
Abstract
Abstract
Objective:
Executive and motivational dysfunction have been associated with pediatric obesity. Poor sleep quality and psychopathology, often comorbid with obesity, are also associated with executive and motivational dysfunction. We examined the contribution of these comorbid factors to the association between obesity and executive function and reward-related decision-making.
Methods:
Seven- to 18-year-old children with and without obesity performed a working memory task with low and high loads, a response inhibition task, and a probabilistic reward-related decision-making task. Parents filled out standardized measures of executive function in everyday behavior, sleep health, and psychiatric symptoms. Analyses controlled for age, gender, IQ, and parental education.
Results:
Children with obesity showed worse working memory performance under higher load (p = 0.007), and worse parent-reported behavioral regulation (p = 0.05) and metacognition (p = 0.04) in everyday behavior and their reward-related decision-making was less consistent with learned probabilistic conditions (p = 0.04). Response inhibition did not differ between groups. Children with obesity had worse parent-reported sleep health (p < 0.01) and 4.27 greater odds of clinically relevant internalizing symptomology (p = 0.03), both of which mediated the effect of obesity on behavioral regulation (p's < 0.01) and metacognition (p's < 0.01). Performance-based assessments were not associated with sleep health or psychopathology.
Conclusions:
Sleep quality and internalizing psychopathology were worse in children with obesity and contributed to parent-reported executive dysfunction in their everyday behavior. Performance-based measures of working memory and decision-making were not associated with those comorbidities of obesity.
Introduction
The role of cognitive processes such as self-regulation (termed executive function) and reward-related motivation in promoting and maintaining obesity is increasingly gaining recognition. 1 Obesity, observed in 20% of adolescents in the United States, 2 is associated with risk for medical comorbidities (e.g., cardiovascular disease and diabetes)3,4 as well as less academic achievement, 5 and psychosocial problems (e.g., discrimination and self-esteem). 4 Models of obesity posit that processes of executive function (i.e., inhibition and working memory) and motivation (i.e., reward sensitivity) are directly pertinent to food intake and nonhomeostatic eating.6–8 Indeed, children with obesity showed greater sensitivity to food rewards9,10 and reduced ability to inhibit prepotent responses to food stimuli11,12 and food intake13,14 relative to healthy weight children. However, differences may not be limited to food stimuli, as children with obesity showed higher sensitivity to reward15,16 and deficits in inhibitory control13,16 and working memory13,17 without food involvement. Such baseline cognitive impairments are concerning because of their impact on academic outcomes as well as their role in promoting obesogenic behavior.
In formulating a model about cognitive factors in obesity, it is important to note that executive and reward-related functioning are negatively impacted by psychopathology and poor sleep quality, common comorbidities of obesity. Inadequate sleep and poor sleep quality in children are associated with worse academic performance and executive function18,19 with sleep-disordered breathing, which is common in children with obesity, predictive of behavioral regulation problems longitudinally. 20 Independent of sleep quality, psychopathology has also been associated with executive dysfunction. 21 Furthermore, the two comorbidities have a bidirectional association in adolescents 22 and adults such that at 1-year follow-up, baseline anxiety and depression predicted new cases of insomnia and baseline insomnia predicted new episodes of anxiety and depression in adults. 23 While the causal pathways in the relationship between sleep, psychopathology, and cognition remain to be elucidated, sleep quality and psychopathology likely modulate decision-making and executive difficulties observed in pediatric obesity.
This study examined nonfood-related, reward-related decision-making and executive functioning in children with obesity and the contribution of sleep health and psychopathology. Reward-related decision-making was analyzed for both decision outcomes and underlying process parameters using Bayesian modeling, 24 while executive functioning was examined with tasks requiring reactive response inhibition, requiring cancellation of an action after it is planned (stop signal task [SST]), 25 dynamic working memory requiring trial-to-trial updating with load manipulation, 26 and with ecologically relevant assessment of regulatory and metacognitive executive difficulties using the Behavioral Rating Inventory of Executive Function (BRIEF). 27 Sleep quality, assessed by parent report of sleep health using the Children's Sleep Habits Questionnaire (CSHQ), 28 and psychopathology, assessed by parent report of symptoms of DSM-based psychiatric disorders using the Child and Adolescent Symptom Inventory (CASI), 29 were tested as potential mediators of deficits associated with obesity. Together, this study provides a comprehensive and nuanced examination of decision-making and executive functioning in pediatric obesity, with emphasis on contributions of sleep and mental health.
