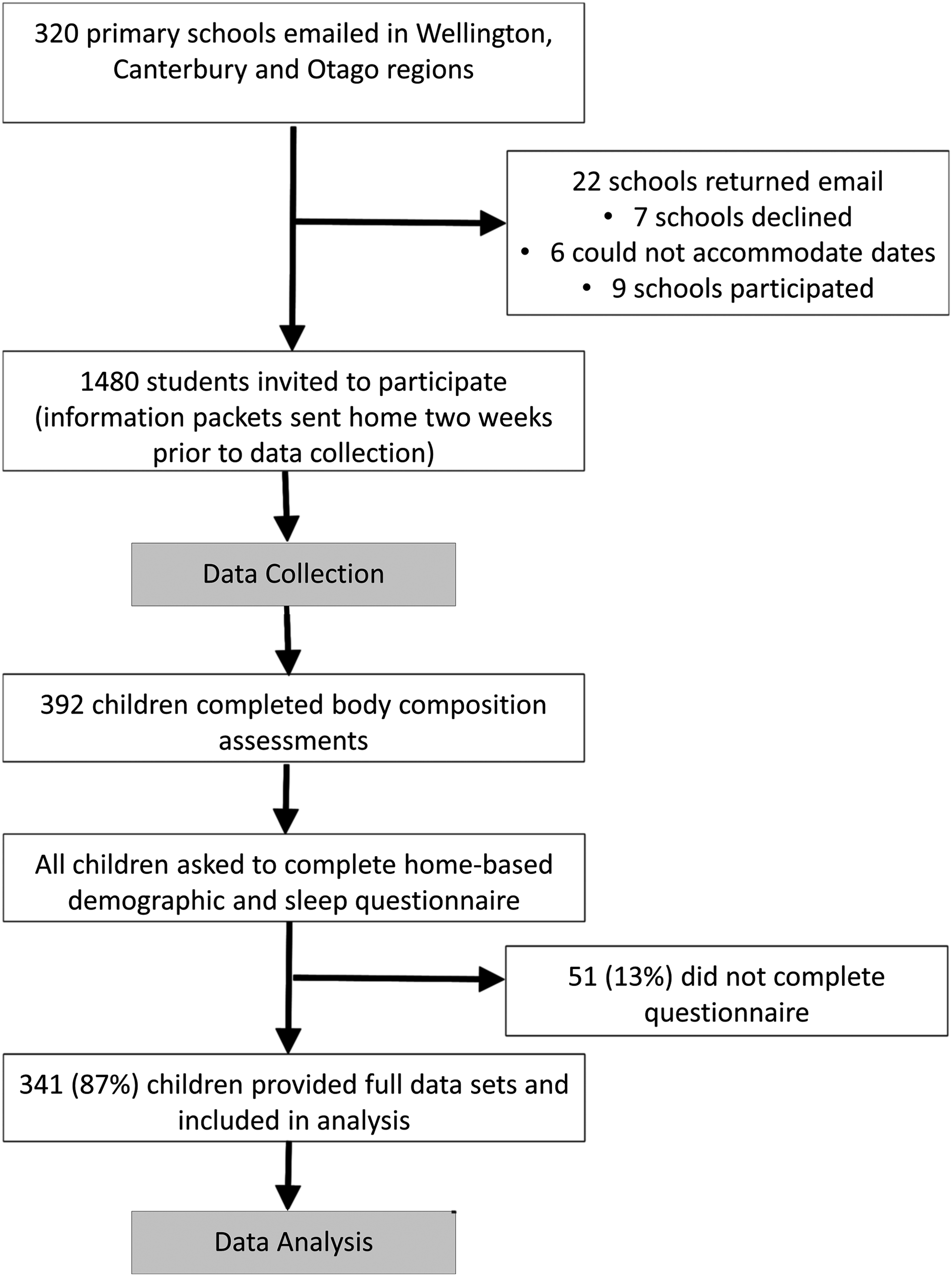
Participant recruitment flowchart.