Methods
Participants
Participants included 112 7 to 18-year-old children, of which 105 provided parent reports of executive functioning and psychopathology, 78 performed the decision-making task, and 59 performed the response inhibition and working memory tasks, with partial overlap across the three samples (Table 1). Children were recruited through on-hold messages and flyers at Children's National Health System (CNHS) and neighborhood fairs. Informed consent and assent was acquired according to the Institutional Review Boards of Georgetown University and CNHS.
Demographic Characteristics, Executive Sample Is a Subset of Parent Report and Reward Samples
Data are presented as mean (SD) unless otherwise noted.
Fisher's test (cell n > 5) used to test group differences by sample: †p = .06; *p < 0.05; **p < 0.01; ***p < 0.001.
Sample completed the Behavioral Rating Inventory of Executive Function and Child and Adolescent Symptom Inventory.
Sample completed the BART.
Sample completed the N-back and stop-signal tasks.
Estimated from vocabulary and matrix subtest of the Wechsler Abbreviated Scale of Intelligence.
BART, Balloon Analog Risk Taking Task; CSHQ, Child Sleep Habits Questionnaire; SES, socioeconomic status.
Full-scale IQ 30 was lower in children with obesity (BMI ≥95th percentile) across all samples, while parental education, age, and gender differed between groups in at least one sample (Table 1). Exclusion criteria included a current medical diagnosis, including insulin resistance or diabetes, psychiatric diagnosis and/or prescription of psychotropic medication, and current or past history of neurological disorders.
Measures and Procedure
See Supplementary Data for task details (Supplementary Data are available online at www.liebertpub.com/chi).
Reward-related decision-making
The Balloon Analog Risk Taking Task (BART) 31 had 30 balloon trials. Participants were instructed to pump up balloons without popping them, winning 10 points for each successful pump, but losing all points following popping. Participants could save points and get the next balloon at any time. Unbeknown to participants, points saved were exchanged for $5 to ensure ethical treatment of participants.
Response inhibition
A visual SST 32 presented a fish (go stimulus) facing either left or right, to which participants responded with a button marked “L” or “R,” respectively. Participants were instructed not to respond if the white net appeared (stop signal), which was presented at a variable delay on 1/3 of the trials. The stop signal delay increased or decreased after each successful or unsuccessful stop, respectively, to maintain ∼0.5 probability of successful inhibition.
Working memory
Participants completed a letter N-back task with consonants only in two runs, 1-back and 2-back, in counterbalanced order. Participants were instructed to respond to serially presented consonants when the letter presented was the same as the letter presented in N trials previously (1-back: “R”-“L”-“L”; 2-back: “M”-“K”-“M”), with a greater working memory demand for 2-back than 1-back.
Parent-report questionnaires
A parent completed the BRIEF, 27 CSHQ, 28 and CASI. 29 The BRIEF provides T-scores (normed for age and gender; M = 50, SD = 10) for two indices: Behavioral Regulation Index (BRI; α = 0.94) and Metacognitive Index (MI; α = 0.96). Construct validity has been established for the BRIEF such that Child and Behavior Checklist (CBCL) subscales thought to reflect executive behaviors (e.g., Attention Problems and Emotional Control) correlate well with the BRIEF (r's > 0.50). The CSHQ characterizes behaviorally based sleep problems and provides estimates of hours slept per night and a total score, which encompasses bedtime habits, ability fall and stay asleep, and daytime sleepiness. Average CASI T-scores (normed for age and gender; M = 50, SD = 10) were calculated for Externalizing (Attention Deficit Hyperactivity Disorder, Conduct Disorder, and Oppositional Defiance Disorder; α's = 0.80–0.94) and Internalizing (Generalized Anxiety Disorder, Separation Anxiety, Major Depressive Episode, and Dysthymic Disorder; α's = 0.74–0.85) symptoms and categorized as Low Risk (T < 60) or At Risk/Clinically Significant (T≥ 60). Construct validity has been established for the CASI such that the CBCL Internalizing and Externalizing subscales correlate well with CASI subscales used in the Internalizing (r's > 0.50) and Externalizing (r's > 0.35) composites.