Demographics
Demographic data collected included date of birth, sex, ethnicity, and school address. The school address was used to determine school decile rating, an SES indicator of the school. The decile is based on the proportion of students at the school with low SES as defined by the student's residential address. Decile 1 includes the 10% of schools with the highest proportion of students from low SES communities, decile 10 being the lowest proportion. School decile was divided into “Low” (Deciles 1–5) and “High” (Deciles 6–10).
Sleep Behaviors
Three variables were measured: average sleep duration, sleep disturbances, and social jetlag. To determine average sleep duration and social jetlag, the participant's primary caregiver was asked to report what time their child usually went to bed and what time they usually got up on both school days and free (weekend) days. Single items of habitual school/weekday sleep show reasonable concurrent validity with actigraphy and diary data. 18 Average sleep duration was calculated using a ratio of five weekdays to two weekend days. Social jetlag was calculated as the absolute difference between the midpoints of sleep on weekdays versus weekend days. 7
Sleep disturbances were estimated by having parents complete the Children's Sleep Habits Questionnaire (CSHQ). The CSHQ demonstrates adequate internal consistency, acceptable test–retest reliability, and discriminant validity. 19 The 33 questions were answered on a 7-point Likert scale from Always (1) to Never (7), with higher scores indicative of greater sleep disturbances. The CSHQ includes eight subscales that align with the key sleep complaints relevant for this age group: bedtime resistance, sleep onset delay, sleep duration, sleep anxiety, night waking, parasomnia, sleep-disordered breathing, and daytime sleepiness. A Total Sleep Disturbance score was calculated as the sum of all 33 scored CSHQ questions, with a potential range of 33–99. A Total Sleep Disturbances score >41 was used to indicate disturbed sleep, as this cutoff has been shown to accurately identify 80% of children with a clinically diagnosed sleep disorder. For this study, only the Total Sleep Disturbance score was used. 19
Adiposity
Five dependent variables were recorded: body fat (%), fat mass (kg), fat mass index (FMI, kg/m2), WHR, and BMI (kg/m2). Body fat (%) and fat mass (kg) were measured using multifrequency bioimpedance analysis (BodyStat Quadscan 4000, Isle of Man, United Kingdom). The instrument was calibrated in accordance with the manufacturer's instructions and measurements were conducted according to standardized procedures. 20 Participants were studied in the supine position on a nonconductive surface, with arms and legs abducted at a 30°–45° angle from the trunk to avoid medial body contact by upper and lower extremities. FMI was calculated by dividing fat mass (kg) by height squared (m2).
To calculate the anthropometric indices (BMI and WHR), height was measured with a calibrated portable stadiometer (Seca, Germany), with shoes and socks removed and head in the Frankfort plane. Using a nonelastic tape (Seca, Germany), the waist circumference was measured during mid-expiration at the midpoint between the lower costal margin and the level of the anterior superior iliac crest, and hip circumference was measured around the widest portion of the buttocks. Age- and sex-specific BMI z-scores were calculated using the 2007 World Health Organization (WHO) method, 21 and BMI values were categorized using the International Obesity Task Force sex- and age-dependent cutoff points. 22
Statistics Analyses
Statistical analyses were performed using Statistical Package for Social Sciences version 22 (SPSS, Inc., Chicago, IL). Only participants who had complete data for all sleep and all adiposity variables were included in the analyses. Linear regression analyses were performed using Gaussian family generalized estimating equations with robust standard errors to allow the clustering in data among students attending the same schools, 23 to ensure results are representative of the population in the sampled area. Each analysis included one dependent variable (body fat%, fat mass, FMI, WHR, or BMI) and all three independent variables (sleep duration, social jet lag, and sleep disturbances). For each analysis, the influence of confounding variables was assessed by fitting two models, with Model 1 adjusting for school clustering only. Model 2 was additionally adjusted for age, sex, ethnicity, and school decile rating. Model 3 included the relevant sex interaction terms. All regression models were assessed by examination of the model residuals plotted against their normal scores. Anonymized data will be shared on reasonable request.