Statistical approach
Parental education was controlled for in all analyses with age and gender controlled for in-task performance outcomes as BRIEF or CASI indices are already normed for age and gender. Since intellectual functioning may contribute to variability in executive performance, IQ was controlled for in-task performance outcomes. Three types of models examined the effect of obesity status (obese vs. nonobese): (1) analyses of covariance for all task performance outcomes; (2) log-linked gamma generalized linear regression for nonparametric BART decision-making parameters; and (3) logistic regressions for CASI composites indices. Mediation analyses were modeled using adjusted bootstrapping percentile. 33
Results
Reward-Related Decision-Making
Groups did not differ on average number of pumps for balloons that did not pop (F(1, 66) = 1.42, p = 0.24, ηp
2
= 0.02) or the number of balloons popped (F(1, 66) = 2.33, p = 0.13, ηp
2
= 0.03; Table 2). As done in previous studies,34,35 a Bayesian learning model was used to assess decision-making,
24
with 92% of participants (36 obese, 36 nonobese) showing better fit, estimated by Bayesian Information Criterion, for the Bayesian model than a model assuming no learning (binomial test p < 0.01). There were no differences by obesity status for reward sensitivity (γ parameter; β(se) = 0.16 (0.15),
Group Differences in Task Performance and Parent-Reported Daily Executive Behaviors
Data are presented as mean (SD) and p-values reflect significance of 2-sample t-tests unless otherwise noted. N-Back p-values use Tukey adjustment for multiple comparison.
Mann-Whitney-Wilcoxon tests were used for all parameter estimates.
Mann-Whitney-Wilcoxon's difference in location.
Cohen's d for medians using pooled median absolute deviation.
RT, reaction time; SSD, stop-signal delay; SSRT, stop-signal reaction time.
Executive Functioning
Response inhibition
Stop-signal reaction time (SSRT), an estimate of the speed of the inhibitory process, and the stop-signal delay (SSD), the delay length for which a participant successfully inhibited responses 50% of the time, did not differ between groups (SSRT: F(1, 53) = 0.64, p = 0.43, ηp 2 = 0.01; SSD: F(1, 53) = 0.21, p = 0.65, ηp 2 < 0.01; Table 2), indicating that inhibitory control of prepotent responses was not affected by obesity.
Working memory
Group X Load (1-back vs. 2-back) analyses of variance were conducted for accuracy (mean percent correct target and nontarget responses) and reaction time (RT; Table 2). For accuracy, a significant effect of Load (F(1, 56) = 78.2, p < 0.01, ηp 2 = 0.45) showed worse accuracy for the higher (2-back: M = 84%, SD = 13%) than lower (1-back: M = 97%, SD = 5%) load. There was no main effect of Group (F(1, 56) = 1.80, p = 0.19, ηp 2 = 0.02); however, the interaction (F(1, 56) = 4.0, p = 0.05; ηp 2 = 0.04) indicated lower accuracy in the obese than nonobese group for the high, but not low load (Table 2).
RTs showed a main effect of Load (F(1, 56) = 12.8, p < 0.01; ηp 2 = 0.13) with slower responses in the higher (2-back: M = 709 ms, SD = 142 ms) than lower (1-back: M = 641 ms, SD = 141 ms) load, but did not show a main effect of Group (F(1, 52) = 1.74, p = 0.10, ηp 2 = 0.02) or interaction (F(1, 56) = 0.39, p = 0.53, ηp 2 < 0.01, Table 2). Together, these results indicate that working memory accuracy, but not speed, was sensitive to obesity, particularly under more demanding conditions.
Parent Report Questionnaires
Executive function
Children with obesity had higher scores on both BRIEF indices (BRI: F(1, 100) = 3.85, p = 0.05, ηp 2 = 0.04; MI: F(1, 100) = 4.32, p = 0.04, ηp 2 = 0.04), indicating worse parent-reported everyday executive functioning relative to children without obesity.
Sleep health
Despite no difference between groups for hours slept, obesity was associated with higher CSHQ scores (β (se) = 7.64 (2.07), t = 3.69, p < 0.01), indicating sleep health was worse in children with obesity relative to those without obesity (Table 1).
Psychopathology
Obesity status was not related to risk for Externalizing symptomology on the CASI (β (se) = 0.66 (0.70), z = 0.95, p = 0.34). However, children with obesity experienced 4.27 greater odds of scoring above the At Risk/Clinically Significant cutoff for Internalizing symptoms on the CASI relative to children without obesity (β (se) = 1.45 (0.64), z = 2.30, p = 0.02).