Results
Of the 392 participants who took part in the PACMAC study, 341 had complete adiposity and sleep data (Fig. 1). The 341 children included in this study were comparable to the full 392 participants (9.54 years, 50% female, 29% overweight, and 54% low decile school). Table 1 presents the demographic characteristics of the participants included in this analysis. Among the 341 participants, 29% were classified as overweight and 40% had disturbed sleep. The majority of participants (92%, n = 315) slept for at least 9 hours each night, and on average, the total sleep duration did not differ for the week compared to the weekend (10.1 hours vs. 10.1 hours, p = 0.490). However, all, but two children went to bed later on the weekend (mean: 42 min, 95% CI: 44, 50), and 97% (n = 330) awoke later on the weekend (42 min, 95% CI: 37, 46). As a result, the average social jetlag was 43 min (95% CI: 40, 47), and 35% had ≥1 hours of social jetlag.
Characteristics of Participants, Stratified by Sex
Univariate Models
The univariate outcomes are shown in Table 2. Sleep duration was associated with fat mass (p = 0.022), BMI (p = 0.018), and WHR (p = 0.025), sleep disturbances with fat mass (p = 0.010), FMI (p = 0.009), and BMI (p = 0.019), and social jetlag with all five adiposity variables (p = < 0.001–0.008).
Linear Association between Body Composition Measures and Sleep Measures
Model 2: school decile, ethnicity, sex, age.
Note: the univariate models specify the sleep measures (sleep duration, sleep disturbances, and social jet lag) separately (separate models). The multivariate models include all sleep measures in the same model.
Multivariate Models
Multivariate models 1–2 are shown in Table 2. When adjusted for confounders (Model 2), sleep duration was not associated with any sleep variable and sleep disturbances were associated with FMI (p = 0.041), while social jetlag remained associated with all five adiposity variables (p = 0.010–0.033). One hour of social jetlag was associated with a 3% increase in body fat, a 1.73 kg increase in fat mass, a 0.76 kg/m2 increase in FMI, a 0.89 kg/m2 increase in BMI, and a 0.13 (ratio) increase in WHR.
Sensitivity Analysis: Sex Interaction
Model 3 included the sex interaction term (data not shown). The interaction term was only significant for the associations between sleep duration and sleep disturbances with WHR. When stratified by sex, the association between sleep duration and WHR was not significant for girls (β = −0.007, 95% CI: −0.015, 0.000, p = 0.053) or boys (β = −0.005, 95% CI: −0.015, 0.005, p = 0.360). Similarly, the association between sleep disturbances and WHR was not significant for girls (β = −0.001, 95% CI: −0.002, 0.000, p = 0.060) or boys (β = 0.001, 95% CI: 0.000, 0.002, p = 0.062).
Discussion
Following adjustment for potential confounders, sleep duration was independently associated with WHR and sleep disturbances were independently associated with fat mass and FMI, while social jetlag was independently associated with all five adiposity markers. The importance of the association between social jetlag and adiposity is strengthened when considering that 92% of the children did achieve, on average, the minimum nine hours of sleep recommended by the national guidelines in New Zealand, 14 and the findings were not confounded by different sleep durations on weekdays and free (weekend) days. Collectively, these findings suggest that social jetlag is at least as important as sleep duration and sleep disturbances in this age group.
Strengths and Limitations
This study had several potential limitations. First, the cross-sectional study design makes it difficult to interpret the temporal sequence and clinical importance of the absolute 3% greater body fat. Longitudinal studies are required to determine causality. Second, the use of parent-reported questionnaires may have led to some measurement and reporting errors. Nonetheless, the use of single item habitual school/weekday sleep survey shows reasonable concurrent validity with actigraphy and diary data. 18 Third, the CSHQ is a screening rather than diagnostic tool for sleep disturbances, and relies on parent self-report. Future studies would do well by incorporating objective measures of sleep quality. Fourth, this study might have been underpowered to detect a significant sex interaction as moderation analyses require substantial sample sizes. 24 Fifth, we adjusted our statistical models by using a school-level proxy of SES; further studies would do well to adjust using a family-level indicator of SES. Last, further study is required to generalize these findings to preadolescents in other nations. However, a major strength of this study is the relatively large and representative cohort of New Zealand-based preadolescents.
Comparison with Other Studies
While the univariate analysis confirmed previous findings, showing a negative relationship between sleep duration and increased adiposity, 1 and a positive relationship between sleep disturbances and increased adiposity,2,5 multivariate analysis revealed that only social jetlag was independently associated with all five estimates of adiposity. The findings are in agreement with a previous cross-sectional study of 77 adolescents, which reported a positive association between social jetlag with BMI and WHR. 8 Of particular note, the increase in fat mass and BMI per one hour's social jetlag was greater than that previously reported in 815 non-shift working adults [0.10 kg (SE: 0.48) and 0.12 kg/m2 (SE: 0.24), respectively]. 6 The aforementioned study in adults was longitudinal, strengthening the argument for causality.
In adults, social jetlag is thought to be influenced by an individual's chronotype, which refers to their biologically preferred time for sleep, with some people preferring to go to bed early and rise early and others preferring to go to bed later and rise later.4,13 An individual whose preference is to go to bed late and rise late may have their sleep truncated during the work week due to the need to rise in time for work. During the weekend, they then spend a longer time sleeping to recover from the sleep debt accrued across the work week as well as sleeping at more naturally preferred times. In studies of adults, both sleep duration25,26 and social jetlag6,7 have been independently associated with metabolic changes and adiposity. It is not clear, however, whether social jetlag presents the same way in younger individuals.
In this sample, the amount of sleep children obtained during the week, on average, was the same as that during the weekend. However, experienced social jetlag was, on average, 43 minutes, and was greater than one hour for 35% of children. This suggests that these children are shifting both their bedtimes and rise times between weekdays and weekends. Children of this age may be in a transitional developmental period where they can still fall asleep earlier on school nights, but are delaying their bedtimes and beginning to sleep in on weekends. This is in contrast to teenagers who become significantly more phase delayed and cannot fall asleep earlier on weekdays. 27
To maintain good metabolic health, the central circadian pacemaker in the suprachiasmatic nucleus must remain in synchrony with circadian rhythms in the peripheral organs. 28 Desynchrony between the central and peripheral clocks occurs when the timing of sleep is disturbed, and may also be possible when the timing of eating is altered, although we currently know very little about what happens to eating patterns when individuals experience social jetlag. This circadian desynchrony is thought to create disturbances in metabolic processes that are linked to weight gain.28,29 At present, our understanding of the biological mechanisms that link social jetlag to obesity are still limited, but the relationships are likely to be complex and involve both behavioral and biological components.
Policy Implications
Healthy dietary behavior and sufficient physical activity are entrenched aspects of obesity prevention, but the focus must also extend to good sleep behavior. Good sleep behavior, however, does not only pertain to the total duration of sleep but also entails, ensuring consistent sleep–wake cycles. To our knowledge, there is no evidence suggesting that an intervention altering the sleep times of children would have an effect on measures of adiposity. However, considering the potential for a relatively simple translation of social jetlag into a public health message, further longitudinal trials are warranted, which utilize objective sleep measures such as actigraphy. Further study is also warranted to determine the interactions with chronotype, nutritional behaviors, and metabolism in children. 28
Conclusions
Independent of sleep duration or sleep disturbances, one hour of social jetlag was associated with five measures of adiposity, including 3% greater absolute body fat. While further studies are required to confirm causality, these preliminary findings suggest that social jetlag may be an important and measurable public health target in children.
Footnotes
Acknowledgments
The authors would like to thank each child and their schools for willingly giving their time. Clinical Trial Registration: ACTRN12614000433606.
Author Disclosure Statement
No competing financial interests exist.