Mediation Analyses
Neither CSHQ nor internalizing symptomology was associated with performance during 2-back (CSHQ: β (se) = −0.002 (0.001), t = −1.05, p = 0.29; Internalizing: β (se) = 0.02 (0.05), t = −0.37, p = 0.72) or response consistency (CHSQ: β (se) = −0.01 (0.02),
Separate multiple mediation models, including age, gender, and parental education as covariates, were conducted for BRI and MI scores (Fig. 1A, B). The covariance between CSHQ total score and Internalizing symptom category was equivalent for both mediation models (cov (se) = −0.61 (0.30), z = −2.04, p = 0.04). Despite significant covariance, both mediators showed significant indirect effects for BRI (CSHQ: β (se) = 3.05 (1.41), z = 2.16, p = 0.03; Internalizing: β (se) = 3.46 (3.46), z = 2.38, p = 0.02) and MI (CSHQ: β (se) = 3.20 (1.44), z = 2.22, p = 0.03; and Internalizing: β (se) = 2.84 (1.32), z = 2.15, p = 0.03). There were no differences in the strength of the indirect effects of the two mediators (BRI: β (se) = −0.42 (2.06), z = −0.20, p = 0.84; MI: β (se) = 0.36 (2.01), z = 0.18, p = 0.86). The direct effects between obesity status and worse scores on BRIEF indices became nonsignificant after inclusion of the mediators (Fig. 1A, B); thus, the presence of poorer sleep heath and At Risk/Clinically Significant levels of Internalizing symptoms mediated effects of obesity status on executive functioning as measured by parent report of everyday behavior.
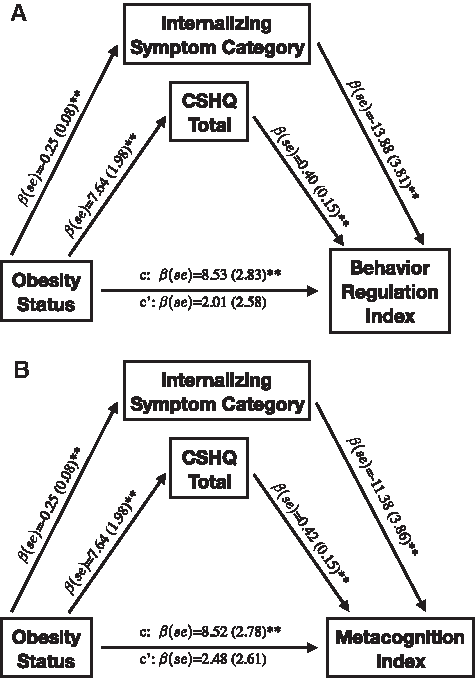
Separate multiple mediation models are depicted for the (A) Behavioral Regulation and (B) Metacognitive Indices of the Behavioral Rating Inventory of Executive Function. All reported coefficients are standardized. **p < 0.01. CSHQ, Child Sleep Habits Questionnaire.
Discussion
Pediatric obesity was associated with impairment in select components of reward-related decision-making and executive functioning with poorer sleep health and greater risk of internalizing psychopathology, mediating everyday executive behavioral deficits. Children with obesity did not differ for reward-related decision-making outcomes or sensitivity to monetary reward, but showed reduced ability to adapt behavior to changing reward contingencies. While inhibitory performance did not differ, children with obesity showed executive dysfunction under higher working memory demands and in everyday behavioral regulation and metacognition. Parent reports indicated that children with obesity had poorer sleep quality, despite equal sleep durations, and four times greater risk for experiencing internalizing psychopathology. Importantly, sleep health and internalizing symptoms mediated the deleterious effect of obesity on everyday behavioral regulation and metacognitive abilities, but not on decision-making and working memory performance. Our results highlight significant vulnerabilities for cognitive, sleep, and mental health of children with obesity, while elucidating a potential path through which obesity impacts everyday executive behaviors.
Children with obesity's decision-making performance were atypical in ways that could have significant impact upon the maintenance of their obesity status. The Bayesian decision-making model for the BART 24 had never previously been applied in studies of obesity and showed that despite lack of group differences in reward-related behavioral outcomes (i.e., number of pumps and pops), children with obesity showed responses that tended to be less sensitive to estimation of risk, suggesting decision-making that was less informed by one's own evaluation of risk/reward across trials. Such nuanced examination of decision-making may explain why tasks similar to the BART (e.g., Door Opening task and Hungry Donkey Task) have mixed findings, with some showing greater reward sensitivity in pediatric obesity,16,36,37 while others have not,17,38,39 as a tendency to make decisions that are inconsistent with own reward/risk evaluation may not be consistently captured in observable outcomes. Identifying specific reward-related biases in obesity is important for guiding prevention/intervention efforts.
Performance-based and ecologically relevant examination of executive function revealed impairments that may negatively impact academic achievement and social interaction. Unlike past findings using auditory stop signals,16,40 we did not observe group differences using visual stop signals. It is possible that inhibitory control is more challenging under cross-modal conditions (i.e., auditory stop signal and visual go cue), suggesting that response inhibition deficits may only be seen under more challenging demands. Indeed, impairment in dynamic working memory in children with obesity was limited to the higher load condition in this study. These results were not an effect of the wide age range of the sample as age was included as a covariate. Past studies show mixed findings using span tasks, which require active maintenance without dynamic updating.13,17,41 Dynamic working memory correlates with academic performance and is highly predictive of overall intellectual function 42 ; we controlled for IQ; thus, the observed deficit was above and beyond that accounted for by general intelligence. Assessment of everyday behavior with the BRIEF revealed that children with obesity were more likely to exhibit impairment on the Behavioral Regulation factor (i.e., inhibitory, emotion regulation, and set switching) and the Metacognition factor (i.e., working memory, planning, organization, and monitoring abilities). 43 Working memory, behavioral regulation, and metacognitive executive deficits are likely to interfere with academic achievement as well as social interaction. 44
Parent-reported sleep health and psychopathology accounted for significant variance in the observed effects of obesity on executive functioning. Worse sleep quality and greater odds of clinically relevant internalizing symptomatology in children with obesity, as observed in this study, are consistent with previous studies.4,45–47 Both factors, however, are associated with executive functioning, independent of obesity. Association with sleep 19 may stem from repeated deprivation of oxygen during sleep apnea and/or from attention problems induced by daytime sleepiness. Internalizing symptoms are defined as overregulated behavior and are highly comorbid with disorders of executive function such as attention deficit hyperactivity disorder. 21 In this study, both sleep health and internalizing symptomology significantly mediated the effect of obesity on executive functioning expressed in everyday behaviors, but not in performance. The chronic effects of poor sleep and internalizing symptomology may be more readily apparent in spontaneous behavior over time rather than in a laboratory setting where children can muster the motivation to overcome attention problems for the short duration of the task. Further experimental work, including intervention designs, is needed to disambiguate the causal relationhips between obesity, sleep health, internalizing psychopathology, and executive function.
Interpretation of the results is constrained by three challenges that are not specific to this study. First, the effect of obesity is confounded by lower SES and intellectual functioning, both of which covary with lower executive function and worse psychological well-being, independent of obesity status. We controlled for these statistically with well-accepted proxy measures, namely parental education for SES and full scale IQ for intellectual function. Parental education was chosen because it is associated with cognitive development 48 and has been more consistently associated with pediatric obesity 49 than family income levels. Second, whether our results relate to causes or consequences of obesity cannot be discerned by this study design. Children were not undergoing treatment for diabetes; however, presence of undiagnosed cases cannot be ruled out. Physiological factors associated with obesity such as brain inflammation due to increased free fatty acids 50 and insulin dysregulation 51 could negatively impact neuronal functioning in frontal lobe regions, 50 which are important for decision-making and executive function and promote the development of depression. 52 Study designs that manipulate inflammatory/metabolic functioning (i.e., comparison before and after weight loss) are necessary to disambiguate cause versus consequence of obesity on cognitive and psychological function. Last, psychopathology was measured with parent report, which is thought to be more valid in younger children than in adolescents, particularly for internalizing symptoms. Self-report measures would be important to include in future work.
Results underscore the importance of early intervention and prevention, as cognitive deficits likely worsen as cognitive and social adaptive demands increase with age. Worse reward-related decision-making and risk for internalizing disorders are particularly important during adolescence, when social influence on risk-taking behavior and risk for developing psychopathology is highest. 53 In addition, depressive symptoms have been shown to contribute to persistence of obesity in adolescence, 54 highlighting the importance of understanding the causal relationships between internalizing symptoms, obesity, and executive functioning. While our findings should be replicated with objective assessment of sleep health, they suggest that at least some aspects of executive dysfunction in obesity could be alleviated by improving sleep health and psychopathology.
Acknowledgment
Georgetown University Institutional funds.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.